
Abstract
The incidence of Kawasaki disease in Maghreb countries is apparently low, unlike those living in the province of Quebec, Canada. This retrospective study compared Maghrebi children living in Quebec to the countries of origin, Morocco, Algeria, and Tunisia. The annualized incidence rate in Quebec (18.49/year/100 000 children under 5 years of age) was 4 to 12 times higher than in Tunisia, Morocco, and Algeria (0.95, 4.52, and 3.15, respectively). The prevalence of incomplete diagnostic criteria was higher in Quebec at 39%, Morocco 43%, and Tunisia 39% compared to Algeria at 8%, with minimal delayed diagnosis (7%) only in Quebec compared to 30%, 35%, and 62%, respectively (P < .001). The rate of coronary aneurysms was comparable however (11% in Quebec vs 4%, 10%, and 25%, in Tunisia, Morocco, and Algeria, respectively; P = .31). The higher incidence of Kawasaki disease in the Maghreb community in Quebec versus the countries of origin seems due to underdiagnosis, which represents a public health concern in those countries.
Introduction
Kawasaki disease (KD) is a vasculitis primarily affecting children under 5 years of age 1 in more than 60 countries with variable incidence between countries and among ethnic groups. 2 The highest incidence is in Japan and in children of Asian origin. The incidence of KD in Arab countries and specifically in North African countries, also known as Maghreb, is unclear but reportedly low.3,4 A KD registry was conducted in the province of Quebec, Canada, where the number of immigrant Maghrebi children with KD appeared significant. Our study aims to determine the incidence of KD among Maghrebi children in Quebec in comparison to available reports from their countries of origin.
Methods
We conducted a survey in Quebec covering children with potential Maghrebi origins diagnosed with KD between 1996 and 2013. Clinical data were gathered from the medical charts. Additional data were assembled using a standardized questionnaire that was administered to patients’ parents (Appendix A). The study was approved by CHU Ste-Justine Research Review Board as a central committee for this collaborative study, and parental written informed consent was obtained. We compared epidemiological and clinical features of KD in Maghrebi children residing in Quebec to those reported in Tunisia, Morocco, and Algeria. Geographically and ethnically, the Maghreb countries include Morocco, Algeria, Tunisia, Libya, and Mauritania. Since there were virtually no Libyan and Mauritanian emigrants in Quebec during the study period, this specific population was not considered for comparison.
In Tunisia, data available between 1996 and 2013 were collected from 5 teaching hospitals for a doctoral project in medicine published in 2008, 5 with 3 additional patients diagnosed between 2007 and 2013. In Morocco, data were assembled between 2001 and 2009 from a doctoral project in medicine published in 2010 3 collected in the Hassan II teaching hospital, which handles all the Wilaya of Fez. In Algeria, data were collected between September 2005 and December 2008 from a doctoral thesis in medicine published in 2010 6 including 12 hospitals spread over 10 Wilayas. Familial cases of KD were assessed in the studies of Morocco and Algeria, but not in that from Tunisia.
Annualized incidence rate was calculated as follows: number of observed cases/annualized population under 5 years × duration of the study. For the calculation of the incidence rate, the standard denominator (SDenom) of 100 000 children under 5 years old was obtained from Statistics Canada for the Province of Quebec by country of origin for the following consecutive statistical periods (1996, 2001, 2006, 2011; Appendix B). The count of North Africans in Quebec was thus available on 3 series of 5-year intervals, 1996 to 2001, 2001 to 2006, and 2006 to 2011. The average annual population of children under 5 years was then calculated: [(Pop1996 + Pop2001/2) + (Pop2001 + Pop2006/2) + (Pop2006 + Pop2011/2)]/3; “Pop” being population of Maghrebi children under 5 years old residing in Quebec for the specific statistical year.
