
Abstract

Introduction
The current gold standard of pediatric obesity treatment involves a family-based approach and behavioral modification, as posited by the 2007 American Academy of Pediatrics Expert Committee 1 and others.2-4 However, pediatricians implementing family-based approaches typically have experience in dyadic interactions, with a child and a parent, and not entire families. Effective therapies, such as Motivational Interviewing, 5 were initially utilized in areas outside of obesity, and adapted for use in weight management settings with families. 6 Similarly, weight management clinicians could gain valuable insight from those experienced in family therapy, but not necessarily weight management.
The goal of this study was to gain a deeper understanding of perceptions and methods of family therapists outside the field of weight management. We sought to determine which theoretical models guide their treatment and explore successful approaches to engage and retain patients to inform future interventions for pediatric obesity treatment.
Methods
Interview Guides
Interviews were developed to probe family therapy practice and approaches, engage families in treatment, and identify barriers to family-based treatment. Interviews were semistructured to allow new areas of interest to emerge (Table 1). 7 Interview guides were developed and tested via cognitive interviews. 8 These were mock interviews with treatment providers (counselors, psychologists) who then provided feedback on how questions were asked. Guides were then modified to ensure clarity and ease of understanding. The average length of interviews was 30 minutes. All protocols, interview questions, and consent processes were approved by the Wake Forest University Health Sciences Institutional Review Board.
Family Therapist Interview Guide.

Participants and Study Sites
Family-based mental health care providers were recruited through public contact listings (mostly email listserves) of professional mental health associations (Association of Marriage and Family Therapists, etc). An email describing the study was sent to members of these organizations; interested individuals were given enrollment instructions. Respondents who met eligibility criteria then were scheduled for a phone interview.
Subject Selection Criteria
Inclusion criteria were the following: licensure as a mental health professional, self-identification as a professional who routinely provides family therapy, English-speaking, and able to provide informed consent. We limited participation to therapists who are not primarily involved in weight management treatment, so we could gain unique and original perspectives from outside that specialty.
Data Collection
After completion of the consent process and demographic questionnaire, telephone interviews were digitally recorded using USB Blast (Goleta, CA) audio-recording technology. Interviews were transcribed verbatim.
Data Analysis
A content analysis approach was used to systematically code and aggregate responses, and then thematically analyze data. 9 This iterative process allowed ideas to emerge from the transcripts, and incorporated various individuals’ experiences to build understanding of the data. Interview transcripts were initially reviewed to identify potential codes by 2 investigators (JAB, JAS). The study team created a common coding system, along with a data dictionary for each code to separately assign agreed-upon codes to relevant text. Initially developed codes were then modified as needed. The codes were compiled to compare broad categories and for ongoing comparisons and revisions.
Results
Fourteen therapists responded and were interviewed (Table 2). Most reported that they practiced family, individual, and couples therapy. Participants’ clinical practices included work with blended families, secondary trauma, and foster care system issues. Most reported working in private practice settings, but also nonprofit clinics, inpatient facilities, and in-home services. Referrals to their practices most often came through colleagues, schools, physicians, insurance panels, hospitals, former clients, and word-of-mouth. See Table 3 for notable quotes from interviews.
Family Therapist Information.
