
Abstract
Severe hypercalcemia in infants is usually attributed to genetic etiologies and less commonly to acquired ones. An 8-week-old girl presented with failure to thrive, mild respiratory distress, and life-threatening hypercalcemia (23.5 mg/dL). Serum 1,25(OH)2-vitamin D (1,25(OH)2-D) level was elevated and parathyroid hormone undetectable. Evaluation for genetic mutations and malignant etiologies of hypercalcemia was negative. Treatment with intravenous hydration, loop diuretic, and calcitonin failed to correct the hypercalcemia, which was subsequently controlled with bisphosphonate therapy. Due to progressive respiratory deterioration, a bronchopulmonary lavage was done on day 17 of her hospitalization disclosing Pneumocystis jiroveci infection. The subsequent immunological investigation showed no abnormalities. She was treated with trimethoprim/sulfamethoxazole resulting in gradual clearing of her lungs and normalization of serum 1,25(OH)2-D level. A year later, she remains healthy with normal biochemical parameters of mineral metabolism. We conclude that in a child with hypercalcemia with suppressed parathyroid hormone and elevated 1,25(OH)2-D, once the genetic etiology for elevated 1,25(OH)2-D and malignancy are ruled out, one should investigate closely for a chronic granulomatous disease. Among the latter Pneumocystis jiroveci pneumonia infection should be considered even in an immunocompetent child.
Introduction
In immunocompetent children, Pneumocystis infection is mild and may present as an upper respiratory tract infection. On the other hand, Pneumocystis is a life-threatening infection in children who are immunocompromised from conditions such as HIV infection, chemotherapy, corticosteroid therapy, transplantation, and primary immunodeficiency states.1,2 Few patients with Pneumocystis infection develop hypercalcemia caused by elevated 1,25(OH)2-vitamin D (1,25(OH)2-D).3-5 The latter is due to the fact that in chronic granulomatous conditions activated macrophages produce 1,25(OH)2-D dependent on the substrate, 25(OH)-vitamin D (25(OH)-D) availability, but is not regulated by feedback from calcium, parathyroid hormone (PTH), or 1,25(OH)2-D.6-9
In this report, we describe a 2-month-old immunocompetent infant who presented with nonspecific symptoms of failure to thrive and lethargy associated with life-threatening hypercalcemia that preceded by 2 weeks the development of Pneumocystis jiroveci pneumonia (PJP). The hypercalcemia was related to increased ectopic synthesis of 1,25(OH)2-D, which was aggravated by inappropriate vitamin D supplementation. The life-threatening hypercalcemia was corrected by bisphosphonate therapy, and normalization of serum 1,25(OH)2-D was achieved by treating the granulomatous disease with trimethoprim/sulfamethoxazole (TMP/SMX).
Case Report
The infant girl was born at full term with a birth weight of 4300 g via spontaneous vaginal delivery. She presented at 8 weeks of age for evaluation of failure to thrive, lethargy, and dehydration. The parents reported that she was taking 30 to 60 mL of expressed breast milk every 2 hours and vitamin D 400 IU/day, and having ~20 wet diapers/day. Her admission weight was 3710 g (2nd percentile), length 58.4 cm (60th percentile), and head circumference 39.0 cm (75th percentile). In the preceding 3 weeks, she had lost ~1 kg in weight. Her physical exam revealed no dysmorphic features, sunken anterior fontanelle, sunken eyes, anicteric sclera, and no skin rash. Her lungs sounded clear and she had normal heart rate and sounds without murmurs. The abdominal exam was benign without hepatosplenomegaly. Her extremities showed no deformities.
