
Abstract
The endoscopic STING procedure using Deflux is a common and minimal invasive treatment for vesicoureteral reflux. Herein we present the case of an 11-year-old girl with loin pain and de novo hydronephrosis and megaureter on the left. Ultrasound and plain abdominal X-ray demonstrated a calcification at the ureterovesical junction. She had been treated with Deflux injections 5 years before. The clinical quiz addresses the differential diagnosis, workup, and pathogenesis of calcifications at the ureterovesical junction following endoscopic reflux therapy.
Clinical Quiz
Case Summary
During a routine outpatient visit for dysfunctional voiding and reflux nephropathy, an 11-year-old girl reported recurrent colicky flank pain in the left loin, which had started several weeks before. There was no macroscopic hematuria or passage of a kidney stone, and the voiding pattern, after treatment of the voiding issues, was normal. The patient was known to have constipation and had stopped taking laxatives several months before. The past medical history was remarkable for recurrent urinary tract infections and vesicoureteral reflux grade III to the left and grade II to the right kidney for which she had undergone a STING procedure using dextranomer-hyaluronic acid (Deflux; Oceana Therapeutics Ltd, Dublin, Ireland) on both sides at the age of 5 and 6 years, respectively. The left kidney showed scarring with a split renal function of 38%. Following the second STING procedure, the reflux had resolved and the patient had no further urinary tract infections.
The physical examination was unremarkable, in particular no signs of constipation or tenderness in the left loin.
Urinalysis was unremarkable, and a urine culture was negative.
Renal ultrasound showed moderate left sided hydronephrosis with megaureter and an echogenic structure with acoustic shadow at the ureterovesical junction (UVJ; Figure 1a and b). This corresponded to a calcification in the left lower quadrant on abdominal X-ray (Figure 2).

Ultrasound of the left kidney (a) and bladder (b) showing hydronephrosis and an echogenic structure with acoustic shadow (+) at the left UVJ.

Plain abdominal X-ray demonstrating a radio-opaque structure in the left lower quadrant (arrow).
Questions
Taking into account her medical history, what should be considered in the differential diagnosis?
Which diagnostic tests would you consider?
Answers
Prevesical calculus or calcified Deflux depot.
Diagnostic tests to be considered include MAG3 scan Computed tomography scan Urethrocystoscopy with retrograde ureterography or ureteroscopy
Discussion
In the present case, colicky flank pain and de novo hydronephrosis with megaureter and a radiopaque structure at the UVJ suggested a prevesical ureterstone. In order to determine if the calcification was located in the ureteric lumen, a computed tomography (CT) scan was performed, which showed several calcifications at the level of the left UVJ of high density (>800 HU; Figure 3). However, it was not possible to discriminate between intra- or extraureteral position of the lesions. It was therefore decided to perform an urethrocystoscopy with retrograde ureterography, which documented patency of the distal ureter with bulging at the site of Deflux injection (Figure 4). Based on these findings, a diagnosis of a calcified Deflux deposit was made. On MAG3 scan the partial function of the left kidney was unchanged compared to an earlier DMSA scan, thus excluding significant obstruction. Without a specific intervention the dilation diminished with time, and the left-sided pain resolved after restart of laxatives. The hydroureter could reflect recurrence of reflux; still in the absence of urinary tract infections a new voiding cystourethrography was waived.
