
Abstract
Introduction
COVID-19 management has been a major burden to nursing homes and similar Long-Term Care Facilities (LTCFs; Rennert-May et al., 2023). Despite the widespread roll-out of COVID-19 vaccinations which have reduced transmission and severity within the general population, LTCF residents are at high risk for COVID-19 hospitalization (Muhsen et al., 2022). Those with pre-existing health conditions (e.g., chronic fatigue syndrome, chronic chest pain, and musculoskeletal joint pain) are at a higher risk for repeat infections by COVID variants (such as Delta summer 2021 and Omicron winter 2022 periods; Oordt-Speets et al., 2023; United States Government Accountability Office, 2023). Emerging COVD-19 variants continue to be an ongoing health risk to vulnerable older adult populations (Baker, 2023). For instance, a novel COVID-19 variant (EG.5) has been associated with a surge in hospitalizations in Texas (since August 2023) (Baker, 2023). The JN.1 is a prevalent COVID-19 strain since September 2023, requiring ongoing management of care needs of vulnerable populations (Idris & Adesola, 2024). Since the widespread availability of COVID-19 vaccinations beginning 2021, there has been a reduction in LTCF resident hospitalization overall (Benin et al., 2021; Nanduri et al., 2021), although the excess hospitalization reduction benefits for those with cognitive impairment have not been reported.
LTCF residents with dementia and a history of COVID-19 infection are particularly vulnerable to long-haul COVID-19 (Najar et al., 2023). Dementia is a progressive age-related memory impairment disorder on a continuum from moderate to severe (Reisberg, 1982). LTCF residents with dementia who contracted COVID-19 were three times likely to suffer from severe COVID-19 and risk for higher mortality in comparison with LTCF residents without dementia (Azarpazhooh et al., 2020; Brown et al., 2020; Hariyanto et al., 2021). However, their hospitalization care outcomes for older adults with dementia are less well known (Bianchetti et al., 2022), while important for improving ongoing care needs.
Hospitalization Care
Predominantly, dementia patients from LTCFs are hospitalized for severe respiratory disease (Guijarro et al., 2010; Zhou et al., 2021). In addition, due to cognitive decline, these patients encounter challenges in adapting to the hospital environment, and at higher risk for functional decline (Phelan et al., 2012). Challenges to dementia patients in their hospitalization care include the fact that medical surgical units and hospital staff often typically lack specialization in dementia management (Guijarro et al., 2010). For instance, care units may be less certain managing behavioral symptoms and complications of dementia such as risk for falls associated with delirium (Surr & Gates, 2017). In addition, dementia patients from LTCF facilities often have more comorbid conditions on admission (Bunn et al., 2014), requiring emergency care and longer hospitalization than would be without dementia (Louie et al., 2020).
Pre-existing Conditions
Hospitalization of residents from LTCF with dementia would vary by pre-existing health conditions (Amanat et al., 2021; Atkins et al., 2020). Prevalent health conditions in older adulthood associated with excess hospitalization risks include type 2 diabetes (Harb et al., 2021), hypertension (Wang et al., 2022), cardiovascular diseases (Huang et al., 2023), chronic kidney disease (Georgakopoulou et al., 2023), obesity (Lagrandeur et al., 2023), and chronic obstructive pulmonary disease (COPD; de Miguel-Diez et al., 2023). Moreover, older adults with dementia and long-haul COVID-19 were more vulnerable to stroke (Docherty et al., 2020; Roig-Marin & Roig-Rico, 2022), chronic blood loss (Al-Buthabhak et al., 2021), paralysis (Islamoglu et al., 2021), weight loss (Courtois-Amiot et al., 2023; Di Filippo et al., 2021), and neurological disorders (Alonso-Lana et al., 2020). Many of these conditions require emergency hospitalization of older adults with cognitive impairment from delays by carers in recognizing their developing care needs.
In summary, LTCF residents with dementia carry significant risk of hospitalization and mortality due to COVID-19 infection (Liu et al., 2021; Sun et al., 2023). Moreover, disparities in access to healthcare would exacerbate adverse medical outcomes among those with dementia (Udoh et al., 2023), including their risk for poorer COVID-19 hospitalization outcomes.