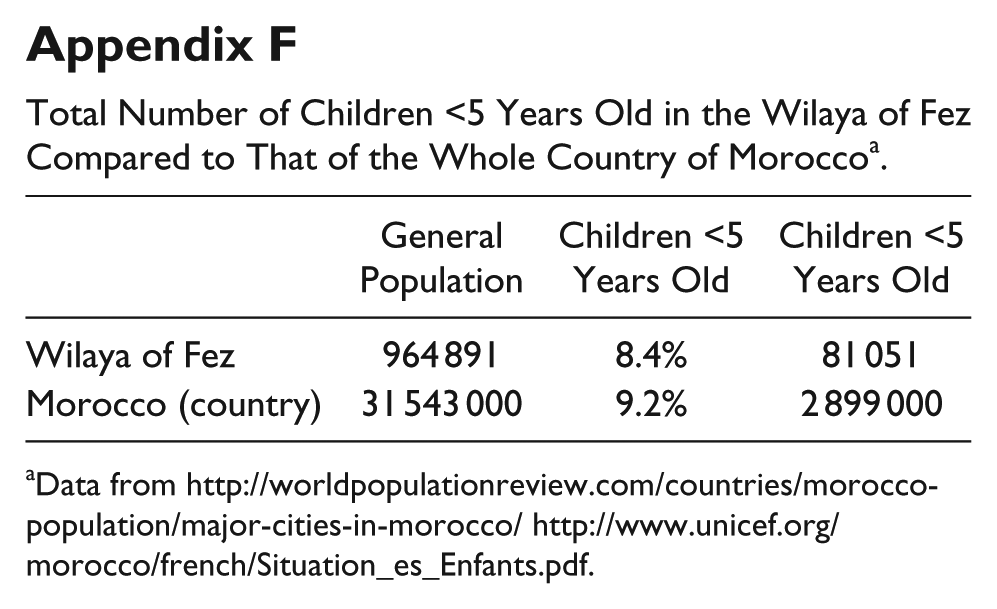
For North African countries addressed in the study, similar SDenom was dispensed from the Regional Directorate of Health in Nabeul, Tunisia (Appendix C), and from the National Office of Statistics in Alger, Algeria (Appendix D). The SDenom in the Wilaya of Fez, Morocco, was calculated based on the general population in that Wilaya where the published rate of children under 5 years old was 8.4% (Appendixes E and F).
Statistical Analysis
Descriptive statistics with ratios and percentages were compared with the χ2 or the Fischer tests for categorical data. Continuous data, mean ± standard deviation, were compared with the t test when data were normally distributed, or the U Mann-Whitney test otherwise. A P value <.05 was considered statistically significant.
Results
There were 34 potential Maghrebi patients identified in the province of Quebec during the study period, for whom consent was obtained from 28 (82%) with the following descent: Morocco 15, Algeria 11, and Tunisia 2. All cases were from the Montreal metropolitan area teaching and subsidiary hospitals. In Tunisia, 31 patients were identified, whereas 23 were identified in Morocco and 64 in Algeria.
From a demographic perspective, the proportion of patients younger than 5 years of age was 79% in Quebec, 70% in Morocco, 91% in Algeria, and 69% in Tunisia (P = .45). The average annual Maghrebi SDenom in Quebec was 8908, hence with an annual incidence rate of 18.49/SDenom (individual country of origin detailed in Table 1). Comparatively, in Tunisia, the Nabeul Pediatric Regional Hospital is the only hospital throughout the Governorate to evaluate children with KD, and the incidence was 0.95/SDenom (regional population of children under 5 years old of 58 071; Appendix C). In Morocco, Wilaya of Fez, 23 patients with KD were hospitalized between 2001 and 2009 at the Pediatric service of Hassen II hospital, with an incidence of 3.15/SDenom (regional population of children under 5 years old of 81 050 since 2004; Appendixes E and F). In Algeria, the Wilaya of Alger, there were 64 cases with an incidence of 4.52/SDenom (regional population of children under 5 years of age between 2006 and 2008 of 280 239; Appendix D). Compared to the countries of origin, the relative incidence of KD in Quebec varied between 4.05/1 and 12.42/1 (Table 1 and Figure 1). The age at KD diagnosis was comparable (3.3 ± 2.12 years in Quebec, 3.4 ± 2.16 in Morocco, 2.58 ± 1.58 in Algeria, and 4.1 ± 3.54 in Tunisia; P = .448), with a peak at 1 year of age in all 4 groups (Figure 2). A seasonal peak in the spring was observed in all groups, with a second peak in the winter in Algeria and in the summer in Tunisia (Figure 3).
Annualized Incidence Rate of Kawasaki Disease in the North African Community in Quebec With Comparison to the Countries of Origin.

