
Abstract

Case Report
A 2-month-old female was seen in our emergency department for evaluation of a congenital infection. During pregnancy, mother was routinely screened for human immunodeficiency virus (HIV) and syphilis in the first trimester and tests results were negative. Throughout the entire pregnancy, mother had regular prenatal care at scheduled visits. She presented to her obstetrician at 28 weeks gestation with generalized skin lesions on palms and soles, as well as a painless lesion in her genital area. At both the 28-week and 36-week prenatal visits, she was referred to dermatology, and mother was subsequently treated with topical hydrocortisone cream. No further workup was done. Two months after delivery, mother followed up with her primary care provider due to lack of resolution of skin lesions. At that time, a sexually transmitted infection was suspected and mother was tested for syphilis, and rapid plasma reagin (RPR) came back positive at 1:128. Infant was referred for further workup.
On presentation, physical exam of the infant was significant for desquamation of the skin on the bilateral soles of her feet, pinpoint pink dots on the soles of her feet bilaterally, and a erythematous skin lesion 1 × 1 cm on her right medial knee. Mother did report that infant was not moving her left leg. Infant did not exhibit any neurological deficits on physical exam. Significant laboratory findings included slight anemia, hemoglobin of 8.9 g/dL, and hematocrit of 26.5%. Further workup for congenital infection was done including lumbar puncture. All findings in the cerebrospinal fluid in this patient were within normal limits, including normal cell count, glucose, and protein. Venereal disease research laboratory (VDRL)tests was negative as well. Long-bone radiographs were also done, which were significant for osteochondritis and periostitis. This was seen in the medial metaphysis of the proximal left tibia and distal left femur (Figure 1A), the metaphysis of the medial right proximal tibia, and in the distal left ulnar metaphysis (Figure 2A).

(A) X-ray of left tibia/femur before treatment.
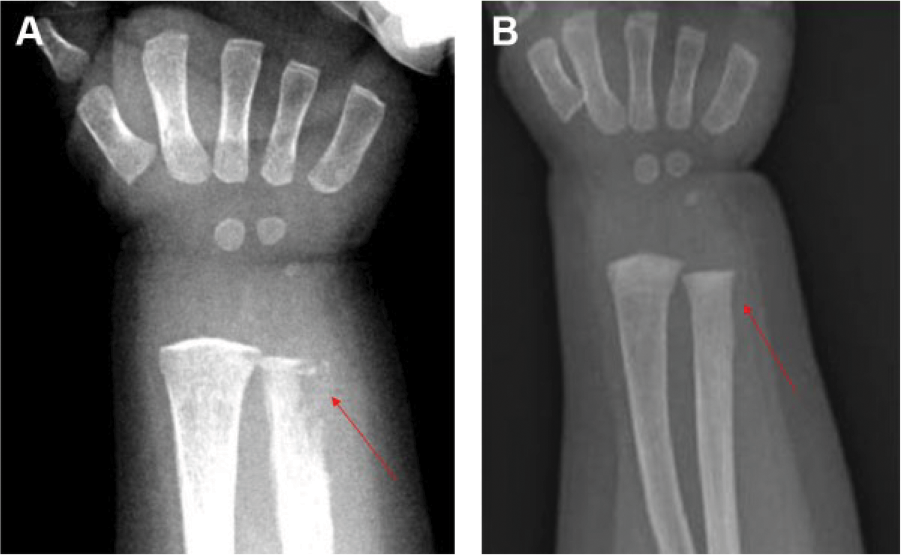
(A) X-ray of left ulna before treatment.
Hospital Course
Infant was tested and had positive syphilis tests: RPR titer 1:128 and enzyme immunoassay test >70 index.
Infant was subsequently treated with intravenous (IV) aqueous crystalline penicillin G (50 000 units/kg) every 4 hours for a 10-day course. 1 Repeat long-bone radiographs were done 2 months after completing treatment and showed complete resolution of bone findings (Figures 1B and 2B). Repeat RPR titer was done 2 months after treatment, which showed a titer of 1:8, which is greater than a 4-fold decrease from the initial titer of 1:128, indicative of successful response to treatment. 2 RPR titer was repeated 4 months after treatment, which was further decreased to 1:4.
On further investigation, father was found to be the source of infection, and both parents were subsequently treated for syphilis with 3 weekly intramuscular penicillin G benzathine.
Final Diagnosis
Missed diagnosis of symptomatic secondary syphilis in a pregnant women, subsequently resulting in an infant with congenital syphilis with significant bone findings of osteochondritis and periostitis.
