
Abstract
Introduction
While the demographics of the human population have been evolving steadily for many years, it seems that by 2050 the number of people aged over 60 will account for 21.1% of our population, compared to 9.2% in 1990. Our aging population is a major public health issue (Mareschal & Genton, 2014; Sander et al., 2015). Thus, gerontology receives special attention, and aging well is becoming an increasingly central thematic area. Currently, encouraging regular physical activity is one of the main recommendations for non-drug interventions to promote successful aging. It is therefore recommended, that older people should take part in a variety of physical activities of moderate to higher intensity three or more times a week (Vogel et al., 2009; WHO, 2022). In an ageing population, physical activity is essential for a healthy body and mind. More precisely, it has been shown that practicing a physical activity regularly has beneficial effects on health: improved psychological and physical health, improved sleep, reduced prevalence of common chronic diseases, reduced cognitive decline and lower mortality rates (Koster et al., 2018; Mareschal & Genton, 2014; Musich et al., 2017; WHO, 2022). Today, several interventions such as fitness/gentle gymnastics, walking, yoga, muscle-strengthening and endurance exercises and domestic physical activities are proposed to improve the physical health of older adults including people with dementia (Taylor et al., 2004). Indeed, programs aiming to help improve the health of the older adults are emerging. In a recent multi-center randomized controlled trial, the Vivifrail program promoting physical activity was tested on frail people over 75 years old suffering from mild cognitive impairment. It was shown that this program brought significant gains in terms of functional capacity, and also significant effects on the cognitive sphere, muscular functions and depression (Casas-Herrero et al., 2022). Most of these interventions take place at home, in a gym or community hall or at an institution and are supervised by a qualified certified professional. Nevertheless, currently other emerging interventions contribute to maintaining and/or improving the physical health of older adult and take place outdoors in a natural environment. This combines the beneficial effects of these interventions with those of nature (light, fresh air, the view of nature, etc.), providing a natural setting that can be perceived as relaxing (Bachi et al., 2012; Thompson Coon et al., 2011). Moreover, many authors have observed positive links between reconnection with nature and improved quality of life (Fields et al., 2018; Hansen et al., 2017; Mygind et al., 2021; Rappe et al., 2006). Indeed, Equine-Assisted Intervention (EAI) is an example of this type of activity. It combines the positive effects of human interaction with horses with those of nature, at the same time aiming to promote people’s physical or psychological health (all ages). According to De Santis et al. (2017) EAI is “an umbrella term that incorporates programs that aim to improve human health and wellbeing. These interventions are based upon the emotional/physical relationship that is established between the human being and the horse.” Furthermore, EAI serve multiple purposes, as they can encompass therapeutic objectives (EAT: Equine-Assisted Therapies) or recreational objectives (EAA: Equine-Assisted Activities). While EAI have proven their effectiveness with a diverse population (Borgi et al., 2016; Earles et al., 2015; Nurenberg et al., 2015; Pálsdóttir et al., 2020), they represent a new therapeutic area for promoting physical health in older adults (Badin et al., 2022; Hilière et al., 2018; Prieto et al., 2020; White-Lewis et al., 2017). Studies have investigated the effects of EAI on the health of people with disabilities and found that benefiting from an EAI program increased exercise tolerance, quality of life, mobility and interpersonal interactions and relationships (Prieto et al., 2020). Concerning older adults, White-Lewis et al. (2017) demonstrated a significant reduction in physical pain after EAI in older adult arthritis sufferers. In addition, within the same population, Hilière et al. (2018) highlighted that benefiting from an EAI program impacted on both the physical domain (improved balance, mobility, gait ability and muscular strength) and physiological domain (observations of hormonal and cerebral changes). These results are in accordance with a recent systematic review (Badin et al., 2022). Results of this systematic review have highlighted the benefits of EAI on older adults’ physical health, reflected in improved balance, gait and muscular strength. The beneficial effects of EAI on physiology (hormonal changes inducing a state of relaxation) and psychology (increased pleasure and quality of life) have also been demonstrated. To sum up, most studies demonstrate positive effects of EAI on physical health in older adults. Despite the emergence of promising results on the benefits of EAI, the poor methodological quality of the studies (lack of control group, lack of follow-up of individuals, untrained professionals, small sample, etc.) which has been pointed out in many reviews means that conclusive effects cannot yet be claimed (Badin et al., 2022; Hilière et al., 2018; Prieto et al., 2020; White-Lewis et al., 2017). Considering the importance of good physical health in the older population (better performance in daily activities, reduced risk of falls, reduced loss of autonomy, etc.), the aim of this study was to conduct a meta-analysis to provide a more accurate and robust estimate of the effects of EAI on older adults’ physical health.
