
Abstract
Case Report
A previously healthy 14-year-old boy presented with mild chest pain that occurred 9 hours before. He was normal until he experienced acute-onset mild retrosternal chest pain when he performed a gymnastic backflip at school. The pain was continuous, did not change with body movements, increased with deep inspiration, and was associated with slight shortness of breath. He was able to continue gymnastic activity after symptom onset. He had no history of neck, back, and arm pain; nausea; vomiting; or loss of consciousness. He rated the maximum pain as 4 on a scale of 0 to 10, with 10 indicating the severest pain. He had never smoked or used illicit drugs. He visited the clinic because the pain had slightly worsened after dinner.
On examination, he was not in acute distress. He could walk and talk despite his symptoms. His vital signs were as follows: heart rate, 69 beats per minute; respiratory rate, 16 breaths per minute; blood pressure, 108/57 mm Hg; body temperature, 37.2°C; and oxygen saturation, 98% while breathing ambient air. The results of complete physical examination were unremarkable. He did not have a subcutaneous emphysema in the neck. The breath sounds were clear to auscultation bilaterally. Apex beat was located within the normal range. Cervical crepitation, Hamman’s sign, pleural friction rubs, and pericardial friction rubs were absent.
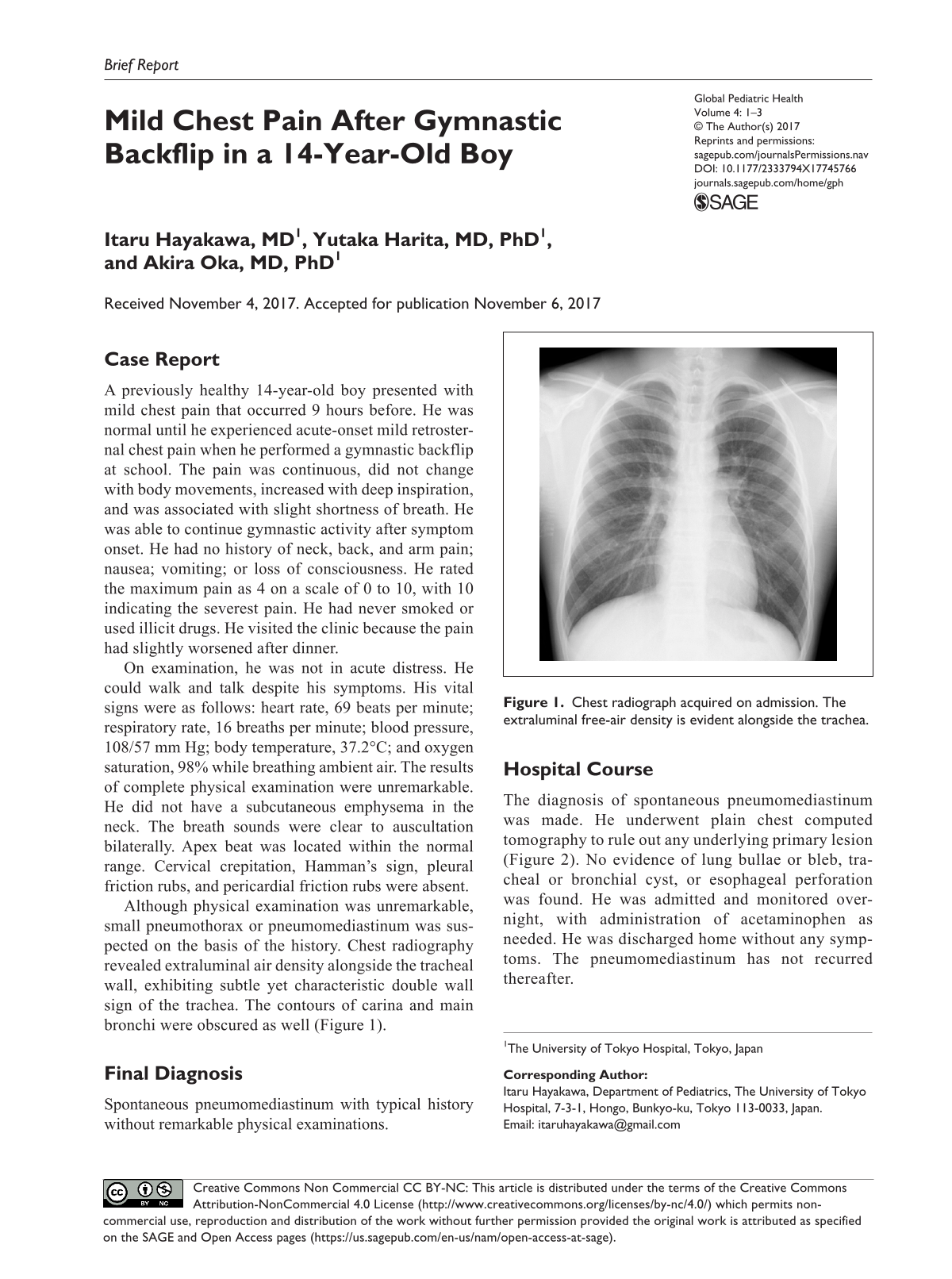
Although physical examination was unremarkable, small pneumothorax or pneumomediastinum was suspected on the basis of the history. Chest radiography revealed extraluminal air density alongside the tracheal wall, exhibiting subtle yet characteristic double wall sign of the trachea. The contours of carina and main bronchi were obscured as well (Figure 1).