Sociodemographic and Health Insurance Status
Older adulthood (65 years and above) is a risk factor for both dementia and COVID-19 infection, portending higher risk for adverse hospital outcomes (Harb et al., 2021). By sociodemographics, being male and a racial minority (e.g., African American, Hispanic-Latino) with dementia was associated with increased likelihood of experiencing severe COVID-19 symptom and hospitalization rates (Chang et al., 2022; Meister et al., 2022). Historically, racial/ethnic minorities in the United States experience barriers to accessing healthcare and have higher rates of emergency hospitalization (Phillips et al., 2000). Disparities in health insurance status would contribute to the likelihood of adverse hospitalization among individuals with dementia and COVID-19. For instance, those with Medicare (for those older than 65 years,) poorer socio-economic status and those uninsured or underinsured lack access to adequate medical care (Luth et al., 2020; Udoh et al., 2023). It is thus important to understand the interaction of sociodemographics with health insurance status as risk for poorer COVID 19 hospitalization outcomes for those with dementia.
The Present Study
The current study aimed to determine COVID-19 hospitalization outcomes for LTCF residents with dementia, and the role of pre-existing health conditions in that relationship. Based on our conceptual model in Figure 1, we investigated the following research questions:
How do COVID-19 hospitalization outcomes of emergency hospital admission and length of stay in hospitals vary for LTCF residents with dementia diagnosis?
What are the differences in the risk of COVID-19 emergency admission and length of stay in hospital for LTCFs residents with dementia controlling for age, gender, and minorities?
What role do pre-existing health conditions play in COVID-19 emergency hospital admission and length of stay in hospital for LTCFs residents with dementia?

A conceptual framework.
Methods
Sources of Data and Participants Selection
The Texas Inpatient Public Use Data File (PUDF) was employed in this study.
The PUDF is a secondary dataset for the purpose of gathering hospital discharge data from all licensed hospitals in Texas. From this dataset, we sampled patients diagnosed with dementia aged over 60 years who were admitted to hospitals from long-term care facilities in Texas due to COVID-19 infection, selecting data from January 2020 to October 2022 (case group, n = 1,434). From the same dataset, we included a control group of 1,674 patients aged over 60 years without dementia admitted to hospitals from long-term care facilities in Texas due to COVID-19 infection. Table 1 provides an overview of socio-demographic, health conditions, and lifestyle characteristics of COVID-19 Infected LTCF patients, categorized based on dementia diagnosis.
Characteristics of COVID-19 Infected LTCF Patients by Dementia Diagnosis in Texas Between January 2020 and October 2022.

Note. LTC = long-term care; Medicare HMO = Medicare Health Maintenance Organization; CI = Commercial Insurance; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease.
This case control study within cross sectional data was not subject to Institutional Review Board (IRB) approval as it utilizes de-identified public-use data.
Measures
Predictor Variable
The dementia variable was extracted from the medical records and then dichotomously coded as 0 (without dementia) and 1 (with dementia).
Pre-existing Health Conditions
Pre-existing conditions included type 2 diabetes, hypertension, chronic kidney disease (CKD), cardiovascular diseases, obesity (defined as body mass index ranging from 30 and 39 kg/m2), chronic obstructive pulmonary disease (COPD), stroke, chronic blood loss, paralysis, weight loss, and neurological disorders that do not impact movement (e.g., epilepsy, mild cognitive impairment, and early stages of neurodegenerative disorders). Those variables were binarily coded based on either the admitting diagnosis, primary diagnosis, or 24 secondary diagnostic codes.
Lifestyle
We selected from the dataset the variables of malnutrition, heavy smoking and alcohol consumption. Malnutrition included various categories, such as iron deficiency and vitamin A deficiency. Heavy smoking comprised cigarette dependence and chewing tobacco dependency, excluding vaping. Heavy alcohol consumption encompassed alcohol dependence and alcohol abuse. Those variables were coded based on either the admitting diagnosis, primary diagnosis, or 24 secondary diagnostic codes.