Abbreviation: SDenom = standard denominator of 100 000 children <5 years old.
Wilaya of Fez, Morocco; Alger, Algeria; Governate of Nabeul, Tunisia.

Relative incidence among Maghrebi children in country of origin versus North American Province of Quebec.

Distribution of patients less than 5 years of age in the 4 series.
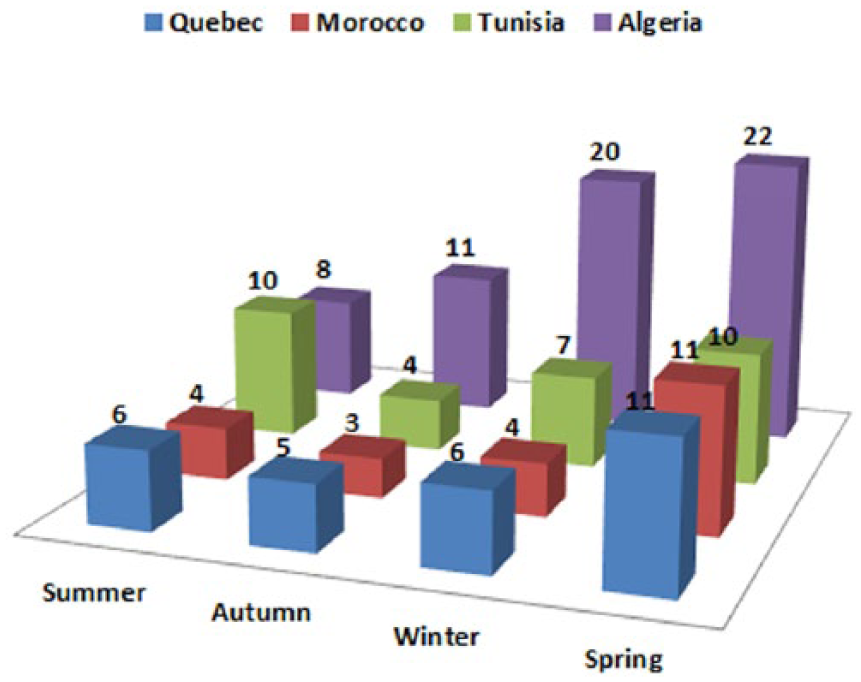
Seasonal patterns in the 4 countries.
In Quebec, there was a high frequency of atopic illnesses, with 12/28 (42.8%) personal history of asthma and/or allergy in addition to 20/28 (71.4%) of similar family history. This feature was not researched in the other 3 groups, however. Otherwise, infectious disease history was more frequent in Quebec, with 11/28 (39.3%) presenting an infectious illness preceding KD compared to 2 patients in the series from Tunisia and Algeria, and 1 from the Moroccan series (P < .001). In Quebec, autoimmune diseases were identified in the family history of 7/28 (25%) patients with one of them affected by several autoimmune diseases. This aspect, assessed only in the Morocco series, was negative for such medical history. Finally, consanguinity was reported in 4 cases in Quebec, but not in Morocco nor in Tunisia (P = .012), whereas consanguinity was not specified in the report from Algeria. Alternatively, one case among siblings was reported in Algeria, but not in Quebec, Morocco, or Tunisia.
The presenting features of the disease were comparable between Quebec and the countries of origin (Table 2), with the exception of the extremity changes that were less common in Quebec (P = .024). The incomplete form of the disease was less often (P < .001) reported in Algeria (5/64; 8%) compared to Quebec (11/28; 39%), Morocco (10/23; 43%), and Tunisia (12/31; 39%), with no statistical significance between Quebec and the latter 2 groups (P = .932). Diagnosis was made at 6.1 ± 2.5 days of fever [range 4-14] in Quebec, versus 9.7 ± 5.6 [5-30] in Morocco, 7.6 ± 4.2 [5-21] in Tunisia, and 13 ± 5.1 [5-21] in Algeria (P < .001), with a delayed diagnosis after 10 days of fever for 11/31 (35.5%) patients in Tunisia, 7/23 (30.4%) in Morocco, and 40/64 (62.5%) in Algeria comparatively to 2/28 (7.1%) in Quebec (P < .001). This diagnostic delay was significantly associated with incomplete KD in Morocco (P = .012) and in Algeria (P = .011), but not in Quebec (P = .64) or Tunisia (P = .34). In addition, diagnosis delay was significantly contributive in the development of aneurysms in Tunisia (P = .037) and Algeria (P = .003), but not in Quebec (P = .79) or Morocco (P = .30). Finally, laboratory investigations (Table 2) showed a statistically significant difference in thrombocytosis and elevation in hepatic transaminase in Quebec compared to the other groups (P < .001 and .043).