Chest radiograph acquired on admission. The extraluminal free-air density is evident alongside the trachea.
Final Diagnosis
Spontaneous pneumomediastinum with typical history without remarkable physical examinations.
Hospital Course
The diagnosis of spontaneous pneumomediastinum was made. He underwent plain chest computed tomography to rule out any underlying primary lesion (Figure 2). No evidence of lung bullae or bleb, tracheal or bronchial cyst, or esophageal perforation was found. He was admitted and monitored overnight, with administration of acetaminophen as needed. He was discharged home without any symptoms. The pneumomediastinum has not recurred thereafter.

Computed tomographic image acquired on admission reconstructed for the coronal section. The extraluminal free-air is evident.
Discussion
Spontaneous pneumomediastinum is a rare and often missed diagnosis. The incidence of pneumomediastinum is only 1 in every 12 850 admissions.1 -4 The incidence in the general population is not known, but it is estimated to be much less than the incidence of pneumothorax (7.4-18 cases/100 000 persons per year), 5 an important differential diagnosis of pneumomediastinum in the emergency setting. The 2 leading complaints of spontaneous pneumomediastinum are sudden-onset chest pain and shortness of breath. These symptoms are frequently accompanied by history of exertion, cough, or upper respiratory tract infection.1 -4
Pertinent positive physical examination findings include cervical emphysema, cervical crepitation, Hamman’s crunch (a crunching or rasping sound synchronous with the heartbeat), 6 and friction rubs. However, in one retrospective cohort study, as many as 5 in 16 patients with spontaneous pneumomediastinum exhibited unremarkable findings on physical examination. 1 Pneumomediastinum with unremarkable physical examination findings is challenging to diagnose and may easily be missed in the emergency departments and primary care clinics, especially when the symptoms are relatively mild. Detailed history taking on possible precipitating factors before the onset of chest pain and plain chest radiography are keys to diagnosing patients with these symptoms.
Chest radiography reveals signs of the presence of extraluminal free air within the mediastinum. 7 The free air alongside the trachea or bronchus, posterior pericardium, pulmonary artery, and aortic branches is known as tracheal or bronchial double wall sign, continuous diaphragm sign, ring-around-the-artery sign, and tubular artery sign, respectively. In our case, the double wall sign of the trachea led to an early diagnosis. Since complications of this disease are often the consequence of hidden causes of pneumomediastinum, “probable primary” pneumomediastinum warrants further inspection of the underlying cause, such as occult lung bullae, lung bleb, asymptomatic tracheal/bronchial tumor/cyst, or hidden esophageal perforation, by computed tomography. None of these were found in our case.
Here we encountered a case of mild spontaneous pneumomediastinum with unremarkable physical examination findings. Subtle radiographic abnormality as well as distinctive history led to an early, and otherwise missed, diagnosis. Careful history taking and meticulous inspection of radiographs are keys to prompt diagnosis and management of spontaneous pneumomediastinum.
Conclusion
Careful history taking and meticulous inspection of radiographs are keys to diagnose physical-negative mild spontaneous pneumomediastinum.
Footnotes
Author Contributions
IH: Contributed to conception and design; contributed to interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
YH: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AO: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.