As shown in Table 1, on admission the laboratory evaluation showed serum calcium 24.3 mg/dL, ionized calcium (iCa) >3.30 mmol/L, undetectable PTH, creatinine 0.38 mg/dL, albumin 3.4 g/dL, and urine calcium/creatinine ratio 2.2 mg/mg. A repeat discussion with the family disclosed that the girl was erroneously receiving 4000 units/day of vitamin D instead of the prescribed 400 units/day. Serum 25(OH)-D was mildly elevated at 165 ng/mL (normal 30-100 ng/mL), and 1,25(OH)2-D was markedly elevated at 237 pg/mL (24-86 pg/mL). Additional evaluation for hypercalcemia showed normal serum PTH-related peptide, vitamin A, 24,25(OH)2-vitamin D level, alkaline phosphatase activity, no mutation in CYP24A1 gene, and normal gene microarray. On admission, the chest X-ray showed only mildly increased parahilar bronchial markings. Computed tomography of the chest, abdomen, and pelvis showed no tumors. Skeletal survey showed no lesions or metabolic bone disease. The renal ultrasound showed mildly enlarged echogenic kidneys (right 6.8 cm and left 6.0 cm).
Serum Calcium, Ionized Calcium, Parathyroid Hormone (PTH), 25(OH)-Vitamin D, 1,25(OH)2-Vitamin D, and Urinary Calcium/Creatinine Ratio at Presentation, During Active Therapy, and Follow-up in an Infant With Pneumocystis jiroveci Pneumonia a .
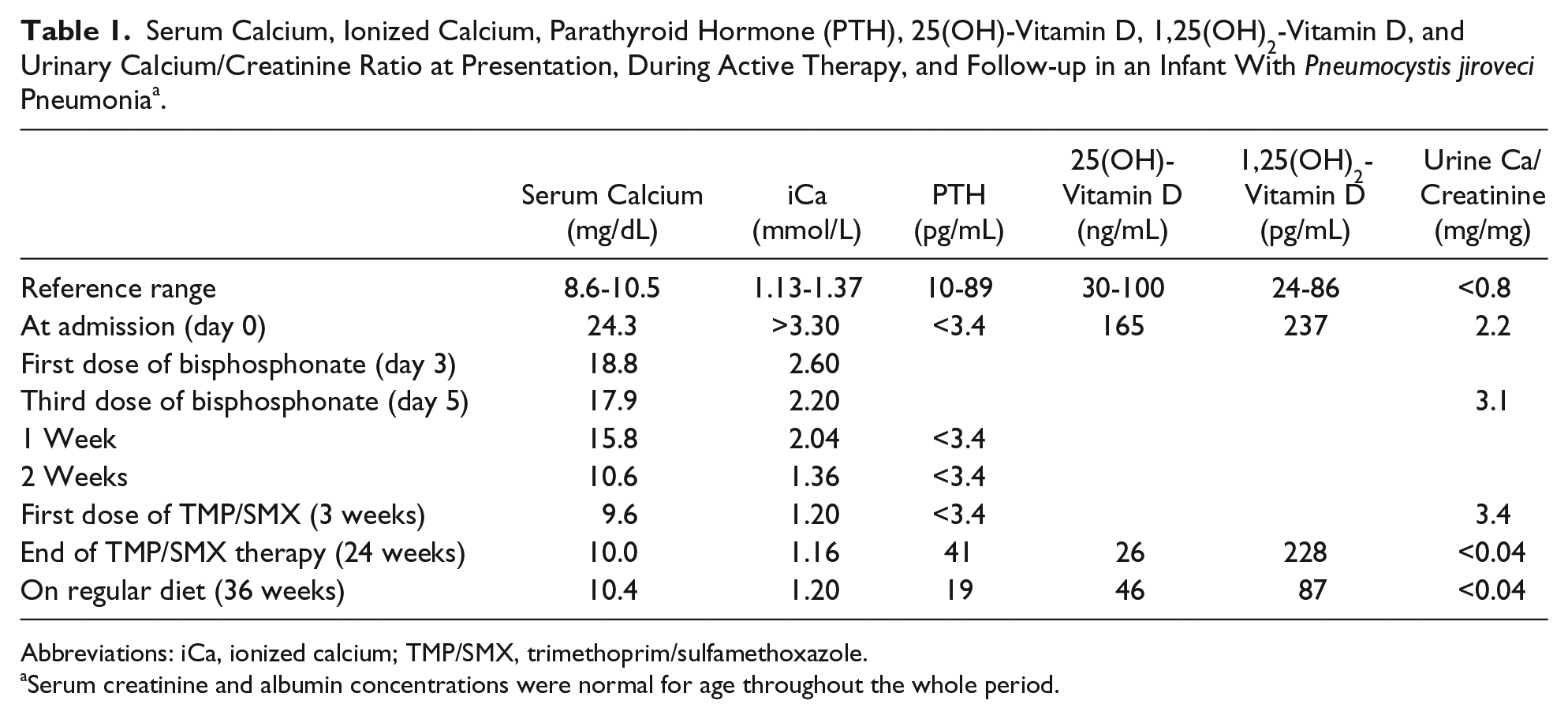
Abbreviations: iCa, ionized calcium; TMP/SMX, trimethoprim/sulfamethoxazole.
