
Abstract
Keywords
Key Statements
What is Already Known About the Topic
Tube feeding increases incidence of pneumonia and mortality in persons with advanced dementia.
Psychosocial health is impacted by the lack of socialization that can occur as a result of tube versus oral feeding.
Tube feeding is commonly recommended amid dysphagia and critical illness.
What This Paper Adds
This research provides essential data on patient outcomes (pneumonia, depression, mortality) as related to feeding route amid dysphagia and end-stage stroke or chronic obstructive pulmonary disease (COPD).
No prior research has measured these outcomes, comparing the treatment effect of tube versus oral feeding in persons diagnosed with life-limiting illness.
Implications for Practice, Theory, or Policy
This research will help guide health care providers regarding selection of the best feeding route for persons diagnosed with dysphagia and stroke or COPD at the end of life.
This research may help to shift nutritional decision-making paradigms.
Introduction
Health care providers may use equipment and invasive procedures amid critical illness to “prevent harm.” This can result in overmedicalization of patients and misalignment with biomedical ethics (Shippee et al., 2018). Tube feeding is defined as provision of liquid nutrition via a tube: (a) placed into the stomach via percutaneous endoscopy or surgical insertion, (b) surgically placed through the skin of the abdomen into the midsection of the small intestine, or (c) inserted through the nose to the stomach (Doley, 2022). Tube feeding is often recommended when a patient demonstrates difficulty swallowing and health care providers fear aspiration (i.e., entrance of foreign material and associated oral pathogens into the airway).
Past research reports complications of oral feeding with dysphagia (difficulty swallowing) including consequences of aspiration, such as pulmonary decompensation related to pneumonia (Thiyagalingam et al., 2021; Wilkinson et al., 2021). Past studies have also revealed risk of harm from tube feeding in patients with life-limiting illness, including increased rates of pneumonia, depression, and mortality (Gillick, 2000; Hanners Gutierrez, 2019; Newman et al., 2020). Use of tube feeding often continues at the end of life as a replacement for eating and drinking by mouth (Lee et al., 2021; Winter, 2000).
Careful hand oral feeding (vs. tube feeding) is an evidence-based and recommended strategy to provide comfort and nutrition (De, 2019; World Health Organization, 2022; Yuen et al., 2023). Health care providers need to discern the potential impact of the chosen feeding route when combined with each patient’s polymorbidity and palliative medicine standards of practice. Palliative care providers should not solely focus on meeting patients’ physical and disease management needs. Standards of care in palliative medicine include psychological support (Ferrell et al., 2018). Tube feeding has been shown to negatively affect one’s psychosocial health (Cardenas, 2021; Pizzorni, 2019).
There is a critical need for research regarding the best option for a feeding route amid life-limiting illness and dysphagia. The aim of this research study was to contribute to clinical nutritional paradigms in palliative medicine through provision of relevant data. The researchers examined patients with end-stage stroke and end-stage chronic obstructive pulmonary disease (COPD), and outcomes related to pneumonia, depression, and mortality were measured.
Ferrell et al. (2018) developed domains of palliative medicine as part of the National Consensus Project for Quality Palliative Care. The goal of palliative medicine as defined by the World Health Organization is reduction of suffering (World Health Organization, 2022). Suffering can be reduced through a focus on psychological, spiritual, and cultural values that shift the lens through which providers view overall health care (Radbruch et al., 2020). Principles of biomedical ethics (Varkey, 2021) underpin health care decision making, including the use of non-oral nutrition and hydration. Patient autonomy warrants unbiased, well-grounded education so that the patient can make an informed, autonomous, least-risk choice. Beneficence and non-maleficence are enacted when the long-term implications of the feeding route are considered versus the potential immediate result or expected benefit. Justice is supported when health care providers make fair and equitable decisions between patients. For example, patients who require careful hand feeding and have little family support should be assisted versus receiving tube feeding as a perceived easier-to-manage nutritional option (Di Muzio et al., 2018).