KD Clinical Criteria Distribution Among the 4 Comparative Series.
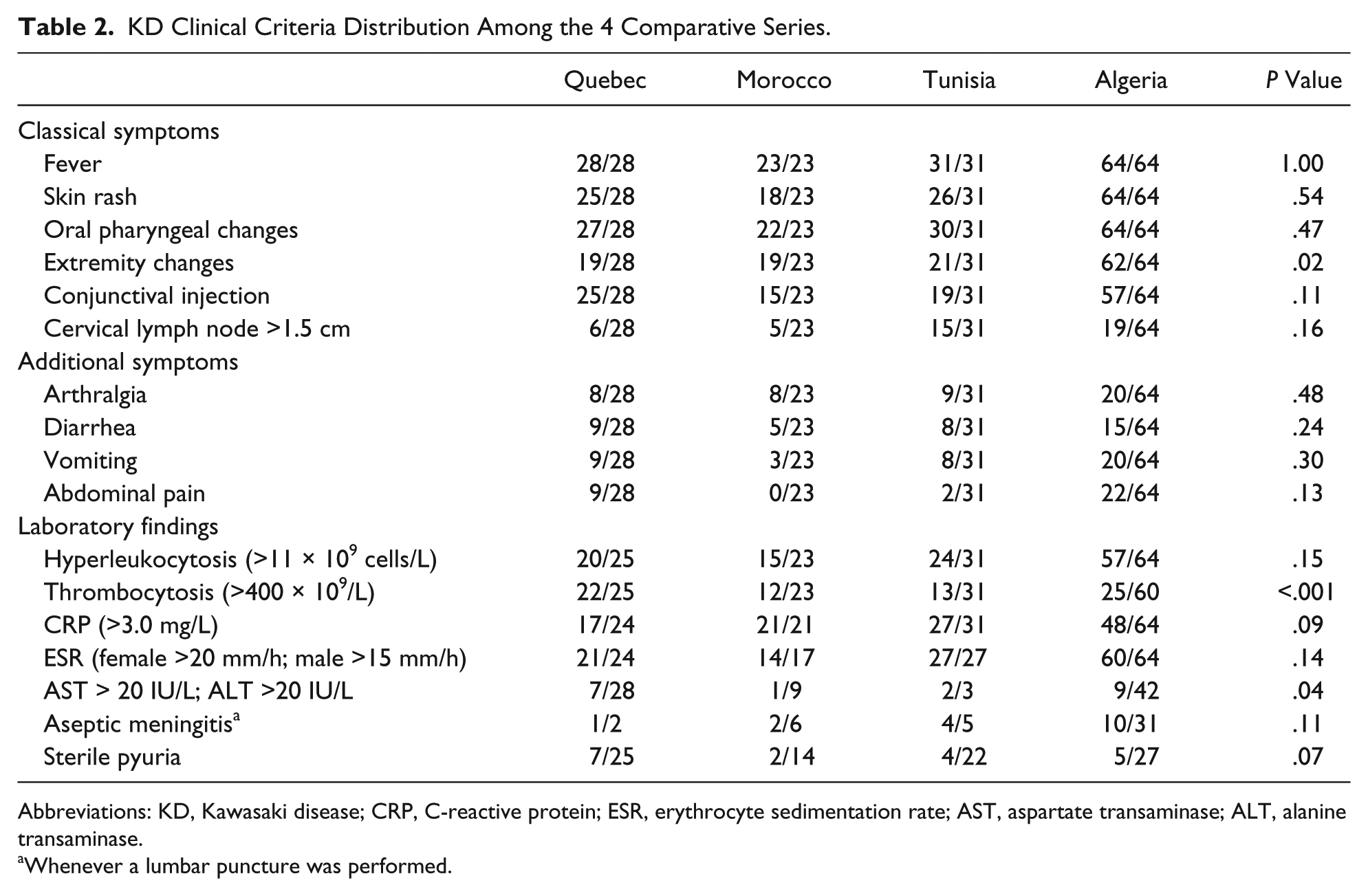
Abbreviations: KD, Kawasaki disease; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; AST, aspartate transaminase; ALT, alanine transaminase.