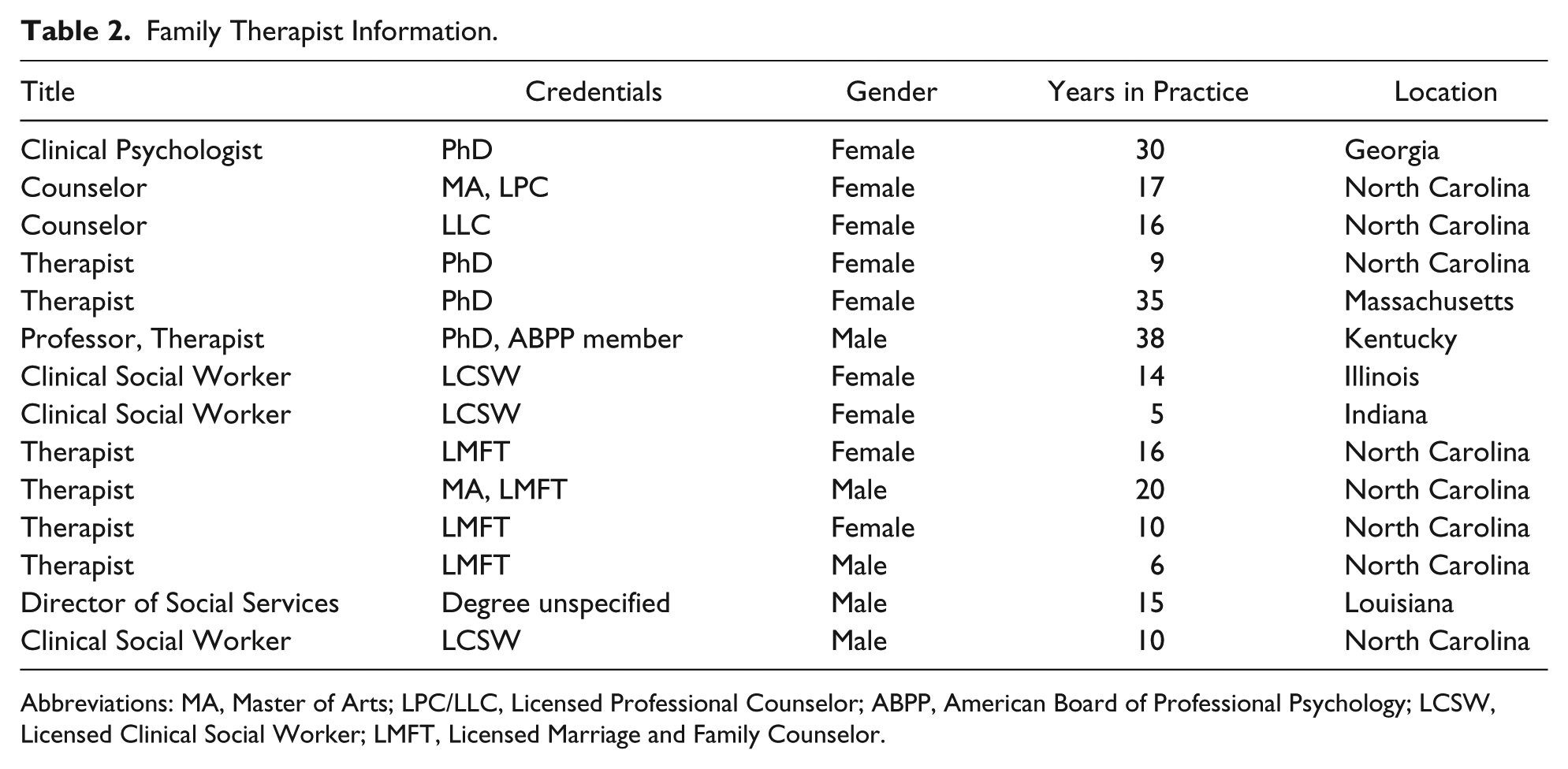
Abbreviations: MA, Master of Arts; LPC/LLC, Licensed Professional Counselor; ABPP, American Board of Professional Psychology; LCSW, Licensed Clinical Social Worker; LMFT, Licensed Marriage and Family Counselor.
Notable Quotations.
