
Abstract
The impact of chronic pain on neuropsychological functioning of older adults is under-studied. The present study examined the relationship between chronic pain, depression, anxiety, cognition, and functional capacity in community-dwelling older adults (ages 60–89) who completed an outpatient neuropsychological evaluation (N = 452). Psychometrically sound and validated measures were used to assess depression (Geriatric Depression Scale [GDS]), anxiety (Beck Anxiety Inventory [BAI]), cognitive functioning (the Mini Mental Status Exam [MMSE] and the Repeatable Battery for the Assessment of Neuropsychological Status [RBANS]), and functional capacity (Texas Functional Living Scale [TFLS] and Instrumental Activities of Daily Living Questionnaire [IADL]). Multivariate analyses of covariance (MANCOVA) were conducted to examine differences between individuals with and without chronic pain, adjusting for age, education, gender, marital status, and other medical conditions. Results indicated that participants endorsing chronic pain displayed significantly higher levels of depression and anxiety, as well as lower levels of cognitive functioning and functional capacity, than those without chronic pain. Additionally, results of hierarchical multiple regressions indicated that chronic pain explained unique variance in all outcome variables, beyond demographic characteristics and health status. Chronic pain management may be an important intervention target for clinicians to help address cognitive and psychological functioning in older adults.
Introduction
Chronic pain is a complex medical condition that affects an estimated 30% to 38.5% of adults over the age of 65 (Larsson et al., 2017; Rikard et al., 2023). Chronic pain is distinct from acute pain as it persists, generally for at least 3 months, and can significantly impact the quality of life and functional abilities of older adults (Domenichiello & Ramsden, 2019; National Institute of Health, 2023). Research indicates that chronic pain has been associated with a number of adverse mental health outcomes, as well as cognitive concerns and limitations in functional capacity (e.g., Bunk et al., 2019; Higgins et al., 2018; Mazza et al., 2018). These findings highlight the necessity of routinely addressing pain as part of geriatric care.
Chronic Pain and Psychiatric Symptoms
Chronic pain has been associated with increased symptoms of mental health disorders (Zis et al., 2017), with multiple studies indicating that patients with chronic pain report higher levels of depression and anxiety symptoms and decreased feelings of well-being (e.g., Mullins et al., 2023; Puto et al., 2023; C. S. Ritchie et al., 2023; Tse et al., 2013). The literature suggests that chronic pain can serve as both a psychological stressor and a physical ailment that contributes to the onset and exacerbation of mood disorders. A number of biological mechanisms (monoamine neurotransmitters, brain-derived neurotrophic factor, inflammatory factors, and glutamate) have been implicated in both chronic pain and depression (Meda et al., 2022; Zis et al., 2017). Additionally, studies indicate that the enduring nature of pain may lead to alterations in brain chemistry and neural circuitry associated with mood regulation, thereby increasing the vulnerability to depressive states (Han & Pae, 2015).
The experience of continuous pain can lead to a state of heightened physiological arousal akin to anxiety, as individuals may anticipate future pain episodes or experience a persistent, negative, cognitive affective style characterized by helplessness, magnification, and ruminative thoughts regarding one’s pain (e.g., pain catastrophizing; Dong et al., 2020). In fact, significant positive associations have been found between fear of pain, pain catastrophizing, pain-related negative affect, anxiety, depression, and pain-related disability (Rogers & Farris, 2022). Some studies have attempted to clarify the directionality of the relationship between chronic pain and psychiatric symptoms with indications that negative emotions may predict pain, disability, and duration of symptoms (e.g., Bonilla-Jaime et al., 2022; Lerman et al., 2015). Puto et al. (2023) added that additional predictors of depression around pain may include social isolation, sole completion of primary education, and disability related to activities of daily living. Although some studies (e.g., Smith & Ayres, 2014) have not found a relationship between psychological symptoms and pain, the vast majority of literature reveals a complex and multifaceted relationship between chronic pain experiences and psychiatric symptoms, warranting further examination.
Chronic Pain and Functional Capacity
The impacts of chronic pain on functional capacity have also been researched and documented in the adult and older adult populations. A majority of study findings indicated individuals with chronic pain were more likely to report difficulty with activities of daily living (ADLs) or physical function when compared to individuals without chronic pain (Dueñas et al., 2020; Puto et al., 2023; C. S. Ritchie et al., 2023). Some studies also report difficulties with instrumental activities of daily living (IADLs; Connolly et al., 2017; Prefontaine & Rochette, 2013; Puto et al., 2023). Published research has also noted the distribution, severity, and interference of pain as some of the best predictors for difficulties with ADLs/IADLs (Dueñas et al., 2020; Eggermont et al., 2014). Furthermore, Stamm et al. (2016) noted that the presence of pain in older adults can increase work impairment and lead to the increased use of healthcare services. However, research findings remain somewhat inconsistent, as some studies have found no relationship between functional capacity and chronic pain (e.g., Tse et al., 2013). Thus, evaluation of functional capacity and additional attenuating factors is another area for ongoing research in older adults with chronic pain.
Chronic Pain and Cognitive Functioning
Research has consistently documented a correlation between chronic pain and cognitive impairment in older adults. Older adults may have a 21% increased chance of cognitive impairment for every 2 years of persistent pain interference (Bell et al., 2022). Decreased efficiency across all domains of neurocognition has been noted in chronic pain literature studying older adult populations (e.g., Bunk et al., 2019; Corti et al., 2021; Higgins et al., 2018; Mazza et al., 2018). One possible explanation for the impact of chronic pain on cognitive functioning is that chronic pain may compete for cognitive resources—particularly in domains such as attention and working memory—which are essential for daily cognitive functioning (Baker et al., 2016; Higgins et al., 2018; Murata et al., 2017). This competition can result in cognitive overload, reducing the capacity of these individuals to process information efficiently and make decisions effectively.