Methods
Search Strategy
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Page et al., 2021). To carry this out, the authors conducted a literature search using the following electronic databases: Cochrane Library, EMBASE, Medline (PubMed) & PsycINFO, and those with no date limit. The following search terms (MeSH) were used for this step: [“equine assisted therapy” OR “therapeutic horse riding” OR “therapeutic horseback riding” OR “hippotherapy” OR “equine psychotherapy” OR “equine facilitated therapy” OR “equus” OR “horse therapy” OR “equine assisted intervention”] AND [aged “older adult*” OR aged OR elderly]. The final search date ranged from the inception of each database up to January 2024.
The inclusion criteria for this study were as follows:
(1) Participants were at least 60 years old.
(2) Interventions: EAI oriented experimental intervention, either therapeutic (EAT) or recreational (EAA).
(3) Presence of a control group which received non-equine assisted interventions.
(4) Outcomes of physical health measures (aspects related to physical functions, such as balance, gait and muscle strength).
(5) Interventional studies (study design): Randomized controlled trials (RCT) or non-randomized controlled trials (NRCT).
(6) Studies written in English.
Data Collection
Study data were extracted by two reviewers (NB and LB) using a standard form. The data extracted included: (1) Publication details: authors, publishing year, countries, (2) nature of interventional studies (RCT Table 1 and NCRCT Table 2), (3) study aims, (4) Participants: sample size, mean age of participants, percentage of female participants, (5) Group activities: contents, sessions, frequency, and duration, (6) Characteristics of EAI sessions, (7) measures of physical health, (8) main findings.
Summary Table of Evidence RCT.

Note. BBS = Berg Balance Scale; CG = control group; COP = center of pressure; EAA = equine assisted activities; EAT = equine-assisted therapy; FRT = functional reach test; ns = non-significant; TE = traditional exercise; TR = treadmill; TUG = times up and go; 30CST = 30-s chair stand test.
(+): significant difference (post-test > pre-test); (−): significant difference (post-test < pre-test).
Summary Table of Evidence NRCT.

Note. BBS = Berg Balance Scale; CG = control group; COP x = center of pressure (medio-latera); COP y = center of pressure (anterio-posterior); EAT = equine-assisted therapy; ns = not significant; TUG = times up and go; 30 CST = 30-s chair stand test.
The flow diagram PRISMA (Figure 1) highlights the process of reviewing the articles in this meta-analysis according to inclusion and non-inclusion criteria.

The PRISMA flow diagram for search strategy.
Quality Assessment
For each study, two reviewers (EVD and GV; GG and KP; NB and OA) evaluated independently the quality of the studies included. Any disagreements between the reviewers were resolved through discussion. The RCTs were evaluated using the revised Cochrane Risk of Bias tool (RoB2; Higgins et al., 2011). The ROB was judged as low, moderate, high, or unclear for each of the following domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the result reported and overall bias. For NRCT, the Risk of Bias tool for non-randomized studies of interventions (ROBINS-I, Sterne et al., 2016) was used. The domains and the overall ROB were judged as low risk, some concerns or high risk (Table 3).
Risk of Bias Domains: (a) RCT Using RoB and (b) NRCT Using ROBINS.


Domain 1 Bias arising from the randomization process; Domain 2 Bias due to deviations from intended intervention; Domain 3 Bias due to missing outcome data; Domain 4 Bias in measuring the outcome; Domain 5 Bias in selecting the result reported.


Domain 1: Risk of bias due to confounding; Domain 2: Risk of bias arising from measurement of the exposure; Domain 3: Risk of bias in selecting participants for the study (or in the analysis); Domain 4: Risk of bias due to post-exposure interventions; Domain 5: Risk of bias due to missing data; Domain 6: Risk of bias arising from measurement of the outcome; Domain 7: Risk of bias in selecting the result reported.