Outcome measures (pneumonia, depression, mortality) for this research study were selected due to the association of each with dysphagia (inclusion criterion) which can lead to challenges with nutritional decision-making. Patients may be denied their requests for oral nutrition due to dysphagia and providers’ feared consequences of aspiration, such as pneumonia and mortality. Moreover, the withholding of oral nutrition (replaced by tube feeding) can have negative psychosocial (Pizzorni, 2019) and physiological (Vellani, 2019) effects. It was important to explore the relationship of pneumonia, depression, and mortality to feeding route, because each outcome measure should be considered when prescribing nutritional support.
Karisik et al. (2024) reported an association between depression and dysphagia following ischemic stroke as indicated by participant scores on the Beck Depression Inventory and Hospital Anxiety and Depression Scale. Patients who are tube-fed and subsequently isolated from socialization or the comfort of eating by mouth may also experience depression (Hepper et al., 2024; Umrania et al., 2021). Pneumonia has been found to have a significant relationship to dysphagia and aspiration. Any pneumonia type (health care-acquired, community-acquired, or aspiration) can be caused by pulmonary ingestion of infectious properties (e.g., oropharyngeal pathogens transported to the lungs by food or drink) (DiBardino & Wunderink, 2015; Mandell & Niederman, 2019). Lastly, dysphagia increases risk of aspiration, which can negatively impact morbidity and mortality (Thiyagalingam et al., 2021).
Dysphagia is commonly present in patients diagnosed with stroke or COPD. Chacko et al. (2021) identified dysphagia following stroke in 53% of patients admitted to a tertiary care center. Clayton et al. (2014) reported reduced laryngopharyngeal mechanosensitivity in patients diagnosed with COPD. When patients with stroke or COPD worsen beyond recovery, nutritional decision-making becomes more complex. Tube feeding is often considered and perceived to be an appropriate intervention for suboptimal swallow biomechanics related to stroke (D’Netto et al., 2023; Food Trial Collaboration, 2005) and COPD (De Schreye et al., 2018; O’Rourke et al., 2014).
Tube feeding has a negative impact on patient outcomes as related to pneumonia, depression, and mortality (Clarke et al., 2017; Hanners Gutierrez, 2019; Lin et al., 2020). A review by Elmahdi et al. (2023) reported high prevalence of aspiration pneumonia and mortality in patients who were tube-fed, citing dysphagia as a risk factor. A prospective observational study by Cintra et al. (2014) yielded increased aspiration pneumonia and mortality in patients with advanced dementia who received tube feeding. Tube feeding has also been found to increase the likelihood of depression and infection in adult patients with varied diagnoses in both restorative and palliative care contexts (Clarke et al., 2017). While tube feeding may be beneficial to combat effects of early sepsis (Compher et al., 2017; Elke et al., 2014) and amid traumatic brain injury (Horn et al., 2015; Kurtz & Rocha, 2020), evidence does not support its routine use with patients at the end of life with dementia, stroke, or COPD (Khoury et al., 2015; Souza et al., 2020; Vignari, 2020).
Nutrition is an essential part of each patient’s health care story. Health care providers and caregivers are challenged to make the “right” decision in the context of patients’ health care complications and emotions (Druml et al., 2016). Prior to decline to fasting and active death, palliative care patients often still want to eat and drink. Oral feeding (self-served) or assisted feeding/careful hand oral feeding (Yuen et al., 2023) are alternatives to tube feeding that offer a slow pace, the ability to stop if dysphagia symptoms arise, and control of the volume delivered per bite/sip. This study was conducted to help determine the best feeding route when a patient wishes to eat by mouth and health care providers feel reluctant to permit this.
The researchers aimed to determine outcomes (pneumonia, depression, mortality), as related to feeding route (oral or tube), of patients with dysphagia who were receiving palliative care post stroke or with COPD. The results of this study will contribute to the palliative medicine nutritional decision-making paradigm.
