
Abstract
Treatment outcomes for adolescents with multidrug-resistant tuberculosis are rarely reported and, to date, have been poor. Among 90 adolescents from Lima, Peru, 68 (75.6%) achieved cure or completion of treatment. Unsuccessful treatment was less common in the Peru cohort than previously described in the literature.
Introduction
Adolescents—defined by the World Health Organization (WHO) as persons between 10 and 19 years old—have unique health characteristics, behaviors, and outcomes compared with younger children or older adults. 1 Current tuberculosis (TB) reporting conventions, however, do not facilitate straightforward examination of this group. Subsets are often limited to adolescents 13 to 18 years old. 2 Alternatively, individuals less than 15 years old have been grouped into pediatric cohorts. 3 This framing may mask outcomes and risk factors that are particular to adolescents 10 to 19 years old as a whole.
Only two reports specifically examine the experience of adolescents 10 to 19 years old with drug-resistant TB (DR-TB). Both reported a high frequency of unsuccessful treatment outcomes. In a cohort of adolescents from Khayelitsha, South Africa, with DR-TB, 28 of 44 (63.6%) experienced either death, treatment failure, or loss to follow-up. 4 Unsuccessful outcomes among adults with multidrug-resistant TB (MDR-TB) from Khayelitsha were less frequent. 5 In a smaller observational cohort of 11 adolescent patients from Mumbai, India, with MDR-TB and human immunodeficiency virus (HIV) coinfection, three patients died prior to initiation of antiretroviral therapy or anti-TB drugs, one shortly after starting treatment, and three after being lost to follow up. 6 The 50% frequency of unsuccessful outcomes of adolescents from Mumbai who initiated MDR-TB treatment was also higher than that of their adult counterparts. 7
The elevated frequency of unsuccessful MDR-TB treatment outcomes in previously studied adolescent cohorts and the difference in frequency of unsuccessful outcomes compared with adults with MDR-TB from the same cities suggests that adolescents 10 to 19 years old may have unique risk factors for failure, death, or loss to follow-up. The specific predictors of unsuccessful outcomes are, however, unknown.
A large, well-characterized cohort of patients with MDR-TB from Lima, Peru, presents an opportunity to further examine treatment outcomes and associated patient characteristics in adolescents. Previous analyses of the Lima cohort have shown that MDR-TB treatment with regimens containing five-likely effect anti-TB drugs is associated with higher rates of sputum culture conversion 8 and decreased rates of failure, 9 relapse, 10 and death. 11 Using this data set, we performed a retrospective study to identify whether MDR-TB treatment outcomes in adolescents in Peru differ from other published cohorts of adolescents 10 to19 years old, and identify risk factors associated with these treatment outcomes. This report is the largest cohort of 10 to 19 year old adolescent patients with MDR-TB to date.
Methods
Study Population
This article reports on the outcomes for a subgroup of adolescents between 10 and 19 years old who were diagnosed with culture-confirmed MDR-TB in Lima, Peru. Patients were included in the present analysis if they began receiving individualized treatment for MDR-TB during the study period from February 1, 1999, to July 31, 2002.
The program and outcomes for the full cohort have been reported elsewhere. 12 In sum, MDR-TB treatment was administered to all patients using directly observed therapy, which was provided by local community health workers and National TB Program (NTP) nurses. Supervising physicians from the Peruvian NTP managed adverse events. Nutritional, psychological, and financial support was provided to patients on treatment.
Independent Variables
We assessed the association between death and available demographic variables, baseline indicators of disease severity, baseline comorbidities, and the extent of prior TB treatment. We also evaluated the association between death and receipt of treatment with five likely effective anti-TB drugs, including a fluoroquinolone and, in the intensive phase, an injectable agent. 11 An agent was classified as likely effective if the baseline phenotypic drug susceptibility test showed no evidence of resistance to a specific agent or, if drug susceptibility test was not available, the patient had less than 1 month of exposure to the drug prior to starting the MDR-TB regimen. Data on adverse effects from MDR-TB therapy were not available.
Outcome Definition
Standard definitions in place at the time of the parent study were used: cure, treatment completion, failure, death, default, and transfer out. 13 The primary outcome for analysis was death from any cause while on treatment. We also report the distribution of composite outcomes. Cure and completion comprised a successful outcome; unsuccessful outcomes were failure, death, and default.