Serum creatinine and albumin concentrations were normal for age throughout the whole period.
The child received intravenous hydration, loop diuretic, and calcitonin for the life-threatening hypercalcemia. The vitamin D supplementation was discontinued, and she was placed on breast milk and low calcium and vitamin D free formula Calcilo XD (Abbott). At the end of 48 hours serum calcium had only decreased to 18.8 mg/dL. She was subsequently treated with zoledronic acid on 3 successive days (cumulative dose 0.375 mg). In the next 2 weeks serum calcium and iCa gradually decreased and normalized on day 15 (Table 1).
In the 2-week period following admission she experience gradual worsening tachypnea requiring supplemental oxygen, which progressed into respiratory distress. On hospital day 17, a chest computed tomography revealed a ground-glass appearance with interlobular septal thickening in both upper and lower lobes (Figure 1). A bronchoscopy with alveolar lavage and wedge lung biopsy was performed, which were both positive for PJP. TMP/SMX therapy was initiated on day 21 of her hospitalization. An immunologic workup (complete blood counts, peripheral smears, serum immunoglobulin levels, granulocyte oxidative burst test, T- and B-cell flow cytometry, in vitro T-cell function to mitogens, specific antigens, and allogenic lymphocytes) and genetic studies (microarray, T-cell/B-cell clonality by polymerase chain reaction) were all normal.

Chest computed tomography shows diffuse ground-glass and parabronchiolar septal thickening within the bilateral lower lobes.
At discharge, at 12 weeks of age, her respirations were normal and the lungs were clear to auscultation. She was sent home on TMP/SMX, and breast milk supplemented by Calcilo XD formula. She was treated with TMP/SMX for a total of 21 weeks. At 24 weeks of follow-up (Table 1), 25(OH)-D level had decreased to 26 ng/mL while serum 1,25(OH)2-D level was still high at 228 pg/mL. At 32 weeks Calcilo XD was changed to whole milk. On her last follow-up (36 weeks), she was taking regular diet without vitamin D supplementation. She appeared well and was developing appropriately. Her length was 80.8 cm (58th percentile), weight 10.3 kg (28th percentile), and head circumference 46.9 cm (62nd percentile). Serum calcium, iCa, 25(OH)-D and 1,25(OH)2-D, and urine calcium were in the normal range (Table 1). The skeletal survey was normal. The follow-up ultrasound showed normal kidneys (right 7.0 cm and left 6.9 cm).
Discussion
Our report highlights severe life-threatening hypercalcemia in an infant during the prodromal phase of PJP from increased 1,25(OH)2-D synthesis by macrophages, which was further aggravated by inappropriately high intake of vitamin D supplementation. Hypercalcemia in association with Pneumocystis infection was first reported in an infant in 1965 but was attributed to vitamin D toxicity. 10 Recently hypercalcemia in PJP has also been reported in recipients of kidney transplant receiving immunosuppressive therapy.4,5
Hypercalcemia occurs when there is an imbalance between calcium entry and exit from the blood from changes in gastrointestinal absorption, urinary excretion, and/or bone deposition or resorption. The etiology of hypercalcemia can be examined as conditions associated with elevated PTH versus those in which PTH is suppressed, and the latter can be further divided into conditions in which 25(OH)-D and 1,25(OH)2-D are normal or elevated. 3 Our patient had undetectable PTH, mildly elevated 25(OH)-D, and markedly elevated 1,25(OH)2-D concentrations. A consideration for hypervitaminosis D was made due to inappropriate intake of vitamin D supplementation, but generally in cases of vitamin D toxicity the serum levels of 25(OH)-D are >250 ng/mL, 11 and as shown in humans 12 and rats, 13 concomitant serum 1,25(OH)2-D concentration is either normal or only mildly elevated. Thus, hypervitaminosis D was not responsible for the life-threatening hypercalcemia in our patient.