Methods
Participants
Participants were patients admitted to a hospital tertiary care center and treated by palliative medicine between January 1, 2014 and September 30, 2017. Data on patient outcomes (pneumonia, depression, mortality) and feeding route (oral or tube) were collected. The method of sampling involved retrospective, archival data analysis. Given the absence of prior studies with comparable methodologies, determining a specific sample size a priori was challenging. Instead, we aimed to collect data over a 45-month period to ensure an adequate sample size for statistical analysis. This approach produced a dataset with sufficient variability and enabled us to match participants effectively. No participant consent was required. The Institutional Review Board mandated ethical rigor. All data were deidentified by the hospital’s Information Technology (IT) Department prior to provision to the first author.
Researchers conducted electronic chart queries as follows: (a) diagnoses (stroke or COPD), dysphagia and outcome measures by International Classification of Diseases (ICD)-9 or ICD-10 coding and hospital mortality database, (b) mortality risk and severity of illness by disease-specific algorithm, (c) age, and (d) sex. The first author manually inspected charts to determine feeding route (route of longest duration) and to confirm presence/absence of dysphagia. Dysphagia was determined by clinical or instrumental examination and coded (ICD-9 or ICD-10) or included in health care providers’ medical notes. From 2,180 records, charts of 541 patients met the inclusion criteria. Inclusion criteria were defined a priori as follows: (a) all adult ages (i.e., 18 years of age and older), (b) diagnosis (i.e., COPD, stroke), (c) presence of dysphagia, (d) informed, autonomous choice of nutritional provision (patient or medical power of attorney), and (e) admission to a tertiary care center and treatment by the palliative medicine service. Patients for whom there was no measurable feeding route (oral or tube) due to death upon hospital admission or shortly thereafter were excluded. Participants who did not desire nutritional support were also excluded.
Participants who were admitted under observation but considered outpatient status were removed. In addition, duplicate visits (i.e., more than one hospital admission) were removed. This yielded 287 participants with five participants added (N = 292) when the Institutional Review Board (IRB) permitted inclusion of participants over 89 years of age after initially excluding them due to concerns about patient confidentiality (i.e., perceived ease of identifying elder patients). Propensity score analysis was used, and 188 participants matched (i.e., 94 per treatment and comparison groups). The age range of matched participants was 29 to 93 years. Intra-judge reliability by the first author was determined using intraclass correlation coefficient (Koo & Li, 2016).
Design
This study involved a retrospective analysis of existing patient medical records. Dependent variables were pneumonia, depression, and mortality. The independent variable was feeding route. Pneumonia and depression were identified from the ICD diagnostic codes and were defined as existing or absent. Mortality was defined as expiration or discharge to hospice (imminent death within 6 months). The independent variable (feeding route) was defined as follows: (a) tube feeding, provided by nasogastric (NG) tube, gastrostomy (G) tube, or jejunostomy (J) tube, and (b) oral feeding, delivered by mouth. The study was conducted to determine possible associations between patient outcomes and feeding route with covariates isolated from the treatment effect.
Covariates were age, sex, diagnosis (stroke or COPD), mortality risk, and severity of illness. Mortality risk and severity of illness scores were obtained from an algorithm yielding a number that corresponded to proximity to death or extent of physiological compromise. According to the Methodology Overview of the 3MTM All Patient Refined Diagnosis Related Groups (APR DRG) (2023), risk of mortality is defined as “the likelihood of dying” (p. 8). Severity of illness is defined as “the extent of physiologic decompensation or organ system loss of function” (p. 8). Mortality risk and severity of illness scores are the result of a complex analysis of health care complications and comorbidities (Centers for Medicare and Medicaid Services, 2024) and have been determined to be the most accurate comorbidity indices (Santos et al., 2022). Stroke or COPD were identified from the ICD diagnostic codes and were viewed dichotomously. Sex was dichotomous and defined as biological identity. Age was defined as years of living.
Statistical Analysis
The primary aim was to determine which feeding route was more likely to be associated with pneumonia, depression, or mortality in patients receiving palliative care, diagnosed with dysphagia, and receiving nutritional provision by choice, with the independent variable (i.e., feeding route) being isolated from potential moderating effects of covariates. A secondary goal of this study was to impact nutritional decision-making by health care providers for patients receiving palliative care with stroke or COPD.