Statistical Analysis
Among adolescents, we evaluated the frequency of baseline patient characteristics and MDR-TB treatment outcomes. We assessed the association of covariates with rate of death through univariate Cox proportional hazards analysis. Covariates associated with the outcome in univariate analysis (P ≤ .20) were considered as candidates for inclusion in the final multivariable model. Covariates retained in the final model were those associated with hazard of death (P ≤ .05). Gender was also retained because of a plausible connection to TB outcomes. When an outcome other than death occurred, data were censored at the time of that outcome. Multiple imputation was used to handle missing values for the multivariable analysis. Analyses were completed in SAS version 9.3.
Ethics Statement
The parent study was approved by the institutional review board at Harvard Medical School and by the Ministry of Health of Peru.
Results
A total of 90 adolescents between the ages of 10 and 19 years initiated their first MDR-TB treatment between February 1, 1999, and July 31, 2002. Baseline demographic characteristics and clinical characteristics are summarized in Table 1.
Distribution of Baseline Patient Characteristics Among Adolescents With MDR-TB in Lima, Peru (n = 90).

Abbreviations: MDR-TB, multidrug-resistant tuberculosis; XDR-TB, extensively drug-resistant TB; HIV, human immunodeficiency virus; BMI, body mass index; CDC, Centers for Disease Control and Prevention.
Patients from Northern Lima received treatment support that was programmatically different than patients from other areas.
Patients enrolled prior to March 1, 2001, were more likely to have received the standard category II retreatment regimen after failure of category I than patients enrolled after this date, when national policy changed.
Low BMI-for-age per CDC definitions 9 or a clinical assessment of malnutrition documented in the medical record.
Age-adjusted low hematocrit definitions from Hollowell et al. 13
Dyspnea or resting respiratory rate >26 breaths/min.
Isolate resistant to at least isoniazid, rifampin, fluoroquinolone, and injectable (kanamycin, capreomycin, or amikacin).
Resistance to the following 12 drugs or drug classes was tested: capreomycin, cycloserine, ethambutol, ethionamide, isoniazid, kanamycin or amikacin, para-aminosalicylic acid, pyrazinamide, rifampicin, streptomycin, first-generation fluoroquinolones (ciprofloxacin, ofloxacin), and later-generation fluoroquinolones (gatifloxacin, levofloxacin, moxifloxacin).
At least 1 of the following: cardiovascular disease, diabetes mellitus, hepatitis or cirrhosis, epilepsy/seizures, renal insufficiency, psychiatric disorder, having ever smoked, having ever used/abused a substance.
In all, 53 (58.9%) patients were male, and 37 (41.1%) were female. One patient (1.7%) had HIV coinfection, and none of the patients had baseline diabetes mellitus. Poor nutrition, defined either as low body mass index (BMI)-for-age per Centers for Disease Control and Prevention (CDC) 9 or by a clinical assessment of malnutrition documented in the medical record, was noted in 23 (29.5%) patients at the start of treatment. Two patients (2.5%) reported a history of substance abuse and 4 (5.0%) a history of smoking. It was found that 38 patients (44.2%) had bilateral and cavitary TB disease on chest X-ray at the start of therapy. Three patients (3.3%) had extrapulmonary TB disease. Three patients (3.5%) had laboratory-confirmed extensively drug-resistant TB.
