
Abstract
China is a large country where rapid development is accompanied by growing inequalities. How economic inequalities translate to health inequalities is unknown. Baseline health assessment is lacking among rural Chinese children. We aimed at assessing baseline student health of rural Chinese children and comparing them with those of urban children of similar ages. A cross-sectional study was conducted using the 2003 Global School-Based Student Health Survey among 100 students Grade 4 to 6 from rural Guizhou, China. Results were summarized and compared with public data from urban Beijing using multivariate logistic regression models. Rural children are more likely to not wash their hands before a meal (odds ratio [OR] = 5.71, P < .01) and after using the toilet (OR = 5.41, P < .01). They are more likely to feel sick or to get into trouble after drinking (OR = 7.28, P < .01). They are more likely to have used drugs (OR = 8.54, P < .01) and to have no close friends (OR = 8.23, P < .01). An alarming percentage of rural (8.22%) and urban (14.22%) children have had suicidal ideation in the past year (OR = 0.68, P > .05). Rural parents are more likely to not know their children’s whereabouts (OR = 1.81, P < .05). Rural children are more than 4 times likely to have serious injuries (OR = 4.64, P < .01) and to be bullied (OR = 4.01, P < .01). In conclusion, school-age rural Chinese children exhibit more health risk behaviors and fewer protective factors at baseline compared to their urban counterparts. Any intervention aimed at improving child health should take this distributive gap into consideration.
Background
Health behaviors are well known to be hard to change. In 2007, the World Health Organization (WHO) reviewed worldwide evidence on the effectiveness of school-based health programs in changing health behaviors from an early age.1-3 It called for more efforts in building evidence based on practical experience. It recognized the need for improving implementation processes to ensure optimal transfer of evidence into practice and to pay attention to socioeconomically disadvantaged populations. Health Promoting Schools (HPS) are a multicomponent intervention model recommended to improve children’s health by changing health skills, intention, and environmental constraints that lead to healthier behaviors (Figure1). International scholars today agree that evidence on the feasibility, effectiveness, and scaling-up of HPS is especially needed in developing countries where these interventions can potentially have the most impact. 4

An adapted integrative conceptual map of key factors influencing health behaviors. 5
In China, pilot projects of HPS successfully reduced helminth infections and improved student knowledge, attitudes, and self-efficacy regarding HIV prevention in rural areas.6,7 Later in 2008, implementation of comprehensive HPS in Zhejing Province was shown to be efficacious in changing health attitude, knowledge, and behaviors. 8 However, these programs were implemented in a socioeconomically advantaged province. The results also did not reflect a sustainable impact due to a lack of long-term follow-up. Social desirability bias was also a concern because many outcomes were measured by self-report from the participants.
Guizhou province, located in Southwest China, is the poorest and one of the most underserved provinces in the country (see Figure 2). 9 Zhijin county is a typical minority-populated district with 23 ethnic minorities forming 48% of its population. Historically, minorities have been the most socioeconomically disadvantaged groups in the country. 10 The average annual farmer’s income is 3167RMB, or US$483. 11 According to the government census, 99.38% of the school-age children are receiving some form of governmental education. Health education in the villages, however, is practically nonexistent. Specifically, children and adolescents, as well as woman’s health, are often neglected.

Map of China showing the location of Guizhou province.
Objectives
This study aims to (a) study baseline health behaviors of rural Chinese children in an underserved community (b) compare them to those of urban Chinese children to assess needs for HPS.
Methods
The study used a cross-sectional survey method in 2 rural community schools in Zhijin county (Guizhou province, China). The 2003 Global School-Based Student Health Survey (GSHS) 12 was completed by 100 students. This number was based on the power calculation using an α of .05 to detect a hypothesized proportion difference of 10%. The students were randomly selected from Grades 4 to 6 by using a preexisting student number system that has no association to their names, age, or gender. All the 100 guardians of students surveyed gave verbal assent beforehand to the study via the school teachers due to the high illiteracy level. The widely tested GSHS included 68 core questions in 8 categories: “Hygiene,” “Drug Use,” “Mental Health,” “Nutrition,” “Activity,” “Protective Factors,” “Tobacco,” and “Safety.” Verbal assent was obtained from guardians of all children prior to survey administration because the majority of them were illiterate. We limited analysis to children ages 12 to 14 to make our sample more comparable to the publically available urban data. We calculated the prevalence of health behaviors and protective factors among Guizhou students (our data, n = 76) and compared the results with those from urban Beijing, using a publically available data set 13 and limiting the analysis again to ages 12 to 14 (n = 1629). Missing data under each question were treated by creating a separate “missing” category. Selected questions from each behavior categories are included in this article to keep results comparable to previously published WHO country-specific fact sheets. 13 Odds ratios (ORs) of the health behaviors and risk factors were obtained from logistic regression models adjusting for age and gender. A P value of <.05 was used to define statistically significant difference between the rural and urban children. Data analysis was completed using STATA version 11 (StataCorp, College Station, TX).