Sociodemographic Variables
Demographic information of patients, including age, gender, and race/ethnicity, was obtained from medical records. Male gender and race/ethnicity were classified into binary variables (yes/no). Age was dichotomized and coded as 0 for the range of 60 to 74 years and as 1 for those aged 75 years or older.
Health Insurance
The patient’s health insurance coded in a binary manner, distinguishing between Medicare, Medicaid, Medicare Health Maintenance Organization (HMO), and charity insurance.
Dependent Variables
Dependent variables were COVID-19 Infection hospitalization status outcomes of Emergency Admission and length of stay (LoS) in hospital. The emergency admission variable was dichotomously coded as 0 (non-emergency admission) and 1 (emergency admission). The LoS was dichotomized into 1 to 5 days (shorter hospital stays) and ≥6 days (longer hospital stays) following Rees et al. (2020).
Data Analysis
All analyses were conducted using SPSS version 27. We utilized both crude and multivariate binary logistic regression models to determine risk factors associated with emergency admission and length of stay hospitalization outcomes among patients admitted from LTCFs due to COVID-19 infection. In our logistic regression models, we explored the potential confounding variables to result in a final model, including all identified risk factors from the initial crude analysis. We excluded from analysis percentage of cases that fell below 5%.
Results
Dementia Status and Hospitalization Outcomes
Tables 2 presents the general distribution of dementia, demographic and disease characteristics concerning emergency admission and longer hospital stays. Within the group of COVID-19 infected patients admitted from LTCFs, dementia was an independent factor significantly associated with both emergency admission and longer hospital stays. Patients with dementia exhibited nearly a two-fold increase in the likelihood of emergency admission (OR = 1.70; 95% CI [1.40, 2.06] and interestingly their odds of longer hospital stay reduced compared to those without dementia (OR = 0.64 [0.55, 0.74]), probably because they went back to the LTHF.
Characteristics of COVID-19 Infected LTCF Patients by Admission and Longer Hospital Stays Statuses in Texas Between January 2020 and October 2022.

Note. LTC = long-term care; Medicare HMO = Medicare Health Maintenance Organization; CI = Commercial Insurance; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease.
Demographics, Lifestyle, and Health Insurance Status
Tables 3 and 4 present the Odds-ratios (ORs) for dementia status, demographic and personal factors that exhibited statistically significant associations with COVID-19 emergency admission and longer hospital stay, respectively (see Figures 2A and B). For patients identifying as racial minority, the likelihood of experiencing COVID-19 emergency admission increased 30% (OR = 1.33; 95% CI = 1.01–1.75).
Dementia and Demographic Factors Associated with Admission Status Among COVID-19 Infected LTCF Patients in Texas Between January 2020 and October 2022.

Note. OR = odds ratio; 95%CI = ninety-five percent confidence interval; aAdjusted for Medicare HMO and African American; bMutually adjusted for all variables together in this table; bold *p < .05.
Dementia and Demographic Factors Associated with Longer Hospital Stays Among COVID-19 Infected LTCF Patients in Texas Between January 2020 and October 2022.

Note. OR = odds ratio; 95%CI = ninety-five percent confidence interval; aAdjusted for Age and Malnutrition; bMutually adjusted for all variables together in this table; bold *p < .05.