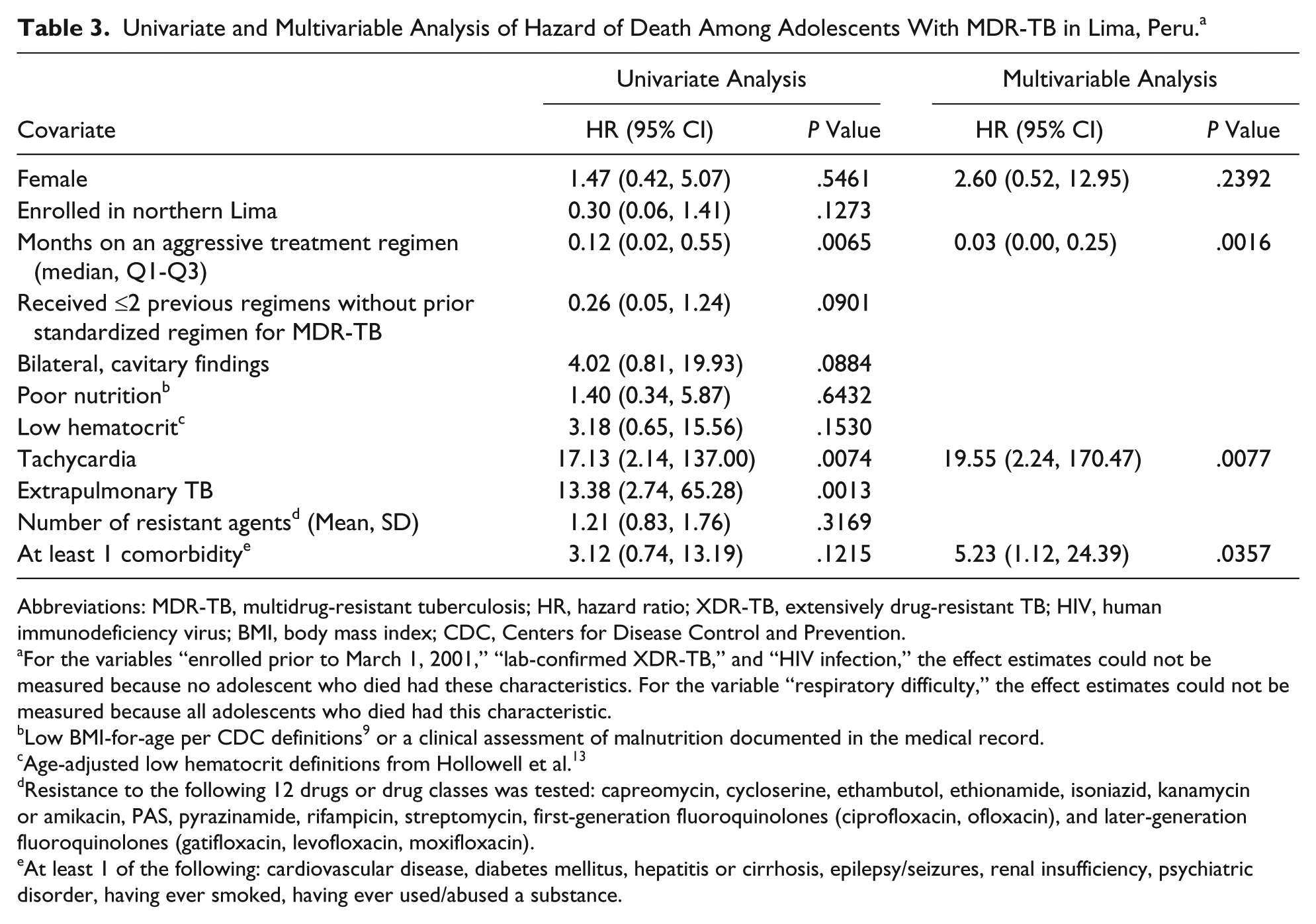
Successful treatment outcomes were achieved in 68 (75.6%) patients (Table 2). Ten patients died (11.1%). Treatment failed in three patients (3.3%). Eight defaulted (8.9%) and one (1.1%) transferred out. In univariate analysis, the rate of death was significantly associated with extrapulmonary TB (hazard ratio [HR] = 13.38; 95% CI = 2.74, 65.28) and tachycardia (HR = 17.13; 95% CI = 2.14, 137.0), whereas treatment with at least five likely-effective drugs was protective (HR = 0.12; 95% CI = 0.02, 0.55; Table 3). In multivariable analysis, the rate of death was associated with having at least one comorbidity (HR = 5.23; 95% CI = 1.12, 24.39) and tachycardia (HR = 19.55; 95% CI = 2.24, 170.47). Treatment with at least five likely-effective drugs remained protective (HR = 0.03; 95% CI = 0.003, 0.25).
Frequency of MDR-TB Treatment Outcomes Among Adolescents in Lima, Peru (n = 90).