It is important to note that research has identified mixed findings related to the relationship between chronic pain and cognitive functioning. Two systematic reviews and meta-analyses and one study using longitudinal data seemed to counter prior positive findings by retrieving small to moderate magnitudes, low-quality evidence, or no evidence that adults or older adults with pain have worse cognitive functioning than individuals without pain (Nery et al., 2023; Rathbone et al., 2016; C. S. Ritchie et al., 2023). Another recent systematic review also found mixed evidence by concluding that sixteen studies showed that patients with chronic pain had impaired cognitive functioning; six studies found chronic pain did not worsen cognitive function, and one study concluded the impact of pain on cognitive function depended on the underlying cognitive status (Jang et al., 2022). These cognitive deficits may be due to the pain itself or to the psychological stress and negative affective states (i.e., depression, anxiety) associated with chronic pain, which can lead to changes in brain regions involved in cognitive processes (e.g., Ojeda et al., 2018; Yang & Chang, 2019). This may also be due to the existence of mediating and moderating factors in the relationship between chronic pain and cognitive functioning, including the effects of medication, mood symptoms, and chronicity or intensity level of pain (Higgins et al., 2018). These findings underscore the importance of further examination of the cognitive profile of chronic pain in older adults, as well as consideration of the importance of addressing chronic pain management and additional attenuating factors to address cognitive health in older adults.
Rationale for the Present Study
Understanding the presentation of chronic pain in older adults and its relationship to mental health, cognitive functioning, and functional capacity is crucial for developing effective pain management strategies, improving the quality of life, and reducing the overall burden on healthcare systems. Although a number of published studies have focused on chronic pain and its impact on individual domains (such as mental health or cognition), few have examined its effects comprehensively across multiple domains, such as psychiatric symptoms, functional capacity, and cognitive function within a single study. The present study is one of the few to adopt a holistic approach by assessing chronic pain across all three domains in a single sample. Furthermore, this study is unique in evaluating the specific contributions of chronic pain beyond demographic factors and other medical conditions, quantifying its impact with effect sizes to better capture the extent and magnitude of these associations. This comprehensive examination is critical for understanding the complex impacts of chronic pain in older adults. Further studies in this area are essential, as they can inform caregivers and policymakers about the specific needs of older adults with chronic pain so that effective targeted interventions and support systems can be developed.
The aim of the present study was to address these gaps in the literature and contribute to the field by investigating multifaceted associations between chronic pain and a number of behavioral health outcomes (anxiety, depression, cognition, and functional capacity) in a sample of community-dwelling older adults. The researchers hypothesized that individuals who endorsed chronic pain complaints would display higher levels of mental health concerns, lower scores on tests of cognitive functioning, and higher impairments in functional capacity, after adjusting for demographic characteristics and the number of medical conditions. Additionally, it was hypothesized that chronic pain would explain unique variance in outcome variables, beyond demographics and health status.
Methods
Participants
This study involved a sample of 452 community-dwelling adults aged 60 to 89 who presented for a neuropsychological evaluation at an outpatient neuropsychological clinic in Virginia (see Table 1 for participants’ demographic characteristics). After checking in for their appointment, patients completed a history and demographics form in the waiting room. This form had several demographic questions as well as a number of dichotomous questions regarding the patient’s health; one of the items on the form asked whether they experienced chronic pain. Patients circled “yes” or “no” in response to the question, “Do you have chronic pain complaints?” Responses were later reviewed and discussed in clinical interviews (completed by doctoral-level psychologists or a board-certified neuropsychologist) to obtain further information regarding pain complaints. For the purposes of this study, the participants were split into two groups (chronic pain group and control group); individuals were classified into the chronic pain group if they endorsed chronic pain complaints on the history form and these concerns were later discussed and verified in the clinical interview. Of 452 patients, 224 were classified into the chronic pain group based on their responses on the history form and clinical interview.
Participant Demographics and Characteristics (N = 452).

Note. M = mean; SD = standard deviation.
Two performance validity tests (PVTs) were utilized in this study: the Word Choice Test (WCT; Pearson, 2009) and the Effort Index (EI) embedded within the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS; Silverberg et al., 2007). Participants were included in the current study only if they passed both the WCT (<43; Bernstein et al., 2021) and the EI (>3; Silverberg et al., 2007) in order to ensure the validity of the neuropsychological data and to reduce the risk of confounding results due to inadequate effort or response bias.
Most commonly reported medical diagnoses included hypertension (n = 201; 44.5%), diabetes (n = 99; 21.9%), hyperlipidemia (n = 84; 18.6%), arthritis (n = 67; 14.8%), heart disease (n = 41; 9.1%), non-CNS cancer (n = 21; 4.6%; most common: breast, prostate, and skin cancer); GERD (n = 49; 10.8%), and kidney disease (n = 81, 17.9%). Approximately one-third of participants had a history of a neurological disorder (n = 134, 29.6%).
Measures
Psychiatric Symptoms
Depression was assessed using the Geriatric Depression Scale-Short Form (GDS-SF; Yesavage & Sheikh, 1986), which is a condensed version of the original GDS, containing 15 dichotomized items selected to screen for depression in older adults. The short form retains the psychometric robustness of the full version and is well-suited for both clinical and research settings (Almeida & Almeida, 1999; Yesavage & Sheikh, 1986). Total GDS-SF score was used in the present study, with higher scores indicating greater symptoms of depression.