 LOW RISKS
LOW RISKS  SOME CONCERNS
SOME CONCERNS  HIGH RISKS.
HIGH RISKS.
Statistical Analysis
The meta-analysis was carried out using Review Manager 5.4 using random effects models and results were presented as a forest plot. Because the outcomes were continuous variables, the standardized mean difference (SMD) and SD between pre and post-intervention within groups were used to calculate the total effect size (Cohen’s d). An overall combined effect size with a 95% confidence interval was calculated. Statistical heterogeneity between studies was tested using I² statistics (I2 low: 25%; I2 moderate: 50%; I2 high: 75%) (Higgins et al., 2003).
Results
Studies and Subject Characteristics
A total of 264 articles were selected after our initial search in the databases. Among these articles, 18 duplicate records were excluded by Excel. In the screening phase, 114 articles were selected for full-text review. In the end, only six of these 114 articles were included in this meta-analysis, of which four were randomized controlled trials. Details of this search strategy are shown in Figure 1.
The six studies selected were published between 2011 and 2020, three of them were conducted in Brazil (Araujo et al., 2011, 2013; Diniz et al., 2020), one in Korea (Kim et al., 2014), one in Spain (Aranda-Garcia et al., 2015) and one in the United States (Homnick et al., 2013). The total sample included 150 people (71% women, n = 107), 64 in experimental groups and 86 in control groups. Sample sizes ranged from 38 to 15 people. Mean age ranged from 65.7 to 71.53 years. The participants were free of any pathology (Aranda-Garcia et al., 2015; Araujo et al., 2011, 2013; Diniz et al., 2020; Homnick et al., 2015; Kim et al., 2014). Data from these six studies are presented in Tables 1 and 2.
Intervention Characteristics
Regarding the experimental groups in these studies, the proposed EAI programs can be divided into two categories: (1) Five studies proposed programs with a therapeutic focus, that is, Equine Assisted Therapies (Araujo et al., 2011, 2013; Diniz et al., 2020; Homnick et al., 2015; Kim et al., 2014) conducted by a qualified professional, usually from the health field, with specific health objectives. (2) The remaining study proposed a program with a less therapeutic focus, that is, Equine Assisted Activities (Aranda-Garcia et al., 2015). Most EAI sessions (n = 4) took place at an equine therapy center (Araujo et al., 2011, 2013: Diniz et al., 2020: Homnick et al., 2015) and one in a riding center (Aranda-Garcia et al., 2015). One study did not provide information on the location of sessions (Kim et al., 2014). The duration of the various EAI was 8 to 12 weeks, conducted once to three times a week with sessions ranging from 20 to 60 min. Overall, the total duration of the EAI programs ranged from 10 to 36 sessions (20, 67 ± 12, 18), this represents EAI programs ranging from 5 to 36 hr of practice. Tables 1 and 2 summarize the content of the sessions.
Regarding the control groups in these studies, the interventions varied: for four studies they involved activities of daily living (i.e., no specific intervention) (Araujo et al., 2011, 2013; Diniz et al., 2020; Homnick et al., 2015); in one study, the control group followed 36 twenty-minute sessions on a treadmill over 12 weeks (Kim et al., 2014); the remaining study involved two control groups: one with no intervention, with the participants carrying out daily living activities, and the other in which participants carried out 16 sixty-minute sessions of traditional physical exercise over 12 weeks (Aranda-Garcia et al., 2015).
