
Abstract
Accurate measurement of vital signs are important at skilled nursing facilities (SNF). Recent technological advancements now enable automated vital sign measurements. This overcomes the limitations of traditional manual vital sign measurement, which is time-consuming and error-prone. We present a novel case where continuous vital sign measurement was used to detect meaningful vital sign changes that led to early detection of a COVID-19 outbreak at a SNF. Residents were continuously monitored for changes to baseline respiratory rate and heart rate and with a Probability of Change (POC). Variations in baseline respiratory rate and heart rate occurred in 66% and 42%, respectively, of COVID-19 positive individuals; 83% of participants had statistically significant variations in either vital sign. Clinical investigations are typically triggered by vital signs outside normal ranges. We present a novel methodology to detect subtle vital sign changes that can lead to earlier diagnosis, treatment, and recovery from infections, like COVID-19.
What This Paper Adds:
Presents alternative method to prevent clinical deterioration at SNFs.
Addresses COVID-19 challenges at SNFs.
Applications of Study Findings:
Geriatric residents on telemetry.
Addresses utility and economics of telehealth.
Introduction
Skilled nursing facilities (SNF) are integral to U.S. healthcare. There are 1.6M Americans residing in US nursing homes, with that number expected to double by 2030 (Katz et al., 2009). Furthermore, SNF residents require complex medical care; the average resident has multiple comorbid conditions and takes seven-to-eight medications daily (Tjia et al., 2010).
Despite the growing demand for nursing home care, significant challenges persist. Prior to COVID-19, nursing staff was the single largest cost center for operating a nursing home (Xu et al., 2020). Post COVID-19, staffing challenges have been exacerbated. The American Health Care Association reported in 2021 that the nursing home sector lost 221,000 jobs (14% of its total workforce) (Gasdaska et al., 2022). Another study reported that over 60% of nursing homes have limited new admissions due to staffing shortages, with even more facilities concerned about closing their facilities in the future (ACHA, 2022).
Given these constraints, early detection of health-related issues has become difficult at SNFs. Firstly, measuring vital signs consumes resources. It takes 5 min, on average, to measure and chart one resident’s vital signs (Dall’Ora et al., 2021). This can consume several hours, daily, at SNFs. Secondly, both measurement and documentation of vital signs are prone to error. For example, respiratory rate is the most early and sensitive predictor of patient deterioration (Churpek et al., 2016) yet has been plagued by estimation, errors, or omissions altogether (Cretikos et al., 2008; Mok et al., 2015). Thirdly, certain physiologic and pathologic changes occur with aging that make vital signs less sensitive in detecting disease processes in older adults. Instead, newer research shows that changes to an individual’s baseline vital signs can more accurately detect early signs of clinical deterioration (Brekke et al., 2019).
Monitoring and evaluating vital signs can enhance the quality of care in this environment, and recent advances in wireless sensing technology can mitigate some of the listed challenges (Paterniani et al., 2023). FDA-cleared sensing technologies that continuously measure vital signs remotely can allow for automated vital sign measurements that are more accurate and with iterative outcomes.
To realize the value of continuous and accurate vital sign measurements, this retrospective study reports on the use of a novel methodology to measure subtle changes to vital signs for a group of residents at a skilled nursing facility that resulted in the early detection of several cases of COVID-19 during an outbreak at that facility. The background, methodology, and analysis are described herein.
Methods
Approximately one-quarter of residents from one unit of a 94-bed long-term and skilled living facility in a metropolitan area of the midwestern United States received continuous vital signs monitoring using the Xandar Kardian XK300 vital signs monitor. The XK300 is an FDA-cleared, class II medical device that continuously measures resting heart rate (HR) and respiratory rate (RR) using IR-UWB radar. The monitoring device is supported by software that visualizes resting heart and respiratory rates to enable both real time and trend-based review by clinicians.
In early October 2022, a subtle shift in the baseline heart and respiratory rates of Patient A was detected by the sensor. As shown in Figures 1 and 2, the patient’s vital signs had increased above her baseline (as noted by the red line). While notably different from her measured baseline over weeks prior, her heart rate remained within generally accepted “normal” limits, and respiratory rates appeared only slightly elevated over her typically elevated baseline. The patient’s head-to-toe physical exam was unremarkable, and the patient was noted to be asymptomatic. The following day, facility staff were notified by the patient’s family that she had been exposed to COVID-19, and a subsequent PCR test that day found her positive for COVID-19. The patient later developed symptoms of body aches, a low-grade fever, cough, and runny nose.