Whenever a lumbar puncture was performed.
From the therapeutic perspective, intravenous immunoglobulin (IVIG) was similarly (P = .14) administered to 100% of patients diagnosed in the acute phase in Quebec and 90% in Tunisia (28/31), compared to 5/23 (21.7%) in Morocco and 29/64 (45%) in Algeria (P < .001). In Quebec, 4 patients required a second dose of IVIG with appropriate response, whereas in Algeria 2 patients received a second dose of IVIG necessitating subsequent treatment with corticosteroids due to persistent unresponsiveness. The average duration of fever at the time of IVIG administration was 6 days in Quebec, 9 in Morocco, and 12 in Tunisia and Algeria (P = .021 Quebec vs Morocco, and P < .001 vs Tunisia and Algeria). Treatment with IVIG was administered after 10 days of fever in 1 case in Quebec, 1 case in Morocco, in 46% of cases in Tunisia, and in 59% in Algeria (P = .021).
Coronary artery lesions in general, that is, dilation and aneurysms, affected 11/28 (39%) patients in Quebec versus 5/23 (22%) in Morocco, 6/31 (19%) in Tunisia, and 17/64 (26%) in Algeria (P = .078). The rate of aneurysms was comparable between groups (3/28 [11%], 1/23 [4%], 3/31 [9%], and 16/64 [24%], respectively; P = .31). Aneurysms were ≥8 mm in 2 cases in Quebec with subsequent stenosis, 2 cases in Tunisia with subsequent thrombosis in one, and 1 in Algeria. In Morocco, 1 patient died acutely following discontinuation of antithrombotic agents, and another required amputation of both legs due to posterior tibial artery thrombosis.
Discussion
KD has been reported in more than 60 countries 2 since its first description in 1967, predominantly in Japan, followed by Korea (113.1/SDenom) and China (39.0–55.1/SDenom). 2 In Japan, the incidence of KD continues to increase, reaching 243.1 and 264.8/SDenom in 2011 and 2012, respectively. 7 In the province of Quebec, 2200 cases were diagnosed between 1975 and 2008 according the Quebec Kawasaki Disease Registry 8 and a systemic review performed by our group, estimating an incidence of 17 to 18/SDenom, which is considered high compared to other Western countries (Ireland 15.2, Italy 14.7, France 9.0, England 8.4, Finland 7.2, Sweden 6.2, Denmark 4.9) and equivalent to the United States (19.0/SDenom). 2 Comparatively, in Toronto metropolitan area, Ontario, Canada, the incidence is 26.2/SDenom, 9 where unlike the metropolitan region of Montreal, the East Asian descent population is substantially elevated.
In the Arab countries, especially the Maghreb region, the real incidence of KD seems low. In Morocco, a study performed in Fez reported 23 patients in Hassen II Hospital, which handles all the Wilaya of Fez. 3 In Tunisia, a retrospective study covering 10 years in 5 university hospitals identified 28 patients. 4 In the current study, the incidence of KD among Maghrebi children in Quebec is 4 to 12 times higher compared to those estimates. This difference may be attributed to underdiagnosis in the countries of origin and to the significant diagnostic delay in these countries compared to Quebec. As reflected in the present results, underdiagnosis may well be due to underrecognition of KD in cases presenting with concurrent infectious disease as suggested by the earlier guidelines, prior to the 2004 recommendations. It may also be a reflection of limiting the diagnosis of KD to cases with complete criteria in Algeria, for instance, the largest reported series of the Maghreb countries, where improving this aspect of the diagnosis may well improve patient outcome.