Physical Measures
The articles selected for this study focused on three main areas: balance, gait, and muscular activity:
Of the six articles selected, all evaluated the effect of EAI on balance via several tests (Aranda-Garcia et al., 2015; Araujo et al., 2011, 2013; Diniz et al., 2020; Homnick et al., 2015; Kim et al., 2014). The tools used were: Berg Balance Scale (Araujo et al., 2013; Diniz et al., 2020; Homnick et al., 2015), Fullerton Advanced Balance scale (Homnick et al., 2015), Functional Reach Test (Diniz et al., 2020), Platform utilization for estimation of balance – Center of Pressure (Aranda-Garcia et al., 2015; Araujo et al., 2011) and Sway path length (Kim et al., 2014). Five out of the six articles evaluated the effects of EAI on gait in the older adults (Aranda-Garcia et al., 2015; Araujo et al., 2011, 2013; Diniz et al., 2020; Kim et al., 2014). The instruments used were: Timed Up and Go (Araujo et al., 2011, 2013; Diniz et al., 2020), the maximal gait speed (m/s) on a marked 16-m walkway (Aranda-Garcia et al., 2015), and step length (cm) and step time (s) using a gait analyzer (Kim et al., 2014). Finally, three out of the six articles assessed the effects of EAI on the older adults’ muscular activity (Aranda-Garcia et al., 2015; Araujo et al., 2013; Diniz et al., 2020). The instruments used were: assessment of arm and leg muscle strength using a handgrip and knee extensor (Aranda-Garcia et al., 2015), the 30s Chair-Stand-Test (Araujo et al., 2013) and the Sit and Reach Test (Diniz et al., 2020).
Effect of Equine-Assisted Interventions on Physical Health
Within this meta-analysis, all the articles focused on the effect of EAI on the older adults’
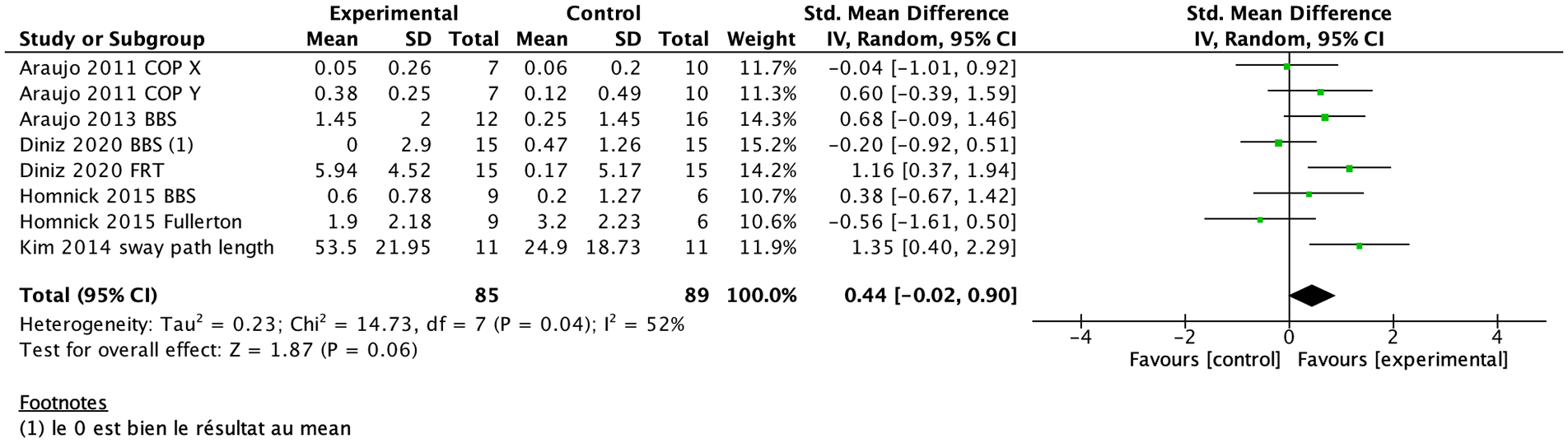
Meta-analyses examining the impact of EAI on the balance of older adults.
Five out of six studies assessed the effects of EAI on the older adults’ gait (Aranda-Garcia et al., 2015; Araujo et al., 2011, 2013; Diniz et al., 2020; Kim et al., 2014). Of these five articles, two showed no effect on gait when the Timed Up and Go and the step length/time were used (Araujo et al., 2013; Kim et al., 2014), while two other articles demonstrated a significant positive effect of EAI on gait, only the Timed Up and Go was used (Araujo et al., 2011; Diniz et al., 2020). Only Aranda-Garcia et al. (2015), showed a significant group by time interaction, in terms of maximal gait speed, the EAI group had a significantly higher maximal gait speed than the control group. The meta-analysis demonstrated that the experimental groups showed a significant improvement in gait compared to the control groups (SMD = 0.93, 95% CI [0.41, 1.44], p = .0004). It revealed a moderate degree of heterogeneity, with an I2 corresponding to 50%. Figure 3 shows the results presented as a forest plot of the five articles.