Discussion
Syphilis is caused by Treponema pallidum, a long, motile, spirochete. Congenital syphilis is an intrauterine infection acquired from an infected mother via transplacental transmission of T. pallidum at any time during pregnancy or less frequently at birth from contact with maternal lesions. 2 Among women with untreated early syphilis, as much as 40% of pregnancies result in spontaneous abortion, stillbirth, or perinatal death. 2 Rate of transplacental transmission is 70% to 100% during primary and secondary syphilis and decreases with later stages of maternal infection, approximately 40% with early latent infection and 10% with late latent infection. 3 Signs of early congenital syphilis include skin lesions, lymphadenopathy, hepatosplenomegaly, blood-stained nasal discharge, osteochondritis, and pseudoparalysis. 2 This infant had signs suggestive of pain in the extremities from syphilitic involvement of the bone, which is termed pseudoparalysis of Parrot. 4 Infant also had classical radiological findings suggestive of skeletal involvement in congenital syphilis, in which there was destruction of the medial proximal tibia, called Wimbergers Sign. 4
These clinical manifestations of congenital syphilis can be prevented with treatment of penicillin to infected mother during pregnancy. 5
Rates of congenital syphilis have decreased over the past 15 years due to increase in screening during pregnancy and subsequent treatment. In the state of Michigan, in 2003 there were a total of 34 cases of congenital syphilis. By the year 2015, there were a total of 11 cases of congenital syphilis, which is a 67% decrease in incidence of cases over the 12-year time span.
While the incidence of congenital syphilis has been decreasing, the incidence of primary and secondary syphilis has been increasing in the state of Michigan. In 2008, the total number of cases of primary and secondary syphilis was 216. By the year 2015, the total number of cases of primary and secondary syphilis increased to 401, which is a 46% increase. The numbers of cases of primary and secondary syphilis in females has been decreasing and the increase in incidence has been attributed to men having sex with men. In 2008, 27% of cases of primary and secondary syphilis were females, and 25% of the cases were men having sex with men. By the year 2015, 8% of cases of primary and secondary syphilis were females, and 72% of the cases were men having sex with men. (Data obtained from Michigan Department of Health and Human Services; Courtesy of Jim Kent, Sexually Transmitted Disease (STD) Epidemiologist.)
Guidelines vary on how frequent to screen for maternal syphilis, whether women should be screened only in the first trimester or also at 28 weeks and at delivery. For example, the Centers for Disease Control and Prevention 2015 Sexually Transmitted Disease guidelines state that screening for syphilis for all pregnant women should be at the first prenatal visit. 1 In addition, the Centers for Disease Control and Prevention guidelines state that for pregnant women living in communities and populations in which syphilis prevalence is high including women at high risk for infection, syphilis testing should be repeated in the third trimester at 28 to 32 weeks and again at delivery. 1 In the Michigan Department of Health and Human Services’ guidelines for screening for syphilis during pregnancy, it states that all women should be screened for syphilis in the first trimester and at 28 weeks and at delivery. 6
Although the incidence of cases of primary and secondary syphilis in females has been decreasing, there continues to be cases of mothers acquiring syphilis during the second and third trimesters as seen in this case. This case emphasizes the importance of screening pregnant women in high-risk areas for syphilis not only during the first trimester, but also at 28 weeks and at delivery. This strategy can decrease the incidence of congenital syphilis and its associated long-term sequelae. In addition, this case also underscores that syphilis should also be considered in all sexually active patients with unexplained skin rash.
The treatment of congenital syphilis in infants over 1 month of age is IV aqueous crystalline penicillin G 200 000 to 300 000 units/kg/day IV, given as 50 000 units/kg every 4 to 6 hours for 10 days. 1 The infant in this case who presented with significant osteochondritis and periostitis as seen on long-bone radiographs was treated with the routine duration of IV antibiotics of 10 days. This case highlights that congenital syphilis presenting with significant osteochondritis and periostitis can have complete resolution with the standard 10-day course of IV penicillin given for congenital syphilis, rather than the prolonged course of 4 to 6 weeks of antibiotics as required in other bacterial infections involving the bone, such as Staphylococcus aureus osteomyelitis.
Conclusion
This case illustrates the multiple missed opportunities for diagnosing syphilis in a pregnant woman, which subsequently resulted in a case of congenital syphilis. The first missed opportunity occurred when a pregnant, symptomatic woman presented with a generalized rash, despite receiving timely prenatal care. In addition, state guidelines for syphilis screening during pregnancy were not followed. Timely testing for syphilis during the first trimester and additional testing at 28 weeks and at delivery in high-risk areas, for all pregnant women, can decrease the incidence of congenital syphilis and its complications.
Author Contributions
SH: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JLL: Contributed to conception and design; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JYA: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.