Seasonal variation in the incidence of KD is well known, peaking in winter in Canada, Korea, Japan, 11 and China, 10 and in spring in Taiwan. 11 This was considered to be related to rainfall in Japan and Costa Rica, and to the driest months in India. 11 In our series the first peak was in spring with the secondary peak in winter in Algeria and summer in Tunisia, possibly related to allergy and viral seasons in general as a relationship between KD and immunological dysregulation is suggested. In a Western Australian study the hospitalization odds ratio for asthma and allergy was 2.6:1 among KD patients compared to the general pediatric population, 12 most of which occurring prior to KD diagnosis. Furthermore, KD is supposedly induced by a delayed-type hypersensitivity due to pollen exposure. 13 In our series, personal and family histories of asthma and allergy were, respectively, found in 43% and 71% of Maghrebi patients residing in Quebec, suggestive of an environmental factor related to the immigration of this ethnic group. Indeed, environmental modifications may play a relevant role in the onset and severity of allergies and asthma among immigrants in Italy, for example, despite lower prevalence of family history of atopy compared to native Italians (27% vs 46%, respectively) and comparable smoking habits. 14
An infectious etiology of KD has been repeatedly evoked in the literature, 15 such as the identification of bacteria and viruses in the biological analyses of KD patients.16-18 In our study, a series of viruses and bacteria were identified such as cytomegalovirus, influenza B and varicella; and Escherichia coli, Streptococcus pneumonae, and Pseudomonas. Despite these findings, a causal relationship remains uncertain. Nevertheless, as an infectious trigger of immune dysregulation has been suggested,19,20 such occurrences remain important to report. In addition to the hypothesis of infectious etiology, genetic predisposition is an accepted hypothesis. Familial cases of KD have been reported, with significantly higher probability of a history of KD in parents whose children suffered from the disease. 21 Likewise, the risk of occurrence among siblings with the disease was 2.1% 22 and 13.9% in twins. 23
Coronary artery lesions are an important complication of this disease and determine its prognosis. Cardiac involvement can extend beyond the coronary artery and can involve inflammation to the 3 cardiac layers including the atrioventricular conduction system. 24 Coronary artery dilations generally remain inconsequential, whereas aneurysms may lead to life-threatening events, 24 including rupture of the affected coronary artery and sudden death. 25 Aneurysmal coronary lesions may evolve to ischemic stenosis and myocardial infarction. 26 A prolonged duration of fever and a delayed therapy are known risk factors for the development of aneurysm. 27 Although our patients residing in Quebec were diagnosed and treated earlier, the proportion of coronary artery lesions was comparable to the other 3 groups in general. Nevertheless, there was an obvious delay in administering therapy in Algeria and Tunisia, with an associated higher frequency of aneurysms. Furthermore, the incomplete form of the disease contributes to a delayed diagnosis and treatment, and subsequently to a greater risk for coronary artery aneurysm. 27 Although it was less common in Algeria, the incomplete form was significantly associated to a delayed diagnosis in Algeria and Morocco. Almost all diagnosed cases in Algeria were with complete clinical criteria, which raises the need to improve the acknowledgment of the incomplete form of the disease. Rapid and early suppression of the inflammation is critical for therapeutic response. 28 In combination with aminosalicylic acid, 20 the first line of treatment is intravenous immunoglobulins within 10 days from onset of fever; otherwise, the odds ratio of coronary aneurysms increases to 3.25. 29
Conclusions
The incidence of KD in the Maghreb community in Quebec is higher than the countries of origin where underdiagnosis seems substantial. Whereas the incomplete form of the disease is often left undiagnosed in Algeria, for example, delayed diagnosis is a point where efforts should be implemented in the Maghreb countries in general. On the other hand, atopic diseases and other potential immunological and environment modulations secondary to migration is worth considering.
Footnotes
Appendix
Total Number of Children <5 Years Old in the Wilaya of Fez Compared to That of the Whole Country of Moroccoa.
| General Population | Children <5 Years Old | Children <5 Years Old | |
|---|---|---|---|
| Wilaya of Fez | 964 891 | 8.4% | 81 051 |
| Morocco (country) | 31 543 000 | 9.2% | 2 899 000 |
Author Contributions
AAG: Contributed to conception and design; contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AF: Contributed to design; contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AAB: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LS: Contributed to acquisition and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RS: Contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AM: Contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ND: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Authors’ Note
This work originated from the Division of Pediatric Cardiology, CHU Ste-Justine, University of Montreal. The study was approved by CHU Ste-Justine Research Review Board as a central committee for the collaborating centers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.