The prohormones, ergocalciferol, and cholecalciferol are hydroxylated in the liver into 25(OH)-D by microsomal cytochrome P450 enzymes. This enzyme activity has no feedback control, and thus the serum 25(OH)-D level reflects body stores of the vitamin, which depend on dietary intake and sunlight exposure. The elevated 25(OH)-D in our case report can be explained by the inappropriately high vitamin D supplementation. The 25(OH)-D circulates bound to vitamin D binding protein and is delivered to the kidney and other tissues where it is hydroxylated to 1,25(OH)2-D. Both 25(OH)-D and 1,25(OH)2-D are catabolized by 24-hydroxylase enzyme into 24,25(OH)2-vitamin D and 1,24,25(OH)3-vitamin D, respectively. 14 In infants with idiopathic infantile hypercalcemia, mutations in CYP24A1 gene encoding the 24-hydroxylase enzyme lead to insufficient catabolism of 25(OH)-D and 1,25(OH)2-D, resulting in high serum levels of these metabolites and low levels of 24,25(OH)2-vitamin D. 14 Our case had neither a mutation in CYP24A1 gene nor low 24,25(OH)2-vitamin D level, thus excluding this entity as an etiology.
High serum levels of 1,25(OH)2-D, and subsequent hypercalcemia, have been described in granulomatous condition such as sarcoidosis, tuberculosis, and so on, resulting from increased activity of 1-alpha-hydroxylase by activated macrophages. 3 In contrast to the kidney, where production of 1,25(OH)2-D is tightly regulated by feedback from calcium, PTH, and 1,25(OH)2-D, it is not regulated in activated macrophages.6-9 The ectopic 1,25(OH)2-D production is substrate dependent, and hypercalcemia is more likely and severe with higher 25(OH)-D levels.6,7 The elevated 1,25(OH)2-D causes increased calcium absorption from the gut. 15 Since production of 1,25(OH)2-D is substrate dependent in activated macrophages, the smoldering PJP infection in our immunocompetent patient combined with inappropriate vitamin D supplementation, created a “perfect storm” for life-threatening hypercalcemia. On follow-up we noticed that despite adequate therapy for PJP, it took more than 30 weeks for serum 1,25(OH)2-D levels to normalize, likely indicating slow resolution of macrophage activity. Treatment should start with intravenous hydration, loop diuretics, and calcitonin, but with increased experience with bisphosphonates they should be considered early in the management of hypercalcemia.15,16 We have previously shown that these anti-bone resorption agents can be safely used in children. 16
In summary, in a child with hypercalcemia serum levels of PTH, 25(OH)-D, and 1,25(OH)2-D are of great help with the initial diagnostic workup. In a child with hypercalcemia with suppressed PTH and elevated 1,25(OH)2-D, once the genetic etiology for elevated 1,25(OH)2-D (CYP24A1 gene mutation) is ruled out, one should investigate closely for a chronic granulomatous disease. Among the latter PJP infection should be considered even in an immunocompetent child as hypercalcemia may occur during the prodrome, and more likely if the child is on vitamin D supplementation.
Author Contributions
JSV: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TS: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
USA: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Acknowledgements
We thank the child’s family for granting us the permission to publish her case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Sam and Helen Kaplan Research Fund in Pediatric Nephrology and the Eric McClure Research Fund in Pediatric Bone and Mineral Disorders.