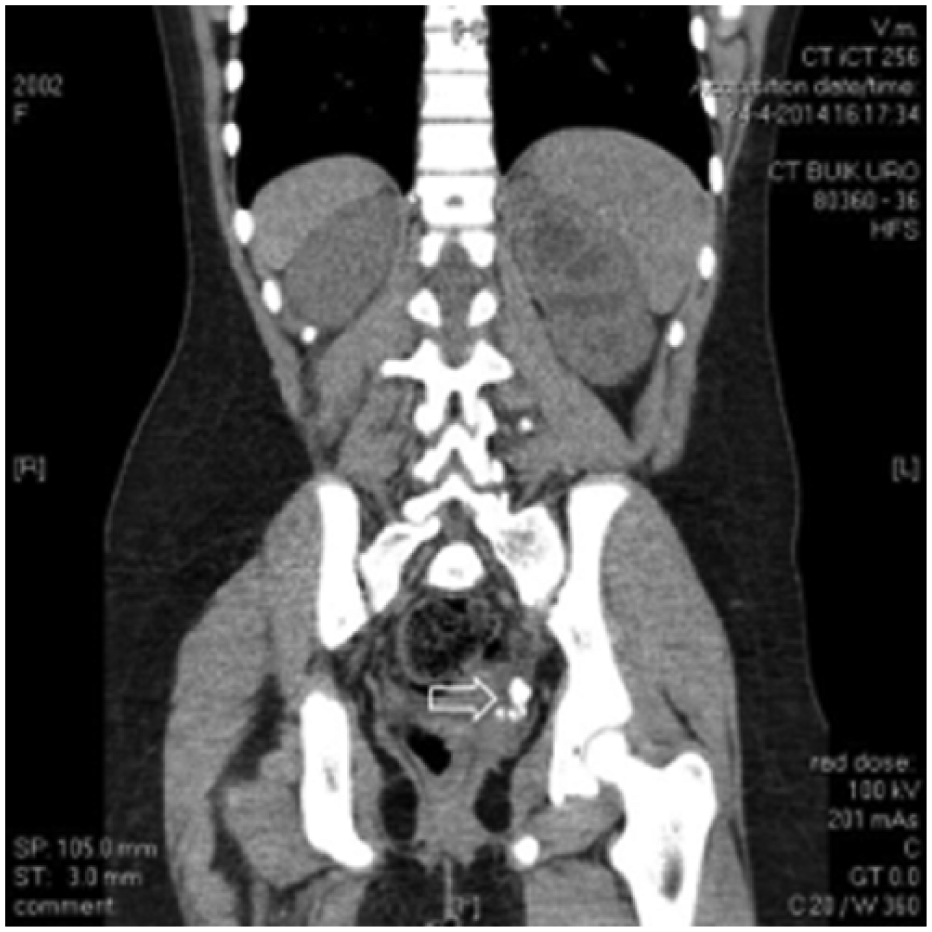
Abdominal CT without contrast showing several prevesical calcifications (arrow).
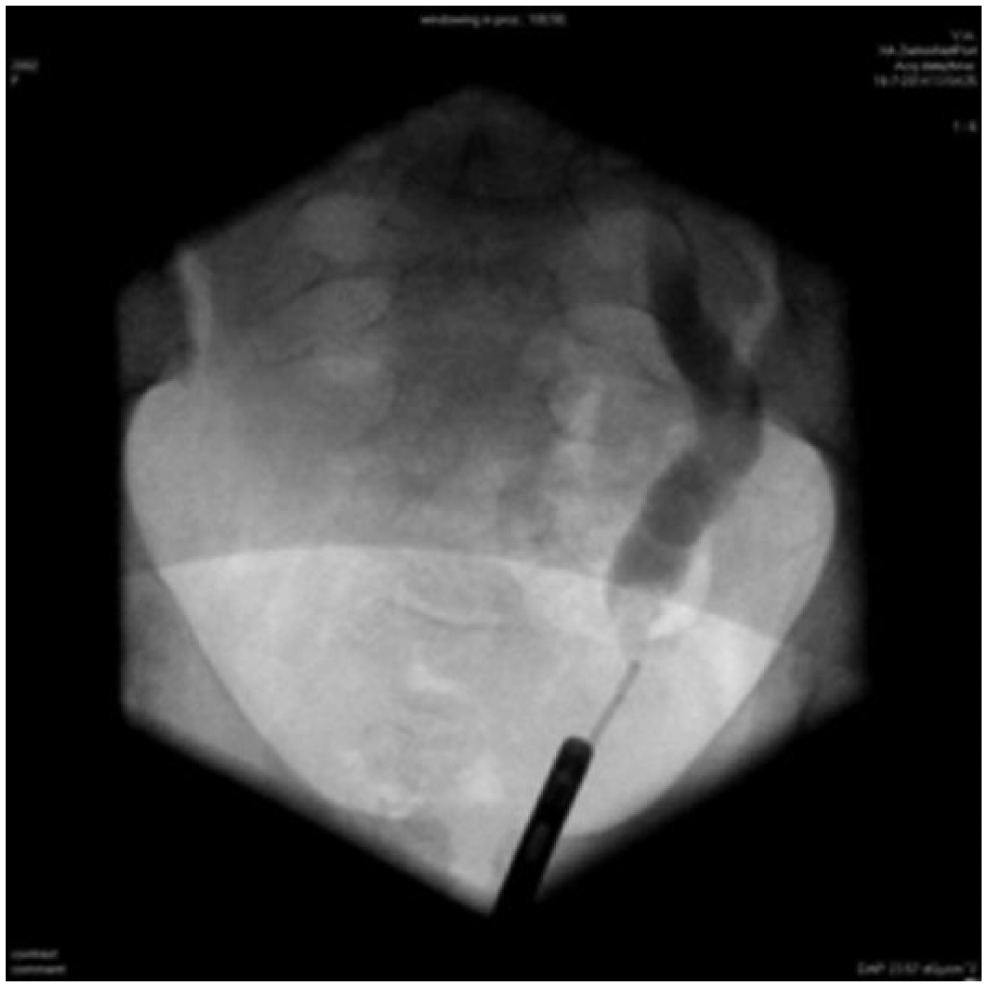
Retrograde ureterography.
The endoscopic STING procedure is a common and minimal invasive treatment for vesicoureteral reflux. From the beginning of the 1980s different substances have been used to create a mound at the VUJ including Teflon, bovine collagen, and autologous chondrocytes. 1 Use of these substances was problematic due to particle migration or lack of durability. First described in 1995, Deflux has become the most frequently used substance for this procedure. 2 A recent meta-analysis showed a success rate of reflux resolution ranging from 51% to 79%, with an inverse relationship between reflux grade and success rate.3,4 All implanted materials have the potential risk of foreign body reaction. Calcification has been described for Teflon, collagen, and autologous chondrocytes. In the systematic study by Gargollo et al, 1 mound calcifications were found in 37% of the patients at a median interval of 2.1 years after autologous chondrocyte injection. Initial animal studies suggested that Deflux injection was not associated with calcification. 5 However, since 2008 several cases of calcified Deflux deposits have been reported.6-10 In a study on 104 children undergoing annual ultrasound screening for up to 10 years after Deflux injection, mound calcification was observed in 2 of the patients after an interval of 4 years following the procedure. 11 Histologically, a foreign body reaction with granuloma formation, giant cells, and pseudo-encapsulation is found. 12 After a mean follow-up of 22 months after Deflux injection, some calcification was present in more than half of the implants. 12 CT is more sensitive than ultrasound to detect implant calcification. The density increases with time and eventually equals that of a calcium oxalate stone. 13 Of note, some small calcifications were also present at the right UVJ in our patient, which were not visible on ultrasound.