Abbreviation: MDR-TB, multidrug-resistant tuberculosis.
Univariate and Multivariable Analysis of Hazard of Death Among Adolescents With MDR-TB in Lima, Peru. a
Abbreviations: MDR-TB, multidrug-resistant tuberculosis; HR, hazard ratio; XDR-TB, extensively drug-resistant TB; HIV, human immunodeficiency virus; BMI, body mass index; CDC, Centers for Disease Control and Prevention.
For the variables “enrolled prior to March 1, 2001,” “lab-confirmed XDR-TB,” and “HIV infection,” the effect estimates could not be measured because no adolescent who died had these characteristics. For the variable “respiratory difficulty,” the effect estimates could not be measured because all adolescents who died had this characteristic.
Low BMI-for-age per CDC definitions 9 or a clinical assessment of malnutrition documented in the medical record.
Age-adjusted low hematocrit definitions from Hollowell et al. 13
Resistance to the following 12 drugs or drug classes was tested: capreomycin, cycloserine, ethambutol, ethionamide, isoniazid, kanamycin or amikacin, PAS, pyrazinamide, rifampicin, streptomycin, first-generation fluoroquinolones (ciprofloxacin, ofloxacin), and later-generation fluoroquinolones (gatifloxacin, levofloxacin, moxifloxacin).
At least 1 of the following: cardiovascular disease, diabetes mellitus, hepatitis or cirrhosis, epilepsy/seizures, renal insufficiency, psychiatric disorder, having ever smoked, having ever used/abused a substance.
Discussion
Unsuccessful treatment outcomes were experienced by 24.4% of adolescents undergoing MDR-TB treatment in Lima, Peru, between 1999 and 2002, which was less frequent than unsuccessful outcomes seen in all-comers (32.8%) from the parent cohort. 12 Unsuccessful outcomes among adolescents in Peru were also considerably less frequent when compared with the two previously described adolescent cohorts in India and South Africa4,6
The lower frequency of unsuccessful outcomes between the Peru adolescent cohort and other adolescent cohorts may be a result of an unequal distribution of risk factors. Notably, the Peruvian cohort had only one patient with HIV and TB (1.1 %), whereas 100% of adolescent patients in the Mumbai cohort were coinfected. Given that HIV/TB coinfection has been associated with increased mortality, 15 it may be partially responsible for the higher number of deaths in the Mumbai cohort (36.3%) versus in the Peru cohort (11.1%). Additionally, adolescents had more frequent loss to follow-up in Khayelitsha (43.2%) and Mumbai (37.5%) than in Lima (8.9%).
Although HIV infection was not common in the Peru cohort, having at least one other comorbidity was associated with a hazard of death. We also found that tachycardia—a sign of advanced disease—was associated with a hazard of death. Adolescent TB is known to have other specific pathophysiological features, including an increasing risk for active disease following primary infection and more rapid progression to damage and cavitation of lung parenchyma.16,17 Further exploration of the effects of these adolescent TB disease characteristics on treatment outcomes is needed.
Our study has several limitations. First, it was a retrospective record review and is subject to all the biases inherent in such studies. Second, the sample size was small, limiting our ability to perform extensive multivariable analysis. Finally, the cohort described comes largely from urban Lima, with low reported substance use and no information on socioeconomic status or stigma. Consequently, our results may not be generalizable to adolescent populations with a different allotment of these risk factors that are presumed to be associated with outcomes of MDR-TB treatment.
With our analysis of 10 to 19 years old adolescent patients with MDR-TB, we have established that treatment outcomes for this group are not universally poor. We hypothesize that MDR-TB treatment with regimens consisting of five likely effective drugs offered through a community-based treatment program may have contributed to the relatively high frequency of successful treatment outcomes compared with other reports in the literature. Our findings underscore the need to better study adolescents with MDR-TB, paying careful attention to the age range that defines the group and the pathophysiological, socioeconomic, and behavioral risk factors that may determine treatment success.
Author Contributions
DBT: Contributed to conception and design; contributed to interpretation; drafted manuscript; gave final approval; agrees to be accountable.
MBM: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable.
JM: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable.
JJF: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable.
CDM: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.