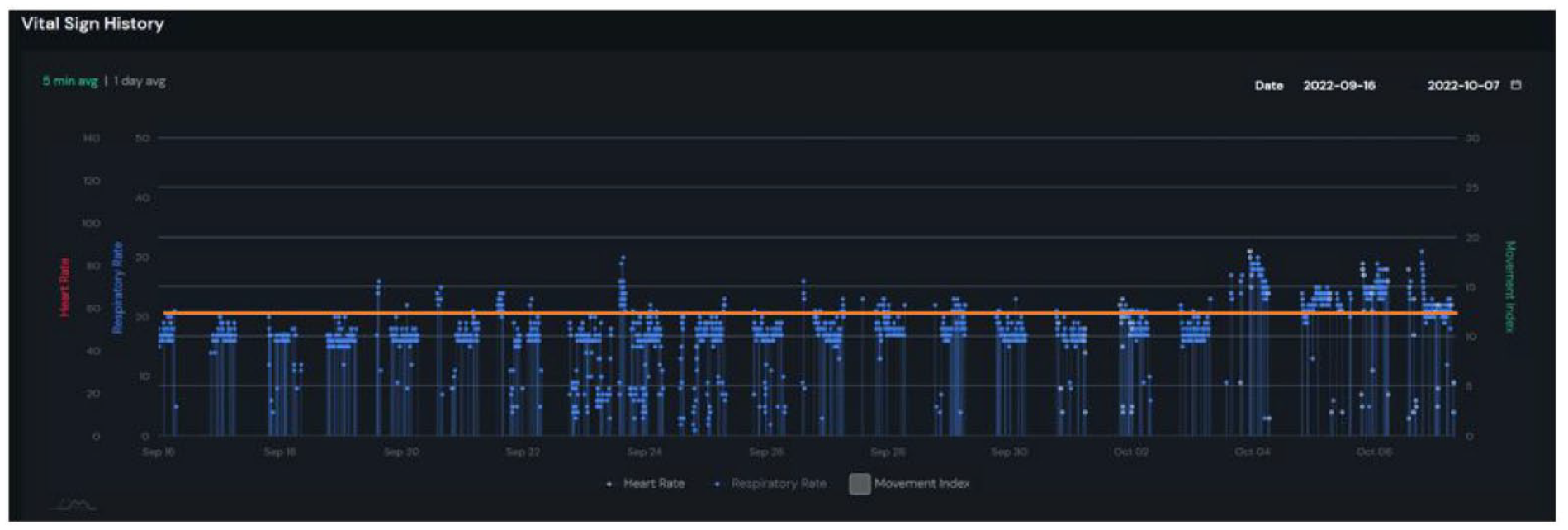
Five-minute averages of respiratory rates collected by the sensor.

Five-minute averages of heart rates collected by the sensor.
Following this initial diagnosis, similar trends in rising baseline vital signs were detected among the other monitored patients. To proactively detect these subtle changes in baseline vital signs, the authors of this manuscript developed the Probability of Change in Condition (POC) Score. The POC Score quantifies the rarity of recently measured heart and respiratory rates to identify subtle but statistically significant changes to a patient’s baseline vital signs, relative to their vital signs over previous days. The POC score is calculated based on statistical modeling of vital signs and rarity analysis of the series of HR and RR within a window of time.
Analysis of Patient A’s shifted vital signs revealed a POC score of 99% for both HR and RR, suggesting a 99% chance that the measured vital signs were different from her normal rates over the previous week.
COVID-19 cases subsequently spread throughout the facility, resulting in a total of 52 of the 72 (72%) residents testing positive over an 18-day period. Of all cases, 35% (18 residents) were on the first floor and 65% (34 residents) were on the second floor, as shown in Figure 3.

New COVID-19 cases by date and location.
Results
Fourteen residents on the second floor were selected as a convenience sample for continuous vital signs monitoring in this study. Of these residents, 13 (6 women and 7 men; average age 79.3 years) tested positive for COVID-19. Data from 12 geriatric patients was included in this retrospective review; data was excluded for one resident who spent limited time in the sensor range and therefore had an insufficient number of vital signs measurements. Data included in the study was collected from a central, online, data repository.
The POC scores for HR and RR of monitored patients were reviewed for the 2 days prior to their COVID-19 diagnosis. “Diagnosis” is defined as the day the patient tested positive for COVID-19 via nasal swab. The results are summarized in Table 1 below.
POC Scores Relative to Day of COVID Diagnosis.


Yellow corresponds to POC score of 80% or above. red corresponds to POC score of 90 or above.
As shown in the table above:
10 of 12 (83.3%) showed a POC score >80 in either HR or RR prior to COVID diagnosis. These are highlighted in yellow and red above.
Fewer patients (only 5 of 12 residents, 41.67%) had vital signs changes that triggered a POC over 90 in one of either HR or RR. These are highlighted in red.
Changes in POC for RR were more common than changes in POC for HR for acute COVID infection; 7 of 12 patients did not have significant variations in HR whereas 4 of 12 patients (33%) did not show significant RR variations prior to COVID diagnosis.