As in the present case, differentiation between a ureter calculus and a calcified Deflux mound may be challenging.6-10 As pointed out by Kirsch, 14 absence of hydronephrosis and hematuria with a history of a STING procedure should provide reassurance and prevent inappropriate intervention for misdiagnosed ureteral stones. In the presence of hydronephrosis, however, additional diagnostic tests have to be considered. 1 In the series reported by Yankovic et al, 7 out of 11 patients underwent urethrocystoscopy. 11 In all cases no calculus was found, but a bulge was seen at the location of the Deflux injection in accordance with the findings in our patient.
In general, calcified Deflux mounds do not require surgical intervention. To the best of our knowledge, only one patient has been reported with significant obstruction 63 months after a STING procedure with massive periureteral calcification requiring ureter reimplantation. 15
In conclusion, calcification of a Deflux mold is a well-documented complication that needs to be differentiated from a prevesical ureteric stone. Arguments in favor of an extraureteral calcification are the absence of hematuria or hydronephrosis and a time lag of several years after the STING procedure. When calcification of a Deflux depot is likely, close surveillance without invasive diagnostics is warranted.
Author Contributions
SK: Contributed to conception and design; contributed to analysis and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
EHVDH: Contributed to interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JIMLV: Contributed to interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AB: Contributed to conception and design; contributed to analysis and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.