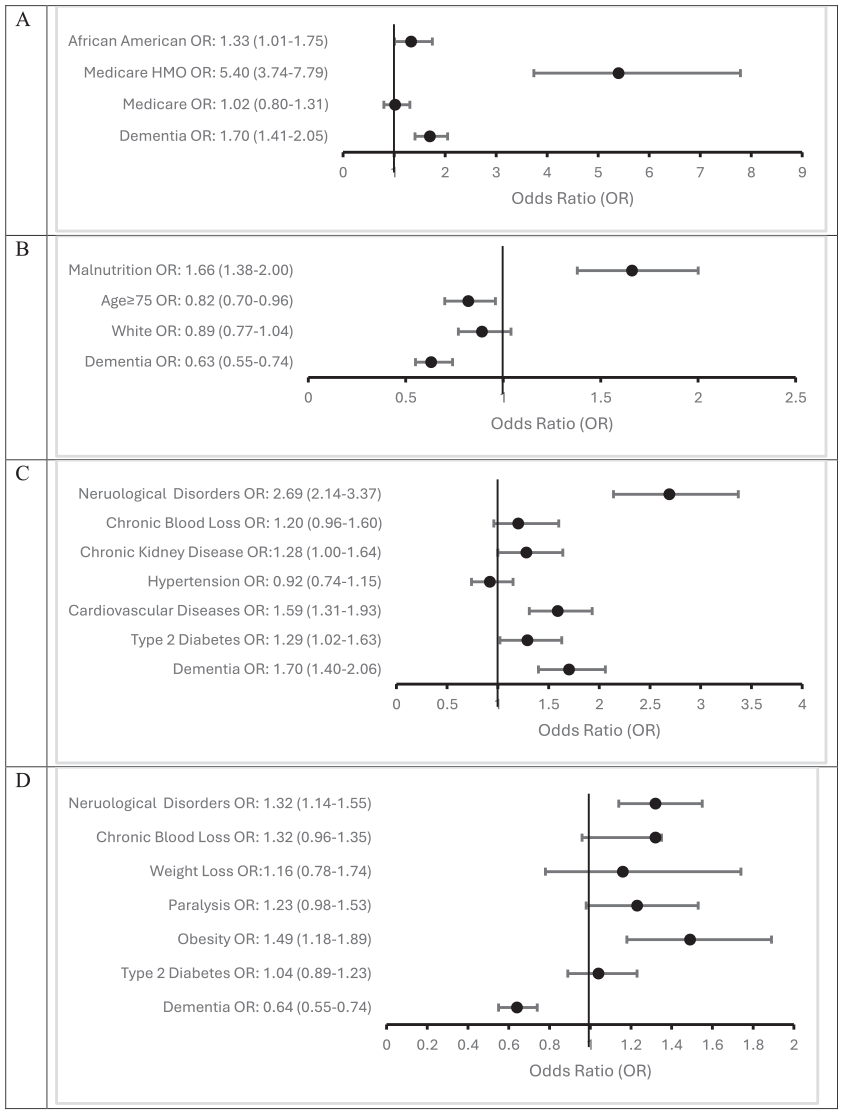
Relationship between dementia and demographic factors and admission status: (A) and longer hospital stays, (B); between dementia and health conditions and admission status, (C) and longer hospital stays, and (D) among COVID-19 infected LTCF patients in Texas between January 2020 and October 2022.
Patients aged over 75 years exhibited an 18% reduction in the likelihood of longer hospital stays (OR = 0.82; 95% CI = 0.70–0.96). Interestingly, our data did not reveal significant differences in age and gender between the groups with COVID-19 emergency admission and those without. Similarly, our data did not find significant differences in race and gender between the groups with shorter or longer hospital stays.
The possession of Medicare HMO coverage was associated with a significantly higher prevalence of COVID-19 emergency admission with dementia, with odds increasing five-fold (OR = 5.40; 95% CI = 3.74–7.79). By contrast, our analysis revealed that none of the health insurance plans were associated with length of hospital stay. Malnutrition was associated with almost a two-fold increase in the odds of longer hospital stays (OR = 1.66; 95% CI = 1.38–2.00). However, none of malnutrition, heavy smoking and alcohol exhibited significant associations with COVID-19 emergency admission.
Pre-existing Health Conditions
Tables 5 and 6 present the ORs of dementia and the health condition, highlighting their respective associations with emergency admission and longer hospital stays (see Figure 2C and D). Having any health conditions was associated with COVID-19 emergency admission with dementia, ranging from approximately 1.5-fold odds for type 2 diabetes (OR = 1.29; 95% CI [1.02, 1.63] and chronic kidney disease (OR = 1.28 [1.00, 1.64]) to approximately three-fold odds for neurological disorders (OR = 2.69 [2.14, 3.37]). Similarly, obesity (OR = 1.49 [1.18, 1.89]) and neurological disorders (OR = 1.32 [1.14, 1.55]) increased approximately 1.5-fold odds of longer hospital stays with dementia.