Propensity score matching was used to approximate a gold standard study, randomizing participants by algorithm (i.e., by the statistical program itself) and matching them on pre-treatment variables for a controlled study design. A propensity score matching protocol by Thoemmes (2012) was completed. Propensity scores were created using logistic regression. A two-step process was used to accomplish statistical analysis, and participants with missing data were excluded.
Stage 1 involved analyzing the relationship of the covariates to the independent variable. The independent variable for the outcome model (feeding route) was the dependent variable in the treatment model (Stage 1). This important first step was completed to reveal any statistically significant confounding or moderating effects of alternative factors on the dependent variables in the outcome model (Stage 2). Participants were matched with nearest-neighbor matching with a caliper of 0.1; the caliper is the maximum allowable distance between two matched participants (Thoemmes, 2012). No participant was used more than once. Group balance was assessed with an independent t-test and Levene’s Test for Equality of Variances to ensure treatment model adequacy. Chi Square tests were run on the balanced groups (matched participants) to examine frequency counts and relationships between feeding route (oral or tube) and outcome measures (pneumonia, depression, mortality) prior to implementing propensity score matching, Stage 2. Frequency counts offered preliminary information about the treatment effect before final regression analyses.
Stage 2 used binary logistic regression to determine odds ratios and predict relationships between the outcome model independent variable (feeding route) adjusted by covariates (age, sex, diagnosis [stroke or COPD], mortality risk, and severity of illness) and dependent variables (pneumonia, depression, mortality). The strongest independent predictors (oral-fed vs. tube-fed) of outcome measures were determined. Intra-rater reliability was determined using intraclass correlation coefficient (ICC); ICC estimates and their 95% confidence intervals were calculated based on an absolute-agreement, one-way, random effects model.
Results
Overall, results revealed strong associations with tube feeding and negative outcomes, and a greater probability that pneumonia, depression, and mortality may occur with tube feeding versus oral feeding in persons with difficulty swallowing and end-stage stroke or end-stage COPD. Table 1 provides baseline characteristics of matched participants.
Feeding Route and Baseline Characteristics of Matched Participants.

Chi Square frequencies and robust classification percentages indicated tube feeding to be predictive of pneumonia, depression, and mortality. Logistic regression conducted amid propensity score matching revealed statistically significant results. Researchers defined statistical significance at the conventional alpha level of 0.05. The odds of pneumonia, depression, and mortality increased significantly with tube feeding, holding all other variables constant. Of note, results indicated pneumonia to be 10.14 times more likely to occur with tube feeding (vs. oral feeding). See Tables 2 and 3 for a summary of results for the all-matched participants outcome model. Intra-rater reliability was conducted using ICC which revealed a value of 1.0. Values greater than 0.9 reveal excellent reliability.
Relationship of Tube Feeding to Pneumonia, Depression, or Mortality in an All-Matched Participants Model (N = 188).

Note. OR = Odds Ratio; CI = Confidence Interval.
p = .01.
p < .01.
p < .001.
Relationship of Oral Feeding to Pneumonia, Depression, or Mortality in an All-Matched Participants Model (N = 188).