The Beck Anxiety Inventory (BAI; Beck et al., 1988), a 21-item self-report inventory, was used to measure the severity of anxiety. It assesses the severity of both somatic and cognitive symptoms of anxiety, asking respondents to rate how much they have been bothered by each symptom during the past week on a scale from 0 (not at all) to 3 (severely). The BAI has strong psychometric properties. It has consistently demonstrated high internal consistency across various populations, with Cronbach’s alpha coefficients often cited as .89 or above, indicating a strong degree of reliability among the items of the scale (Beck et al., 1988; Morin et al., 1999). Total BAI score was used in the present study, with higher scores indicating greater symptoms of anxiety.
Cognitive Functioning
Cognitive functioning was assessed using the Mini-Mental State Examination (MMSE; Folstein et al., 1975) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS; Randolph et al., 1998).
The MMSE is a widely used and validated 30-point cognitive screening measure that includes a variety of cognitive tasks including orientation, attention, memory, language, visuospatial skills, and constructional praxis. The MMSE has demonstrated moderately high levels of reliability and internal consistency across diverse patient populations, including those with dementia syndromes and other psychiatric conditions, as well as cognitively intact individuals (Bernard & Goldman, 2010). The total MMSE score was used in the present study.
The RBANS is an individually administered test intended to evaluate the neuropsychological status of adults aged 20 to 89 years, particularly those with suspected neurological deficits. It is a brief battery—typically administered within 30 to 40 min—and is utilized in clinical settings to measure immediate and delayed memory, visuospatial/constructional skills, attention, language, and overall cognitive functioning. Research has supported the clinical value and psychometric properties of the RBANS across various medical populations (Loughan et al., 2019), and it has been shown to have adequate sensitivity in detecting cognitive impairments in various neuropsychiatric conditions (Duff et al., 2010). The RBANS Total Scale Scores were used in the present study, along with all subtest scores.
Functional Capacity
Functional capacity was evaluated using the Texas Functional Living Scale (TFLS; Cullum et al., 2009), which assesses an individual’s ability to perform simulated instrumental activities of daily living. The TFLS includes 24 performance-based items and yields a total score and four subscale scores: time, money and calculation, communication, and memory. In addition, the TFLS incorporates ecologically valid tasks (Drozdick & Cullum, 2011). The TFLS has demonstrated evidence of robust reliability, internal consistency, and validity (both convergent and discriminant) with several measures of adaptive functioning (Cullum et al., 2001). Total TFLS total and subscale scores were used in this study. In addition to the TFLS, all participants also completed a dichotomized Instrumental Activities of Daily Living (IADL) self-report questionnaire as part of the intake. The number of IADL subdomains in which the examinee indicated requiring assistance was summed up to create a continuous variable of functional capacity.
Procedures
The study utilized a retrospective analysis of archival clinical data. All participants completed the Geriatric Depression Scale-Short Form (GDS-SF), the Beck Anxiety Inventory (BAI), the Mini-Mental Status Exam (MMSE), the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), and the Texas Functional Living Scale (TFLS) as part of a comprehensive neuropsychological assessment battery. The study was approved by the Human Subjects Ethics Review Committee (HSRC) at a local university. To reduce type I error due to multiple analyses, false discovery rate (FDR; Benjamini & Hochberg, 1995) was utilized, correcting for multiple comparisons at p < .05.
Statistical Analyses
Multivariate Analysis of Covariance (MANCOVA)
First, a multivariate analysis of covariance (MANCOVA) was conducted to examine the association between chronic pain and a combination of outcome variables across three domains: (1) psychiatric symptoms, (2) cognitive functioning, and (3) functional capacity. This analysis included the following covariates: age, education, gender, marital status, and the presence of other medical conditions, to isolate the unique contribution of chronic pain. The combined dependent variable included two measures from each domain (a total of six outcome variables were combined into the composite DV within the MANCOVA: BAI, GDS-SF, MMSE, RBANS, TFLS, IADL), allowing for an assessment of the role of chronic pain in these interconnected areas of functioning.
Analyses of Covariance (ANCOVA)
Next, follow-up analyses of covariance (ANCOVA) were conducted to compare the two groups (“chronic pain group” and “no chronic pain group”) in terms of psychiatric symptoms, functional capacity, and cognitive functioning after adjusting for demographic variables (age, education, gender, marital status, and the number of medical conditions). ANCOVA results revealed significant differences between the two groups on all outcome variables. Table 2 presents the comprehensive results of all ANCOVA analyses, as well as means and standard deviations for both groups on all outcome variables.
Comparing Means and Standard Deviations for Outcome Variables Between Individuals with Chronic Pain Diagnosis and Control Group (N = 452).

Note. M = mean; SD = standard deviation; d = Cohen’s d; BAI = Beck anxiety inventory (higher scores indicate higher levels of anxiety symptoms); GDS-SF = geriatric depression scale, short form (higher scores indicate higher levels of depression symptoms); TFLS = Texas functional living scale (higher score indicates better functional capacity); IADL = instrumental activities of daily living questionnaire (higher score indicates a higher number of problems with completing instrumental activities of daily living and therefore lower functional capacity); MMSE = mini mental status exam (higher scores indicate better cognitive functioning); RBANS = repeatable battery for the assessment of neuropsychological status (higher scores indicate better levels or cognitive functioning). All differences were statistically significant after false discovery rate (FDR) correction for multiple comparisons, with the exception of list recognition (p = .093).