Discussion
This report examines a potential correlation between a novel marker of vital sign variability and a COVID-19 infection. Heart rate and respiratory rate variations were evaluated using POC score as a potential early marker of infection. In this study, 66% of residents had RR variations; whereas 42% had HR variations. Combined, 83% of residents had HR or RR variations (reflected as POC scores over 80), prior to a COVID diagnosis. There are several potential reasons for the lower correlation of HR; one, SNF residents have multiple comorbidities and/or medications that can dampen a normal cardiovascular response; and two, HR variation reflects a marked inflammatory response (i.e., a sicker patient) which may occur later as COVID-19 progresses.
Conclusion
Careful observation and systematic evaluation of vital signs are essential in the post-pandemic era. Nursing home residents are vulnerable to COVID-19 due to their age, functional impairments, comorbidities, and congregate living status. When detected early, within the first 5 days of symptom onset, the CDC recommends COVID-19 treatments, such as Paxlovid, which improves clinical outcomes.
The current practice for investigating changes in condition is often triggered when vital signs measurements exceed historically acceptable “normal ranges.” However, it is widely recognized that normal vital signs vary, particularly among patients with chronic conditions and among the geriatric population who reside at SNFs. Relying only on spot checks and vital signs changes that are outside normal ranges may result in both false positives (i.e., escalations for patients with normally high or low heart or respiratory rates) and false negatives (missing subtle changes and failing to escalate when patient vital signs do not exceed thresholds). The POC score uses statistical analysis to detect individualized changes to vital signs relative to his or her historical distribution, regardless of normal thresholds. This represents a novel and more individualized approach to detecting early clinical changes that may be missed by the current standard of care. As such, the POC score may facilitate earlier clinical intervention, faster patient recovery, reduced rehospitalizations and better clinical outcomes for patients, facilities, and healthcare systems.
Additionally, there are economic benefits that stem from this early detection protocol. For the purposes of the study, the cost to administer the sensors was nominal and covered by remote patient monitoring (RPM) CPT bill codes. However, the monitoring protocol aims to detect COVID-19 early to prevent hospital readmissions, which typically cost over $10,000 USD per hospital admission. Additionally, by performing continuous vital sign checks, this methodology saves on clinical human resource costs, which have ballooned in the post-COVID era. Staff COVID exposures can also be reduced, leading to fewer sick days and further savings.
In summary, we present a retrospective study where changes to residents’ baseline vital signs were examined to more rapidly detect a COVID-19 outbreak at a SNF. There was a high correlation: 83% of COVID-19 positive residents who were studied showed meaningful changes to heart rate or respiratory rate, reflected by a POC score over 80%.
RPM has the potential to improve clinical outcomes, patient engagement, and access to healthcare, particularly for immobile, older adults. However, ethical considerations remain. It is vital to ensure equitable access to new RPM technologies, regardless of socioeconomic status, to avoid exacerbating health disparities. Additionally, any patient monitoring technology must balance patients’ need for autonomy and health privacy against the benefits of continuous monitoring.
This review is limited in that a positive COVID-19 diagnosis was used to trigger a lookback period where POC changes could be evaluated. Testing protocols are regulated and stringent in this setting. Thus, testing and diagnosis beyond the first positive case is not due to the presence or onset of symptoms. Instead, the first positive case triggered facility-wide testing of all patients on days 1, 3, 5, 7, and 9, with the regimen beginning again for well residents with each new positive case. An evaluation of POC scores relative to the date of first symptom onset may yield interesting results; as in patient number 1, the positive test came prior to symptom onset by over 24 hr. For maximum utility in detecting COVID-19 early, it would be most helpful to identify patients while they are asymptomatic to reduce the risk of spread.
For the future, the authors recommend a rigorous study be carried out to identify thresholds and characterize the sensitivity and specificity of the POC score in infections, like COVID-19, using the POC techniques described herein. Additionally, the study can be extended to a broader array of disease states, infections, and medical conditions.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Linda Mayhue, Jeong Woo (Glen) Choi, Sun Jong (Sam) Yang, and Yuna Lee are employed by Xandar Kardian Corporation. Salim Ahmed is a consultant to Xandar Kardian Corporation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Participant Consent and IRB Approval
We declare that this submission is exempt from ethics and IRB approval per United States regulation 45 CFR 46. The research meets one of its criteria: “the identity of human ’subjects’ cannot be readily ascertained.” This is because the only patient data in our manuscript is vital sign statistical data (heart rate and respiratory rate only) that cannot readily identify an individual. No other identifying patient information was included in this study. Nor does the reporting of participant data infringe on any rights of participants. As such, informed consent, IRB approval, and ethics approval was deemed unnecessary.