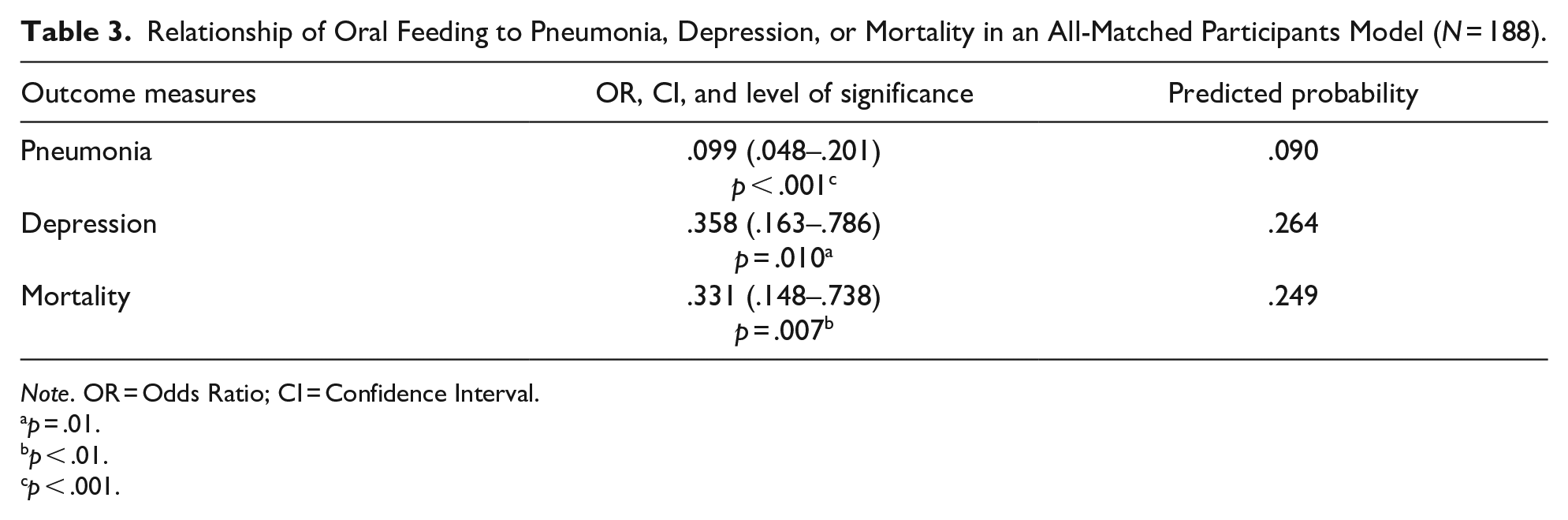
Note. OR = Odds Ratio; CI = Confidence Interval.
p = .01.
p < .01.
p < .001.
Stage 1 statistical analysis effectively isolated all covariates from the treatment effect. Diagnosis (COPD or stroke) was not found to have a statistically significant relationship to feeding route. Participants with the covariate COPD or the covariate stroke had equal propensity to be orally or tube fed. In addition, these diagnoses did not moderate the relationship between feeding route and patient outcomes.
Mortality risk was not found to have a statistically significant relationship to feeding route. Tube feeding was found to be used more often with sicker patients. The odds of a person being orally fed significantly decreased by .371 with incremental increase in severity of illness (p = .018). Further statistical analyses revealed neither the covariate mortality risk nor the covariate severity of illness moderated the relationship of feeding route to patient outcomes.
The relationships of covariates age and sex to the feeding route and patient outcomes were also analyzed. Sex was not found to have a statistically significant relationship with feeding route; however, the odds of oral feeding were significantly greater (OR = 1.032) with an incremental increase in age (p = .012). Further statistical analyses revealed age or sex did not moderate the relationship of the feeding route to patient outcomes.
Discussion
This study contributes to existing literature regarding relationships between oral versus tube feeding and pneumonia, depression, or mortality in patients receiving palliative care who had dysphagia and COPD or stroke. The critical finding was that patient outcomes worsened with tube versus oral feeding. This result was obtained using a controlled, matched sample randomized by algorithm, approximating a gold standard study. Pneumonia was 10.14 times greater in participants who were tube-fed. Results of this study should lend pause to the recommendation of tube feeding amid difficulty swallowing. Results of this study also showed that psychological suffering increased with use of tube feeding, yielding a 2.79 greater likelihood of depression in patients who were tube-fed. Results revealed that mortality was not reduced with tube feeding, but rather, increased by 3.02 times in a comparison to oral feeding.