Hierarchical Multiple Regressions
Finally, hierarchical regression analyses were conducted to evaluate the magnitude of the relationship between chronic and all outcome variables, after adjusting for demographic factors (age, education, gender, and marital status) and the number of medical conditions. The outcome variables were divided into three categories: psychiatric symptoms (anxiety and depression), functional capacity (TFLS and IADL total scores), and cognitive functioning (MMSE and RBANS total scores). Complete details of hierarchical regression analyses are presented in Table 3 (psychiatric symptoms), Table 4 (functional capacity), and Table 5 (cognitive functioning).
Hierarchical Regressions Evaluating Associations of Chronic Pain with Psychiatric Symptoms, After Adjusting for Demographic Characteristics and Medical Conditions (N = 452).

Note. R2 = coefficient of determination; ΔR2 = change in R2 when additional predictors are added; ΔR2 sig = p-value for change in R2; B = unstandardized beta; SEB = standard error of beta; β = standardized beta coefficient; LLCI = lower limit confidence interval; ULCI = upper limit confidence interval; BAI = Beck anxiety inventory (higher scores indicate higher levels of anxiety symptoms); GDS-SF = geriatric depression scale, short form (higher scores indicate higher levels of depression symptoms). Categorical variables of gender and marital status were dichotomized for these regression analyses (gender: male = 1; female = 0; marital status: married = 1; not married = 0 [“not married” category includes single, divorced, and widowed groups]). Number of medical conditions = number of other medical conditions, not including chronic pain (e.g., hypertension, diabetes, heart disease, kidney disease, cancer, etc.). Bold font indicates statistical significance after adjustment for familywise error using false discovery rate (FDR).
Hierarchical Regressions Evaluating Associations of Chronic Pain with Functional Capacity, After Adjusting for Demographic Characteristics and Medical Conditions (N = 452).

Note. R2 = coefficient of determination; ΔR2 = change in R2 when additional predictors are added; ΔR2 sig = p-value for change in R2; B = unstandardized beta; SEB = standard error of beta; β = standardized beta coefficient; LLCI = lower limit confidence interval; ULCI = upper limit confidence interval; TFLS = Texas functional living scale (higher score indicates better functional capacity); IADL = instrumental activities of daily living questionnaire (higher score indicates a higher number of problems in completing instrumental activities of daily living and therefore lower functional capacity). Categorical variables of gender and marital status were dichotomized for these regression analyses (gender: male = 1; female = 0; marital status: married = 1; not married = 0 [“not married” category includes single, divorced, and widowed groups]). Number of medical conditions = number of other medical conditions, not including chronic pain (e.g., hypertension, diabetes, heart disease, kidney disease, cancer, etc.). Bold font indicates statistical significance after adjustment for familywise error using false discovery rate (FDR).
Hierarchical Regressions Evaluating Associations of Chronic Pain with Cognitive Functioning, After Adjusting for Demographic Characteristics and Medical Conditions (N = 452).

Note. R2 = coefficient of determination; ΔR2 = change in R2 when additional predictors are added; ΔR2 sig = p-value for change in R2; B = unstandardized beta; SEB = standard error of beta; β = standardized beta coefficient; LLCI = lower limit confidence interval; ULCI = upper limit confidence interval; MMSE = mini mental status exam (higher scores indicate better cognitive functioning); RBANS = repeatable battery for the assessment of neuropsychological status (higher scores indicate better levels or cognitive functioning). Categorical variables of gender and marital status were dichotomized for these regression analyses (gender: male = 1; female = 0; marital status: married = 1; not married = 0 [“not married” category includes single, divorced, and widowed groups]). Number of medical conditions = number of other medical conditions, not including chronic pain (e.g., hypertension, diabetes, heart disease, kidney disease, cancer, etc.). Bold font indicates statistical significance after adjustment for familywise error using false discovery rate (FDR).
Results
The average age of participants was 73.50 (SD = 7.36), with an average education level of 14.11 years (SD = 2.78). Table 1 presents complete demographic data for the studied sample. In terms of psychiatric diagnoses, approximately one-fifth of participants had a diagnosable psychiatric disorder (n = 85; 18.8%), such as a depressive disorder (n = 67; 14.8%), an anxiety disorder (n = 36; 7.9%), or PTSD (n = 12; 2.7%).
Multivariate Analysis of Covariance (MANCOVA)
The multivariate analysis of covariance (MANCOVA) results indicated that chronic pain had a statistically significant multivariate effect on the combined outcome variables across the three domains of psychiatric symptoms, cognitive functioning, and functional capacity. After adjusting for covariates, including age, education, gender, marital status, and medical conditions, the Wilks’ λ value of 0.842 was significant (F = 7.89, p < .001), with chronic pain accounting for 15.8% of the variance in the combined dependent variable. This suggests that chronic pain significantly impacts the combined outcomes even when controlling for demographic and medical variables.
Analyses of Covariance (ANCOVA)
Psychiatric Symptoms
In terms of anxiety, the difference in BAI total scores between the two groups was statistically significant, F(1, 445) = 53.59, p < .001. Participants with chronic pain (BAI M = 12.15, SD = 12.64) reported significantly higher anxiety scores compared to those without chronic pain (BAI M = 4.05, SD = 6.47). Statistically significant difference was also found for the GDS scores, F(1, 445) = 40.73, p < .001; participants with chronic pain (GDS M = 5.89, SD = 4.68) had significantly higher depression scores compared to those without chronic pain (GDS M = 3.11, SD = 3.43). See Figure 1 for a graphic depiction of these results.

Differences in psychiatric symptoms between individuals with chronic pain and without chronic pain.