Meta-analyses examining the impact of EAI on the gait of older adults.
Finally, three out of the six studies assess the effects of EAI on the older adults’ muscular activity (Aranda-Garcia et al., 2015; Araujo et al., 2013; Diniz et al., 2020). Among these three articles, two showed a significant positive effect of EAI on muscular activity, the tests used were the 30s Chair-Stand-Test and the Sit and Reach Test (Araujo et al., 2013; Diniz et al., 2020). For Aranda-Garcia et al. (2015), mixed results were observed. Regarding knee extensor strength: significant positive results were observed in both the EAI and control groups (traditional exercises). Regarding the handgrip, the control group showed greater improvement than the EAI group. The meta-analysis demonstrated that the experimental groups showed a significant improvement in muscular activity compared to the control groups (SMD = 0.90, 95% CI [0.11, 1.70], p = .03). It revealed a high degree of heterogeneity, with an I2 corresponding to 75%. Figure 4 shows the results presented as a forest plot of the three articles.

Meta-analyses examining the impact of EAI on the muscular activity of older adults.
Qualities of the Studies
Table 3 summarizes the results of the bias and methodological quality assessments for all the studies. Out of the four RCTs identified, half were classified as having high risk of bias and half with “some concerns” in all domains. Two studies presented a risk of bias in three or four of the five ROB domains (Diniz et al., 2020; Kim et al., 2014). Concerning the two NRTCs identified, risk of bias was high for Araujo et al. (2011), whereas there were “some concerns” for Homnick et al. (2013).
Discussion
Summary of Main Findings
The aim of this study was to investigate the effects of EAI on the physical health of individuals who were 60 years old and over. To this end, a meta-analysis was carried out, providing a more accurate and robust estimate of the effects of EAI on this population. To our knowledge this study is the first to measure the effects of an EAI program on the physical health of older adults. Indeed, most studies have investigated EAI in a younger age group (Heussen et al., 2022; Tseng et al., 2013; Wang et al., 2015; Zadnikar et al., 2011). The main result of this meta-analysis highlights a positive impact of EAI on older adults’ physical health. More specifically, the adoption of an EAI program was shown to significantly improve their gait and muscle activity.
Concerning gait, this meta-analysis underlines the benefits of an EAI program on older adults’ gait. These results are consistent with those found in the literature in young people with spastic cerebral palsy or in adults with multiple sclerosis and chronic brain disorders (Kwon et al., 2011; McGibbon et al., 1998; Muñoz-Lasa et al., 2011; Sunwoo et al., 2012). Our results are also in line with those of other studies carried out in an older population (Aranda-Garcia et al., 2015; Araujo et al., 2011, 2019; Berardi et al., 2022; Diniz et al., 2020). There are several possible explanations for this positive result. Firstly, participants in EAI programs significantly increased their step count due to the extensive spaces in equestrian centers, which encouraged them to cover longer distances. Secondly, EAI programs offer a wide variety of activities, including sessions requiring the older adults to walk (e.g., the participant walked with the horse, carried out exercises on foot over a course, etc.) thus contributing to their improved gait (Pothier et al., 2021).
Regarding muscular activity, this meta-analysis demonstrates the positive effects of an EAI program on this aspect. Our findings are consistent with data from studies in the literature on young and older adults (Aranda-Garcia et al., 2015; Araujo et al., 2013, 2019; Benda et al., 2003; de Mello et al., 2022; Diniz et al., 2020). Several factors may explain this result. Firstly, walking activities include movements that call upon various muscle groups, thus contributing to muscle strengthening and toning, with particular emphasis on the lower limbs. In this way, not only the content of the EAI program, but also the environment of the equestrian center (wide open spaces) impact directly on muscle activity. Secondly, during EAI sessions, the participant may be encouraged to practice rising trot when the horse trots involving alternating a sitting and standing position synchronized with the horse’s movements. This posture leads to increased knee (Aranda-Garcia et al., 2015) and thigh muscle activity. Thirdly, a final factor seems to explain the benefits of EAI for both gait and muscle activity, two elements that would seem to be linked since the lack of activity of some muscles in the lower limbs could have an impact on gait performance (Kirkwood et al., 2011). These benefits could be explained by the movements imposed by the horse when the person is riding. A horse can take up to 3,300 steps in a 30-minute session, requiring the rider to make precise postural adjustments with each step. Indeed, from a biomechanical point of view, the horse’s movement during different gaits requires a three-dimensional displacement of the rider’s pelvis in the sagittal, frontal, and transverse planes. Thus, the movement of the horse provides the rider with physical and sensory feedback, replicating the movement of human walking and resulting in improved posture, muscle strength and balance (Koca & Ataseven, 2016; McGibbon et al., 1998).