Dementia and Health Conditions Associated with Admission Status Among COVID-19 Infected LTCF Patients in Texas Between January 2020 and October 2022.

Note. OR = odds ratio; 95%CI = ninety-five percent confidence interval; 1Adjusted for Medicare HMO and African American; 2Mutually adjusted for all variables together in this table; bold *p < .05.
Dementia and Health Conditions Associated with Longer Hospital Stays Among COVID-19 Infected LTCF Patients in Texas Between January 2020 and October 2022.

Note. OR = odds ratio; 95% CI = ninety-five percent confidence interval; aAdjusted for Age and Malnutrition; bMutually adjusted for all variables together in this table; bold *p < 0.05.
Discussion
Our findings indicate that dementia diagnosis predicts COVID-19 emergency admissions and shorter hospital stays among LTCF residents. This shorter length of hospitalization stay was particularly true for those with comorbid conditions, and being a racial minority.
Hospitalization Outcomes
Our findings of higher COVID-19 emergency admission with dementia and COVID 19 infection are consistent with previous studies from the earlier years of the pandemic (Al-Buthabhak et al., 2021; Emmerton et al., 2020). LTCF residents with dementia and a greater prevalence of comorbidities are more vulnerable to acute illness, leading to increased likelihood of using emergency admission, particularly in the context of COVID-19, a community spread infection. Moreover, caregivers in LTHFs reported difficulties in recognizing the severity of COVID-19 symptoms in residents with dementia, which could result in delayed diagnosis and subsequent emergency admissions (Emmerton & Abdelhafiz, 2021).
COVID-19 hospitalization was shorter for LTCF residents with dementia compared to others without a dementia diagnosis. Typically, older adult patients would have longer hospital stays due to underlying health conditions associated with the aging process (Hariyanto et al., 2021; Kim et al., 2022). The shorter hospital stays observed in our study could be linked to hospital staff unprepared to manage dementia patients presenting with COVID-19-infections. This would have been particularly the case during the early stages of pandemic (Mohammadzadeh et al., 2022). Hospital staff would likely regard LTCF better suited to service this vulnerable population, and particularly concerned about the higher risk for fall injuries with dementia from the fact dementia patients have higher movement disorders (Park et al., 2020). We also hypothesize that the shorter hospital stays could also be associated with communication impairments of dementia patients to be less able to express their care needs to hospital staff less familiar with them as individuals.
Pre-existing Health Conditions
The presence of pre-existing comorbidities increases the likelihood of COVID-19 emergency admission. In our dataset, having type 2 diabetes was found to increase the likelihood of COVID-19 emergency admission. Type 2 diabetes is associated with adverse outcomes with COVID-19 (Bonanad et al., 2020; Harb et al., 2021; Roig-Marin & Roig-Rico, 2022). Cardiovascular disease, obesity, chronic kidney disease and neurological conditions were associated with an increased risk of emergency admission among LTCF COVID-19 patients (Bashir et al., 2023). Potential explanations for this increased risk may include the direct impact of the COVID-19 virus on the heart, potentially leading to heart failure and necessitating emergency care, and regular medical interventions like dialysis, as well as worsened respiratory complications resulting from impaired kidney function. Thus, preexisting conditions would increase risk for emergency hospitalization with COVID 19 infections, while care staff unpreparedness would contribute to premature discharge, risking adverse health outcomes.
Sociodemographics
Being a racial minority was associated with an increased risk of emergency admission among LTCF COVID-19 patients. Our findings are consistent with a previous study, which observed a comparable 1.5-fold risk, albeit in different settings (Chang et al., 2022). The increased risk may be attributed to factors such as lower income, restricted healthcare accessibility, and higher prevalence of underlying health conditions in LTCFs. Lack of health care coverage would increase reliance on emergency care admissions and also shorter hospital stays (Udoh et al., 2023).