Functional Capacity
Chronic pain complaints were also significantly associated with functional capacity (TFLS F(1, 429) = 40.83, p < .001; IADL F(1, 429) = 9.59, p = .002). The chronic pain group demonstrated lower scores on a measure of functional capacity (TFLS M = 35.95; SD = 10.12) and endorsed more difficulties in completing instrumental activities of daily living (IADL M = 2.25; SD = 2.2) when compared to those who denied chronic pain complaints (TFLS M = 42.28; SD = 8.72; IADL M = 1.14; SD = 1.87; see Figure 2). All differences were statistically significant after FDR adjustment for multiple comparisons (p < .01), with the exception of List Recognition.
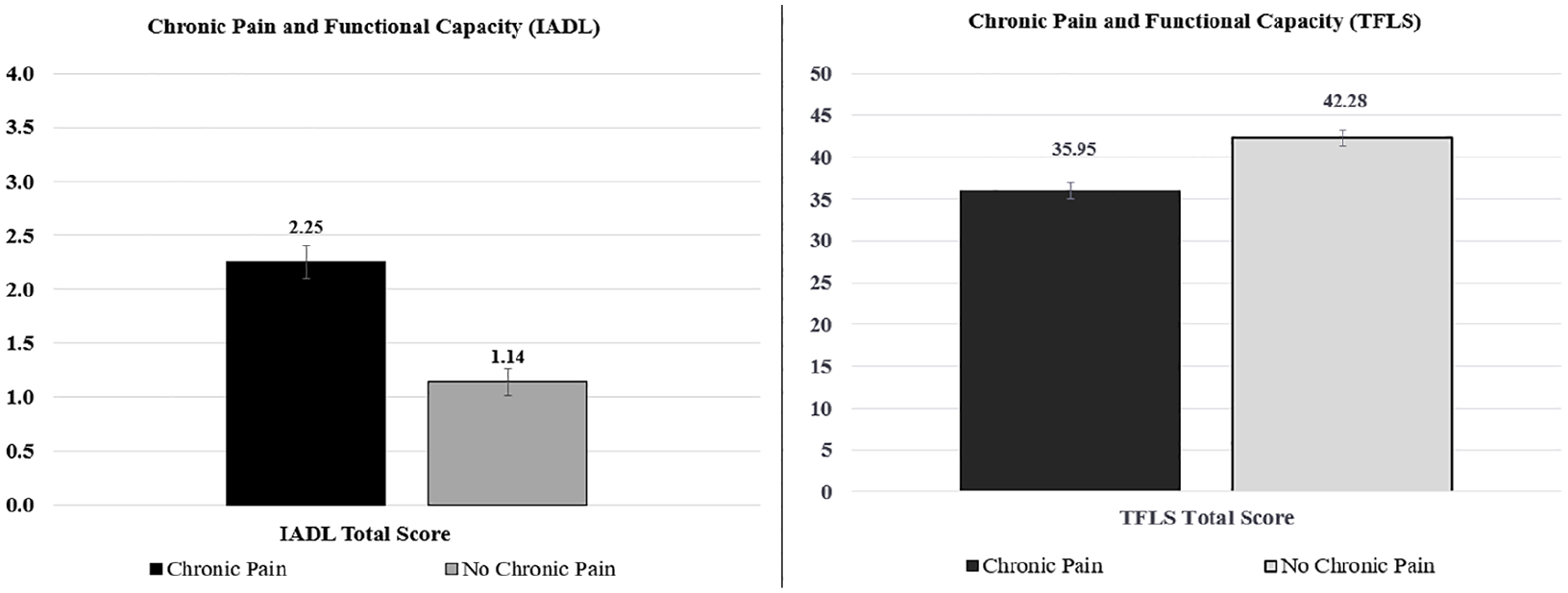
Differences in functional capacity between individuals with chronic pain and those without chronic pain.
Cognitive Functioning
Finally, chronic pain was also significantly associated with cognitive functioning scores (MMSE F(1, 445) = 10.34, p = .001; RBANS F(1, 445) = 36.65, p < .001). Specifically, individuals with chronic pain displayed lower scores on the MMSE (M = 24.36, SD = 4.69) and RBANS (M = 86.93, SD = 21.03) when compared to individuals without chronic pain (MMSE M = 26.20, SD = 3.98; RBANS M = 101.25, SD = 24.81). See Figure 3 and Figure 5 for a graphic depiction of these results.

Differences in cognitive functioning between individuals with chronic pain and those without chronic pain.

Unique variance (ΔR2) explained by chronic pain beyond demographic characteristics and number of medical conditions.

Differences in RBANS subtests scores between chronic pain group and control group.
Hierarchical Multiple Regressions
Psychiatric Symptoms
In the first set of analyses focusing on psychiatric symptoms, the initial model (Model 1) that included only demographic variables, accounted for a modest but significant portion of variance in both anxiety (R² = .089, F(5, 446) = 8.70, p < .001) and depression (R² = .054, F(5, 446) = 5.09, p < .001). Within the first model, the number of medical conditions was a significant predictor for both anxiety (β = .24, p < .001) and depression (β = .16, p < .001), while age, education, gender, and marital status were not significant predictors. Adding chronic pain at the next step (Model 2) as an additional predictor significantly increased the explained variance in both anxiety (ΔR² = .098, F(1, 445) = 53.59, p < .001) and depression (ΔR² = .079, F(1, 445) = 40.73, p < .001). Effect sizes were medium (BAI ΔR2 = .098; GDS ΔR2 = .079). This suggests that chronic pain contributes to psychiatric symptoms above and beyond the demographic factors, and that chronic pain is associated with higher levels of both anxiety and depression. Complete details of these analyses are presented in Table 3.