Results
Table 1 shows the basic characteristics of rural children from our sample (n = 76) and those of urban Beijing children (n = 1629). The mean age of the rural children is slightly lower (12.61 vs 13.33 years, P < .01) than the mean age of the urban children. Gender distribution is slightly more toward females (44.2% vs 44.4%) in both groups (P = .97). Rural children have a much lower mean weight compared with urban children (32.3 vs 50.63 kg, P < .01), and a much lower mean height as well (1.35 vs 1.60 m, P < .01). These differences are significant partly due to the disparity between our rural sample and the large urban sample. It is also due to our data collection in a remote rural area, where only elementary schools exist. Secondary education would require students to move to a more urban area. We tried to minimize the age difference by limiting the analysis to children aged 12 to 14 years in both groups.
Basic Characteristics of the Rural and Urban Students.
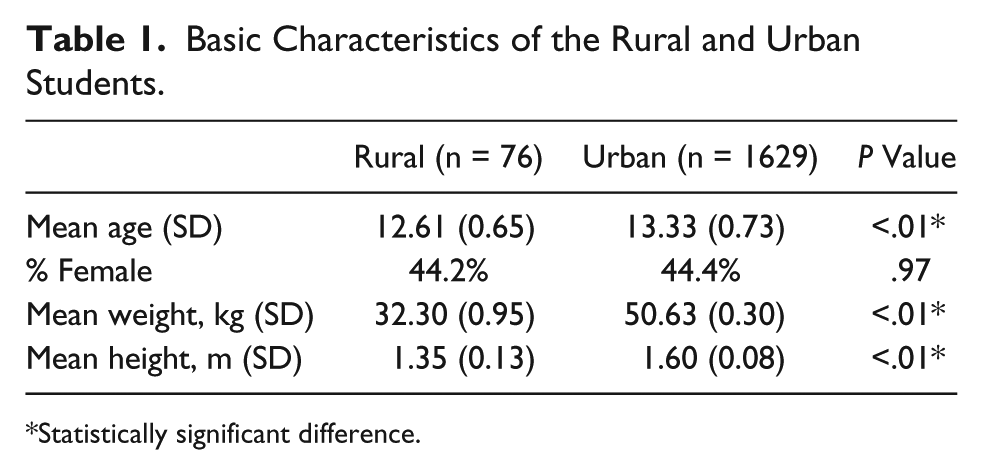
Statistically significant difference.
Table 2 summarizes the main findings in health behaviors. Rural children are more likely to not wash their hands before a meal (OR = 5.71, P < .01) and after using the toilet (OR = 5.41, P < .01). They are no more likely to drink by frequency (OR = 1.06, P < .05) but are significantly more likely to feel sick or to get into trouble after drinking (OR = 7.28, P < .01). Rural children are much more likely to have used drugs (OR = 8.54, P < .01). They are much more likely to have no close friends (OR = 8.23, P < .01). Though a higher percentage of them feel lonely most of the time, this difference compared with their urban counterparts was not statistically significant (OR = 2.10, P = .06). An alarming percentage of rural (8.22%) and urban (14.22%) children have had suicidal ideation in the past 12 months with no significant difference between the 2 groups (OR = 0.68, P > .05). In terms of nutrition, frequent sensation of hunger seems to be rare among rural (1.35%) and urban (2.40%) children (OR = 0.71, P > .05). Though obesity seems to be more prevalent among urban children (17.81%) than among rural children (11.54%), the difference was not statistically significant (OR = 0.52, P > .05). Rural parents are more likely to not know their children’s whereabouts (OR = 1.81, P < .05). Rural children are as likely to get into fights compared with urban children (OR = 1.58, P > .05), but they are more than 4 times likely to have serious injuries (OR = 4.64, P < .01) and to be bullied (OR = 4.01, P < .01).