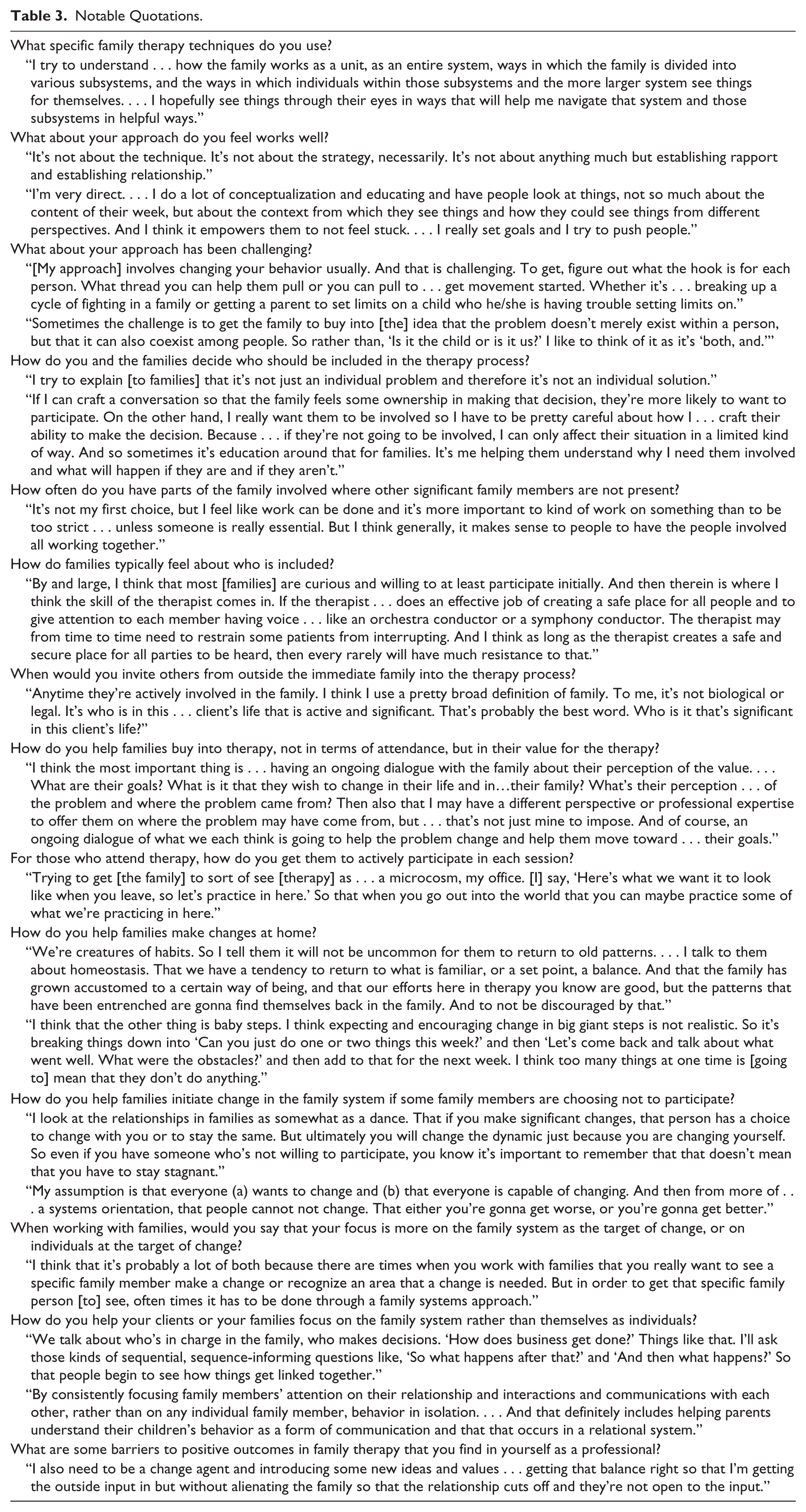
All participating therapists interviewed reported integrating theoretical models and specific approaches into their work. The most commonly reported theories included cognitive behavioral therapy, 10 structural family therapy, 11 and family systems therapy. 12 Others used brief solution-focused therapy, 13 ecological systems theory, 14 and attachment theory. 15 Specific family therapy techniques implemented with structural techniques including enactment (family members acting out transactional patterns within a session so that the therapist can intervene), constructing genograms, role-playing, communication techniques, strategic techniques, solutions-focused techniques, play-based activities, education, and family sculpting.
Approach
Therapists discussed which aspects of their approach they felt either were successful or challenging (see Table 4 for a summary).
Successful and Challenging Aspects of Therapists’ Approaches.

Family Participants
Therapists most often described a collaborative approach in deciding who should be included in the therapy. Often families led this conversation, with the therapist making suggestions; rarely was the family or therapist alone the sole determinant of who was involved in the treatment. A subset of therapists felt it imperative to meet with separate groups, or “subsystems,” rather than meeting with all family members each session. Conversely, therapists were fairly consistent on when it might be inappropriate to include certain significant family members, including when a patient might feel unsafe, if abuse was occurring in the home, or if certain topics of discussion would be inappropriate for younger children. They noted that some parents participating in family therapy with their children lack an understanding of how other family members might be related to a problem. Furthermore, most therapists acknowledged that when someone from outside the immediate family was related to an issue, that person should be invited into the therapy process. These persons were most often reported to be primary care providers, school counselors, teachers, extended family, pastors/priests, and friends. If necessary, therapists reported sometimes contacting these individuals directly and explaining the importance of their involvement, encouraging their clients to do the same, and allowing flexibility in their schedule to accommodate these additional participants.