Functional Capacity
Complete details of hierarchical regressions evaluating associations of chronic pain with functional capacity are presented in Table 4. These analyses revealed that demographic variables alone (Model 1) explained a sizeable amount of variance in TFLS scores (R2 = .115, F(5, 430) = 11.15, p < .001) and in IADL scores (R2 = .091, F(5, 259) = 5.18, p < .001). In Model 1 for TFLS, age (β = −.21, p < .001) and education (β = .22, p < .001) were significant predictors of functional capacity, while gender, marital status, and the number of medical conditions were not. In Model 1 for IADL, only the number of medical conditions (β = .21, p < .001) significantly predicted the level of concerns related to completing instrumental activities of daily living. Introducing chronic pain as an additional predictor at the next step (Model 2) significantly increased the total amount of variance explained in both models, explaining additional 7.7% of variance in TFLS scores (ΔR2 = .077, F(1, 429) = 40.83, p < .001) and 3.3% of variance in IADL scores (ΔR2 = .033, F(1, 258) = 9.59, p = .002). On TFLS, chronic pain was associated with a lower level of functional capacity, and on the IADL, chronic pain was linked with a higher number of problems in completing instrumental activities of daily living. Effect sizes were medium (TFLS ΔR² = .077; IADL ΔR² = 0.033). These findings highlight the significant relationship between chronic pain and functional capacity beyond demographic factors.
Cognitive Functioning
Complete details of hierarchical regressions evaluating associations of chronic pain with cognitive functioning are presented in Table 5. These analyses revealed that demographic variables alone (Model 1) explained a considerable amount of variance in MMSE scores (R2 = .118, F(5, 446) = 11.89, p < .001) and in RBANS scores (R2 = .222, F(5, 446) = 25.47, p < .001). In Model 1 for MMSE, only the number of medical conditions (β = −.30, p < .001) was a significant predictor of the total MMSE score. In Model 1 for RBANS, age (β = −.34, p < .001), education (β = .23, p < .001), and the number of medical conditions (β = −.19, p < .001) were significantly associated with the RBANS total scale scores. Introducing chronic pain as an additional predictor at the next step (Model 2) significantly enhanced the models, explaining additional 2% of variance in MMSE scores (ΔR2 = .020, F(1, 445) = 10.34, p = .001) and 5.9% of variance in RBANS scores (ΔR2 = .059, F(1, 445) = 36.65, p < .001). On both cognitive measures, chronic pain was associated with lower levels of cognitive functioning. Effect sizes ranged from small (MMSE ΔR² = .020) to medium (RBANS ΔR² = .059). These findings underscore the significant inverse relationship between chronic pain and cognitive functioning beyond demographic factors.
Please see Figure 4 for a graphic representation of unique contributions of chronic pain (ΔR²) to all outcome variables beyond demographic characteristics and medical conditions.
Bivariate Correlations
Finally, bivariate correlations were conducted to examine the interrelations between the studied domains. The correlation analysis revealed significant relationships among the three domains: (1) psychiatric symptoms (BAI and GDS-SF), (2) cognitive functioning (MMSE and RBANS), and (3) functional capacity (TFLS and IADLS). Both anxiety and depressive symptoms were positively correlated with each other (r = .636, p < .001), suggesting a strong interrelation within the psychiatric symptoms domain. These symptoms also showed inverse relationships with cognitive functioning and functional capacity. Both measures had somewhat stronger associations with functional capacity (r range: .158-.287) than with cognitive measures (r range: .149-.246). All correlations were significant (p < .01). Correlations revealed that greater psychiatric symptoms corresponded with reduced cognitive and functional abilities. Cognitive functioning measures (MMSE and RBANS) were also strongly correlated (r = .514, p < .001), and both showed strong positive associations with functional capacity measures (TFLS and IADL), indicating that cognitive health is associated with higher functional ability. See Table 6 for complete details of all bivariate correlations.
Bivariate Correlations Among Psychiatric Symptoms, Cognitive Functioning, and Functional Capacity Domains (N = 452).

Note. BAI = Beck anxiety inventory (higher scores indicate higher levels of anxiety symptoms); GDS-SF = geriatric depression scale, short form (higher scores indicate higher levels of depression symptoms); MMSE = mini mental status exam (higher scores indicate better cognitive functioning); RBANS = repeatable battery for the assessment of neuropsychological status (higher scores indicate better levels or cognitive functioning). TFLS = Texas functional living scale (higher score indicates better functional capacity); IADL = instrumental activities of daily living questionnaire (higher score indicates a higher number of problems with completing instrumental activities of daily living and therefore lower functional capacity).
Correlation is significant at p < .01.
In summary, findings revealed a significant association between chronic pain and all outcome variables, indicating that chronic pain contributes uniquely to mental health, functional capacity, and cognitive performance beyond the influence of demographic characteristics.
Discussion
Interpretation of Study Results
The findings of the current study have revealed significant associations among chronic pain, psychiatric symptoms, cognitive functioning, and functional capacity in older adults. Participants who reported chronic pain exhibited significantly higher levels of depression and anxiety compared to those who denied chronic pain, after adjusting for demographic variables and the number of other medical conditions. Additionally, chronic pain explained unique variance in all outcome variables above and beyond demographics and health status. These findings highlight the significant role of chronic pain as an independent predictor of mental health, functional capacity, and cognitive performance. Results suggest that chronic pain may exacerbate anxiety and depression, interfere with one’s ability to perform daily activities, and even impair cognitive abilities.