Prevalence of Major Risk Behaviors and Protective Factors and Odds Ratios Comparing Guizhou Versus Beijing Students Who Are 12 to 14 Years Old.

P < .05. **P < .01.
Discussion
This is the first publicly available study on a broad range of baseline health behaviors and risk factors among underserved rural Chinese children. We chose ages 12 to 14 partly because they are the beginning years of adolescence, when children start to make more personal choices in their own behaviors. Baseline data are crucial for designing appropriate interventions to promote healthy behaviors in any community. They will also help objectively evaluate the impact of any interventions. Ultimately, evidence can be used for advocacy at the local health and global levels to implement effective interventions. 4
Our results show that underserved rural children exhibit more health risk behaviors in almost all major categories, including poor hand hygiene, more alcohol-related accidents and drug use, feeling lonely, lack of monitoring from parents, and increased incidents of injuries and bullying. Only when it comes to nutrition and suicidal ideation do they fare similarly, but no better, compared with their urban counterparts. This raises concerns over that urban-rural disparities do not just exist in socioeconomic conditions, they impact the health of children directly. These findings call for urgent action in piloting effective interventions in these underserved rural communities to build healthy behaviors in children before they form unhealthy behaviors for the rest of their adulthood. It is well known that injuries, drug and alcohol use, as well as neuropsychiatric disorders are major causes of morbidity and mortality in young adults.14,15
Literature has shown that, not only can HPS change behaviors of the participants but they can empower the children to teach their parents, who may have a lower level of education. This may initiate attitude and behavior changes in the entire community. Social impact may go beyond the students themselves. 8 To implement successful HPS programs, however, resources need to be dedicated to training teachers. When a project gained in intensity, teachers needed continuing training and periodic supervision to teach with more confidence and achieve more effects. 3 Our research serves as evidence that this investment is very much needed. It is an investment for the future of these underserved communities, as well as for the long-term health care savings and quality-adjusted life-years.
Our study has the strength of being the first of its kind in a truly underserved rural community in China. The sample was selected randomly among students of a comparable age group to that of the urban sample used as reference. The sample had a similar distribution in gender. The survey used has been well tested around the world through WHO-initiated implementation studies. Our results contribute to the public data available for pediatric health behaviors in China. They can also contribute to building evidence around the world regarding the implementation of child health interventions such as HPS. Our study also has several weaknesses. First, the generalizability of such results is debatable to other underserved communities outside of China, though the authors suspect that urban-rural disparities exist analogously in many other countries and interventions are similarly needed. Second, the study is cross-sectional and was done 8 years after the urban sample was obtained. There could have been some temporal shifts in the health behaviors, though they should actually accentuate the need for intervention in our sampled rural communities because further improvement would have been expected in the urban areas between 2003 and 2011. We may be underestimating the actual urban-rural health disparities as of 2011. Third, our sample size is small compared with the urban sample. This creates some imbalance in the combined data analysis and a tendency to overestimate differences. However, the prevalence estimates of health behaviors themselves are illustrative of the urban-rural differences even without logistic regression analysis. There is reason to suspect that the differences are rather substantial. Bigger rural sample sizes would be helpful for future studies, especially to illustrate the impact of pilot interventions. Finally, social desirability bias may be leading to underestimation of risk factors and behaviors, though it would affect both urban and rural students and enhance our conclusion that interventions are urgently needed to improve student healthy.
Conclusion
This is the first publicly available study on health behaviors among Chinese children in underserved rural communities. At baseline, these children exhibited significantly more health risk behaviors and fewer protective factors compared with their urban counterparts. HPS has high potential to fill this gap.
Footnotes
Author Contributions
XS substantially contributed to the conception and design of the study, contributed to acquisition, analysis, and interpretation of data, drafted the manuscript, critically revised the manuscript for important intellectual content and gave final approval for publication. DZ substantially contributed to acquisition, analysis, and interpretation of data, critically revised the manuscript for important intellectual content and gave final approval for publication. JS substantially contributed to the conception and design of the study, critically revised the manuscript for important intellectual content and gave final approval for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.