With regards to balance, this meta-analysis does not reveal any beneficial effects of an EAI program on older adults’ balance, in contrast to the literature which points to notable improvements in balance at all stages of life (Araujo et al., 2011, 2013, 2019; Berardi et al., 2022; de Milander et al., 2016; Kim et al., 2014). However, two studies conducted with an older population seem to corroborate our findings (Aranda-Garcia et al., 2015; Homnick et al., 2015). This lack of results can have two possible explanations. Firstly, it is possible that the baseline level of balance among participants was high. Indeed, in this meta-analysis, participants were largely independent, which could explain why improvements were not significant. Secondly, studies included in this meta-analysis were conducted on small sample sizes. Indeed, Rydwik et al. (2004) highlighted that studies with samples of fewer than 50 individuals did not show significant results in the field of balance.
Finally, in general the results of our meta-analysis agree with those of the literature, but there are several points to bear in mind when interpreting them. Firstly, the double inclusion of articles within this meta-analysis could introduce a bias in the estimation of the overall effect. Secondly, regarding the heterogeneity of EAI programs, their objectives varied (EAT vs. EAA), sessions were conducted either on horse-back or on foot (next to the animal), and their duration/frequency varied from one program to another (ranging from 10 to 36 sessions), thus making it difficult to compare and generalize results. The current lack of a standardized method for this type of intervention is a real challenge. Thirdly, the low number of participants in studies (NRCT but also RCT) should also be considered. Indeed, most of the studies were limited by small sample sizes and the lack of blinding of participants and assessors which can affect results. For these reasons, using more rigorous protocols will be necessary to confirm the results of this type of intervention.
Implications for Practice and Future Research
This article highlights the benefits of EAI on older adult physical health. The results seem to confirm the ability of this type of program to improve their gait and increase muscular activity, opening up the prospect of clinical implications. This analysis suggests that integrating an EAI program could be considered as a therapeutic approach complementary to usual care in accompanying older adults, potentially reducing the risk of falls, a major factor in the onset of dependency and subsequent institutionalization (Lopez-Tourres et al., 2012). Moreover, the fact that engaging in physical activity can reduce the risk of older adults falling results in improving their quality of life (Nowalk et al., 2001). Future studies should assess not only individual’s fear of falling but also the actual number of falls within cohorts. This would enable us to clarify the real benefits of an EAI program on the risk of falls in older adults. To respond to these challenges, EAI and gerontology professionals are encouraged to work closely together. This interdisciplinary collaboration is deemed essential for designing EAI programs adapted to the specific needs of an older population, thus promoting their physical well-being, and contributing to an overall improvement in their quality of life. It is important to note that the participants selected for review in this study were generally in good health, emphasizing the need for future research to involve older adults with chronic disease or neurodegenerative disorders, such as Alzheimer’s disease.
Conclusion
Our results suggest that benefiting from an EAI program appears to be an effective alternative to improve older adult physical health. From a public health perspective, our findings emphasize the importance of physical activity for the older population, suggesting that implementing an EAI program could help reduce the risk of falls and the overall quality of life of older adults. It is important to note that the benefits may vary depending on the older person’s initial physical condition and specific needs, as well as the importance they attach to this type of intervention. To deepen our understanding of these beneficial effects, further research is required on this topic.
Footnotes
Acknowledgements
Thank you to the Fondation Médéric Alzheimer for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study did not require approval from an ethics committee, as it is based on pre-existing data from the literature.