These results are in line with existing literature that consistently reports a positive correlation between chronic pain and psychiatric symptoms (Brooks et al., 2019; Domenichiello & Ramsden, 2019), as well as cognitive impairment (Bell et al., 2022) and diminished functional capacity (Dueñas et al., 2020; Puto et al., 2023; C. S. Ritchie et al., 2023). However, the present study extends the existing literature by quantifying the magnitude of these associations with specific effect sizes, providing a more granular understanding of the severity of these outcomes. Additionally, a distinctive aspect of this study is its comprehensive assessment of psychiatric, cognitive, and functional outcomes within a single sample, providing an integrated perspective on the complex impacts of chronic pain across several domains of functioning.
Psychiatric Symptoms
The magnitude of the association between chronic pain and psychiatric symptoms (depression and anxiety) was the highest (ΔR2 range: .079-.098), followed by measures of functional capacity and then cognitive functioning. This finding is generally consistent with extant literature (e.g., C. S. Ritchie et al., 2023) and indicates that individuals experiencing chronic pain may be more profoundly affected in their mental health than in their cognitive abilities. The larger effect sizes for psychiatric variables suggest that chronic pain may lead to heightened emotional distress and psychological burden, potentially exacerbating feelings of hopelessness and anxiety. This could be due to the persistent nature of pain, which can create a cycle of negative thought patterns and emotional responses.
Screening for mental health concerns in older adults with chronic pain is vital in light of the risk of suicide in this population (Bryan et al., 2021; Ratcliffe et al., 2008). According to multiple studies, it is evident that chronic pain is associated with an increased risk for depressive episodes (97%), anxiety disorders (36%), and suicidal behaviors, especially in geriatric populations (e.g., Costanza et al., 2021; Xue et al., 2023). A recent systematic review indicates that lack of adherence to recommended treatments tends to be associated with chronic pain, depression, and increased risk of suicide in older adults (Pakniyat-Jahromi et al., 2022). Given these findings, it is crucial to prioritize comprehensive mental health screening and support for older adults with chronic pain to mitigate these significant risks and enhance overall well-being.
Functional Capacity
Effect sizes for the measures of instrumental activities of daily living were generally in the medium range (ΔR2 range: .033-.077); specifically, individuals reporting chronic pain displayed decreased functional capacity when compared to participants who denied chronic pain. This complements existing literature that has identified chronic pain as a risk factor for diminished functional autonomy, potentially leading to increased dependence on others for daily living activities (Domenichiello & Ramsden, 2019; E. K. Ritchie et al., 2022). The reduction in functional capacity may be attributable to the direct physical limitations imposed by pain as well as the secondary effects of depressive and anxious symptomatology, which can further inhibit engagement in daily activities (Baker et al., 2016; de Heer et al., 2014).
Chronic pain in older adults can lead to a sense of fear of increased pain or injury, which in turn leads to an avoidance of physical activity and increased overall physical deconditioning (Coyle et al., 2017). This cycle can result in a decreased functional capacity and ability to complete desired activities. According to E. K. Ritchie et al. (2022, p. 32), “7.8 of 12.3 million older adults in the US with persistent pain experienced a decrease in function over seven years.” This decrease in functionality can be directly related to older adults’ ability to live independently. Thus, findings underscore the importance of addressing chronic pain not only for pain management but also for preserving functional autonomy and promoting independent living among older adults.
Cognitive Functioning
In terms of cognition, the observed effect sizes for cognitive measures were small to medium (ΔR2 range: .020-.059). Specifically, cognitive functioning was significantly reduced in those who were experiencing chronic pain compared to the group without. This includes mental status measures and global difficulty in initial learning of new information and delayed recall of that same information. It is important to note that there is evidence of average performance with recognition tasks or cued memory recall. Additionally, performance on subtests of processing speed, visuospatial skills, and verbal fluency were significantly lower in the group reporting chronic pain. The observed inverse relationship between chronic pain and cognitive functioning highlights the cognitive toll of chronic pain, suggesting that the persistent experience of pain may occupy cognitive resources, thereby impairing performance on tasks requiring attention, memory, and executive functioning (Ding et al., 2021; Moriarty et al., 2017; Simon et al., 2016). Our results lend further support to this cognitive interference hypothesis.
Clinical Implications
In the context of providing clinical care to older adults with chronic pain, this study highlights the prevalence of adverse mental health outcomes, cognitive concerns, and limitations in functional capacity in those reporting chronic pain. The enduring nature and adverse effects of unmanaged chronic pain may lead to a harmful downward cycle of poorer overall quality of life, pain-related disability, and coexisting conditions. Healthcare providers may prevent this occurrence and instead prompt improvement by conducting thorough evaluations in collaboration with healthcare teams and implementing holistic, integrative care plans.
When caring for older adults in the context of chronic pain, factoring in sufficient time to complete a comprehensive assessment should help facilitate an unhurried, effective session. The assessment will aim to identify possible etiologies of pain, levels of anxiety and depression, and the impact of pain on cognition, physical function, and quality of life. Integrated care models for chronic pain management in elderly adults with coexisting conditions can be very beneficial in this population (Jiang & Liu, 2023). Integrative care models address multifaceted aspects of chronic conditions in older adults. There are various programmatic approaches to integrated care that may address the physical nature of pain and the psychological, social, and functional impacts in a variety of ways (Department of Medical Assistance Services [DMAS], 2024). Coordinated access to services is a key element of integrative care models. These models emphasize the importance of integrating various healthcare services and support systems to effectively manage chronic conditions in older adults—including chronic pain—while minimizing the burden of accessing those systems for the recipient.