Engagement
To help families find value in family therapy, therapists advocated being direct and honest with families (explaining their approach/plan to families, educating families on their methods, and recognizing themselves as outside perspectives to issues) and building a strong therapist–family relationship (gaining the family’s trust and building rapport). Therapists also recognized the importance of initially inviting everyone in a family to participate in therapy, and maintaining ongoing feedback regarding the efficacy of sessions.
For those who did attend therapy, therapists reported facilitating their active participation via flexibility in who participated, asking for regular feedback about how therapy was progressing, and highlighting the importance of families generating change for themselves. To assist families making changes at home, therapists most often cited creating homework assignments, formulating manageable goals between sessions, fostering accountability in patients, offering encouragement when changes were made, and practicing during a session. If some family members chose not to participate in therapy, therapists maintained that families could still initiate change in the family system. Therapists recognized that if they were successful in explaining to families the “ripple effect,” or the concept that if one person in a family system changes everyone will be affected, in addition to keeping uninvolved family members abreast of plans, changes in the system could still occur.
Most therapists reported focusing on either the family system or both the family system and individual. They found it helpful to show families how their interactions and relationships were linked via explanations of Family Systems Theory, 16 and providing examples of real-life scenarios. Therapists reported that a family’s reactions to this concept varied; some acknowledging the value of viewing a family as interconnected, while some did not find it helpful or did not understand the interplay.
Treatment Barriers
The most commonly reported treatment barriers included lack of acceptance from significant members of a family, inadequate resources (psychosocially and financially), scheduling issues, and external issues (ongoing substance abuse in the household, financial constraints, etc). Therapists reported their own barriers to positive outcomes as not being the best “fit” for a particular family secondary to personality differences, pressures on their productivity that force them to limit caseloads, lack of financial support for continued education/training, and insurance plans that did not consistently cover family therapy.
Referrals
Every therapist reported frequently referring clients to other health care providers. The most common reasons for referrals included when issues were deemed outside the realm of the therapist’s professional expertise (eg, patients had medical or substance abuse problems), if clients required additional forms of therapy, or if a therapist and family were not making progress. All therapists reported recommending community resources for their families. Commonly mentioned support groups were church/faith-based services, sports teams, social services for children, and more specific services based on the presenting issue (financial support, mediation in divorced couples, career counseling, etc).
Conclusion
The therapists interviewed stressed the importance of obtaining family acceptance and understanding of family therapy, encouraging other members to participate, and appreciate its potential value. This was successful when therapists assumed a direct and honest approach with families and explained the “ripple effect.” Therapists also recommended engaging families collaboratively to determine who should be included in treatment, maintaining flexibility in scheduling appointments, allowing families to “practice” in clinic, and recognizing families’ complexity. Although not specific to pediatric obesity, key ideas reported here may be translated into this field.
The main limitation of the study was its small size (n = 14) and the self-reported nature of the information from therapists. Nevertheless, their insights may assist family-based pediatric obesity treatment providers. While more research is needed to understand dynamics of obesity and families, this study will provide additional tools and approaches for family-based obesity treatment.
Footnotes
Acknowledgements
The authors would like to thank Karen Klein, MA, ELS (Biomedical Research Services and Administration, Wake Forest University Health Sciences), for editing this article.
Author Contributions
JAB contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
MBI contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
SGK contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
EMA contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
JAS contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Skelton has been a consultant for Nestlé Corporation, which was not involved in any part of this research and did not fund any aspects of the research. The other authors have no conflict of interests to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Skelton was supported in part through an NIH Mentored Patient-Oriented Research Career Development Award (K23 HD061597). Dr Bishop was supported by an NIH Short-Term Training for Medical Students Award (T35 DK007400; PI: Reid).