Lifestyle Factors
In this study, malnutrition was found to be a factor associated with longer hospital stays. This finding is consistent with similar studies (Nigatu et al., 2021; Vong et al., 2022). It is reported that malnutrition has been frequently associated with a weakened immune system, increasing vulnerability to the risk of severe COVID-19 infection (Vong et al., 2022). Heavy smoking and heavy alcohol consumption did not show such an association. Dementia patients in LTCF may be at lower risk for heavy smoking and heavy alcohol consumption as smoking and alcohol are routinely managed in LTCFs.
Implications for Practice
COVID-19 hospitalization care outcomes for dementia patients are best with person-centered strategies. In that regard, LTCFs resident care plans residents with should minimize the risk for excess COVID 19 hospital emergency admission of residents with dementia and risk for readmission for unmet needs associated with pre-existing health conditions. With the COVID-19 vaccination roll-out, shorter hospital stays are the norm for the general population for earlier remission of symptoms. However, for LTCF residents with dementia, their shorter hospital stay would be for other than remission of COVID 19 symptoms only, such as from their needs for intensive behavioral management care units may consider to exceed their capacity. Care units may also consider shorter stay for older adults with dementia as preventive of legal liability from injuries to or on patients they are less well prepared to manage.
LTCF should provide patient-centered care to dementia patients, who face a higher risk for adverse COVID-19 hospitalization outcomes. Such practices could include prioritizing universal COVID-19 vaccination interventions within LTCFs for mitigating the severity of COVID-19, reducing need for emergency hospitalization and/or unwanted hospital stays. Moreover, ongoing emergency hospital staff training managing COVID-19 patients with dementia would go a long way improving the care outcomes for this vulnerable population. For instance, a hospital discharge plan co-managed by the hospital and LTFC nursing staff would reduce the likelihood of rapid re-admissions from unresolved care needs for improved health care of the LTCF residents with dementia.
Strengths, Limitations, and Future Directions
For a major strength, our study utilized a large data public health dataset allowing us to analyze the data by pre-existing medical conditions, demographics, and health insurance, in order to understand risk factors associated with COVID-19 emergency admission and longer hospital stays among LTCF residents with and without a dementia diagnosis. The large sample size and our use of case control sampling added power to our study to detect group differences by the variables of study.
However, of the study limitations include the absence of available data concerning the severity of COVID-19 infection, COVID-19 vaccination status and stages of dementia. Future studies should include these factors for a better understanding of the COVID-19 hospitalization correlates for LTFC residents with dementia. In addition, age was found to be a confounding variable among dementia patients with severe COVID-19 infections, suggesting a need for future studies to stratify groups based on age cohorts (Tahira et al., 2021).
Conclusion
Our findings indicate a higher COVID-19 emergency hospitalization likelihood for LTCFs residents with dementia and also shorter hospital stay than would be expected by their having pre-existing conditions, associated with higher symptom severity. In particular, LTCF dementia patients with type 2 diabetes, cardiovascular disease, chronic kidney disease, and neurological disorders are associated with more COVID 19 emergency admission. In addition, LTCF dementia residents with malnutrition and obesity were likely with longer hospital stays. Being on Medicare health insurance (a US health insurance program for older adults 65 years and older), and being a racial minority is associated with a higher likelihood for emergency hospitalization and shorter length of stay in hospital. These findings suggest the need for targeted interventions to address COVID-19 hospitalization disparities, particularly among LTCF residents with dementia with significant health comorbidities.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
This study utilized de-identified public use data and did not require Institutional Review Board (IRB) approval.
HIPAA Identifiers
The authors certify that they have complied with the Health Insurance Portability and Accountability Act (HIPPA) in the conduct of this study. All data used in the study were obtained from the Texas Inpatient Public Use Data File (PUDF) and already de-identified. Since a public data set, no patient consent was required.