Patients can be heavily focused on the functional impact of pain and desire to alleviate symptoms, so it may be necessary to help the patient understand why other factors such as social support, anxiety, and depression are being addressed in their treatment plan. In addition to the general or geriatric practitioner, patient, and their significant others, the interdisciplinary team may include a variety of interdisciplinary health professionals who can play a crucial role in conducting ongoing assessments and follow-ups, as well as general care coordination. Employing safe, effective integrative therapies into the care plan is particularly important in older adults due to the natural physical changes that occur with age. Treatment planning must address underlying mechanisms of pain that are unique in the aging adult to develop safer and more effective treatment options (Domenichiello & Ramsden, 2019). Educating older adults with chronic pain about efficacious complementary treatment options and the correct use of treatments is important for achieving safe pain reduction (McDonald & Walsh, 2022). The impact of multisite chronic—particularly neuropathic—pain on functional outcomes in older adults underscores the importance of considering biopsychosocial aspects in treatment approaches (Butera et al., 2019).
Chronic Pain and Combined Outcomes
The results of the multivariate analysis of covariance (MANCOVA) revealed a significant relationship between chronic pain and the combined outcome of psychiatric symptoms, cognitive functioning, and functional capacity. Specifically, chronic pain accounted for 15.8% of the variance in these combined outcomes, after controlling for key demographic and medical covariates. This finding emphasizes the important role of chronic pain as an influential factor across multiple domains of functioning. It also aligns with existing research suggesting that chronic pain is a physical condition that also impacts mental and cognitive health. Bivariate correlations further supported this conclusion, as significant relationships were observed between psychiatric symptoms and both cognitive functioning and functional capacity.
Specifically, the interrelations among psychiatric symptoms, cognitive functioning, and functional capacity domains (as demonstrated by significant bivariate correlations) underscore the comprehensive impact of chronic conditions on individual’s overall health. The findings demonstrate that higher levels of anxiety and depressive symptoms are associated with lower cognitive performance and decreased functional capacity, aligning with previous literature suggesting the widespread effects of psychiatric symptoms on daily functioning and cognitive health (Stogmann et al., 2016; Sweetman et al., 2024). This interconnectedness supports the need for holistic treatment approaches that address mental health symptoms while considering cognitive and functional capacities, particularly in individuals with chronic pain.
The current findings also emphasize the likelihood of a multi-directional relationship among chronic pain, psychiatric symptoms, cognitive functioning, and functional capacity. Chronic pain has been shown to exacerbate symptoms of anxiety and depression, which in turn may lead to deficits in daily functioning or cognitive performance (Castel et al., 2021; De La Rosa et al., 2024; Delgado-Gallén et al., 2021; Moriarty et al., 2017). In turn, cognitive impairments may reduce an individual’s ability to perform daily tasks, thereby diminishing their functional capacity (Ord et al., 2021). This cascading effect suggests that chronic pain may not only affect each of these domains directly, but it may also indirectly contribute to declines in functioning through its impact on mood and cognition. Such complex interconnections support a biopsychosocial model of chronic pain, which posits that physical, psychological, and social factors interact to influence pain and associated health outcomes (Miaskowski et al., 2020). Therefore, addressing only one domain in treatment may be insufficient, as unaddressed psychiatric symptoms or cognitive impairments could significantly affect functionality and the quality of life in individuals with chronic pain.
Limitations and Directions for Future Research
The present study has a number of limitations. A notable constraint is the reliance on a cross-sectional design, which precludes the ability to infer causality or the directionality of the observed relationships. Additionally, the generalizability of the findings may be limited due to the specific demographic and clinical characteristics of the study sample. Furthermore, selection bias may arise from the referral process for outpatient neuropsychological evaluations, as the individuals included in the study were drawn from an outpatient clinic in Virginia, and most individuals were referred by their primary care provider or a neurologist for a neuropsychological evaluation due to cognitive concerns. This may not represent the broader population of older adults with chronic pain, as those referred for an evaluation may have more significant symptoms or different health characteristics than those who are not referred.
Additionally, the study utilized a singular dichotomous measure of self-reported pain concerns that did not capture the complex nature of chronic pain, which can vary greatly in intensity, quality, and duration. Furthermore, the study did not account for all potential confounding factors (e.g., duration of chronic pain, comorbid medical conditions, and social support), all of which can influence pain perception and its psychological consequences. Future research should aim to address these limitations by employing longitudinal designs, including more diverse samples, and employing more detailed measures of pain. Exploring long-term outcomes of multi-disciplinary integrative pain management strategies and individual studies on the effectiveness of alternative and complementary therapies are all areas of opportunity surrounding this topic.
Conclusion
Overall findings revealed that older adults reporting chronic pain had significantly higher levels of depression and anxiety. Additionally, this group exhibited reduced functional capacity and neurocognitive functioning. Chronic pain explained unique variance in all outcome variables (psychiatric symptoms, functional capacity, and cognitive functioning) beyond demographic characteristics and other medical conditions. These results underscore significant associations of chronic pain with multiple dimensions of health in the older adult population, highlighting the importance of addressing pain in this demographic to potentially improve multiple aspects of their psychological health, cognition, and daily functioning.
Footnotes
Author Note
The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as an official Regent University position, policy, or decision, unless so designated by other official documentation, nor should they be construed as an official Veterans Affairs position, policy, or decision, unless so designated by other official documentation. Dr. Anna T. Magnante is now affiliated with Cascade Neuropsychology, Bellingham, WA, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Salisbury VA Health Care System, VA Mid-Atlantic (VISN 6) Mental Illness Research, Education, and Clinical Center (MIRECC), and the Department of Veterans Affairs Office of Academic Affiliations Advanced Program in Mental Illness, Research, and Treatment. This work was also supported by Hampton Roads Neuropsychology and Faculty Research Grant titled “Lifestyle Factors and Cognitive Functioning in Older Adults” funded by Regent University.