Main Findings/Results of the Study
Results of this novel study align with past studies that have revealed tube feeding to increase risk of pneumonia and mortality. Sako et al. (2014) reported an in-hospital mortality rate of 11.9% amid patients who underwent gastrostomy or jejunostomy placement. Intracranial injury and chronic lung disease were independent risk factors for mortality. Langdon et al. (2009) prospectively observed infection rates in 330 patients post ischemic stroke as related to feeding route (oral or tube) and reported increased respiratory infections in participants who were restricted from oral intake and fed solely by tube. Cintra et al. (2014) reported increased incidence of pneumonia and mortality in persons with advanced dementia who received tube versus oral feeding. Research has revealed a lack of psychosocial support for the elderly, including spiritual support (Jadidi et al., 2021). Qualitative data reveal the benefit of improved attention to patients’ emotional needs as dependence for care increases. Careful hand oral feeding is a measure to improve a patient’s perception of emotional support.
Strengths and Limitations of the Study
Strengths of the study included a rigorous statistical analysis (propensity score matching) that supported a controlled, matched sample randomized by algorithm. Other researchers have used propensity score matching to pair participants and balance baseline covariates while analyzing archived data (e.g., Kim et al., 2024). This study included all adult ages. Participants had dysphagia, detected via clinical observation or bedside or instrumental examination, which distinguished this research from studies that have compared oral and tube nutrition without adjusting for swallow functionality. Participants were patients receiving palliative care, an important caveat, as nutritional decision-making is an essential component of end-of-life care (Eisenmann et al., 2020; Hamburg et al., 2014). Depression was included as an outcome measure, highlighting the importance of assessing psychosocial health amid life-limiting illness.
There were limitations of the study. The study was conducted retrospectively; therefore, pre-treatment characteristics (e.g., oral hygiene) could not be controlled. The first author was also responsible for conducting manual internal chart audits to determine the primary feeding route and to verify presence of dysphagia. Non-automated chart auditing may involve inadvertent human error. Feeding route and daily patient care documentation were clear in the electronic medical record (EMR). However, at times tube feeding may have been paused (e.g., turned off while moving a patient) or a patient may have declined careful hand oral feeding. Brief cessation of feeding is not required in EMR documentation, per hospital policy. The authors do not suspect that infrequent occurrences as described would have invalidated results due to the robust levels of significance that were achieved.
Clinical Implications and Future Research
The findings of this study have several clinical implications, as listed below.
Nutritional decision-making should include consideration of oral nutrition at the end of life.
Health care providers should weigh the decision to replace oral nutrition with tube feeding in the context of dysphagia, particularly regarding the risk of pneumonia.
Patients’ expressed desires to have favorite foods or drinks amid life-limiting illness should be supported by health care providers.
Careful hand oral feeding should be implemented amid life-limiting illness with patients who cannot self-serve oral nutrition but still desire to eat/drink.
Patients’ psychological health and connection to caregivers may be strengthened by increased support for oral feeding at the end of life.
Future research offers opportunities to investigate patient-rated quality of life in patients with dysphagia receiving palliative care and oral or enteral nutrition. In addition, patient outcomes of persons with alternative diagnoses can be investigated with potential moderators controlled (oral hygiene, patient positioning, duration, or refusal/cessation of feeding).
Conclusion
Results of this study reveal that oral nutrition has a stronger relationship to better outcomes than tube-fed nutrition in patients with dysphagia and end-stage COPD or end-stage stroke. Use of feeding tubes in these populations (and others) should be reviewed carefully given evidence that they do limited good and are associated with greater burdens across a range of domains of patient experience. Results should shift the health care lens to one that views oral feeding as possible and evidence-based for terminally-ill patients requesting to eat by mouth. The researchers are not suggesting that tube feeding be omitted as an option but rather that health care providers cease defaulting to tube feeding amid dysphagia for safety or comfort because evidence does not support this. When a patient is not responsive, not eating, and has entered active death, nutrition is not the priority. Prior to this state, however, patients may still seek nutrition. Food and drinks offered by mouth when desired by patients can better meet standards of care in palliative medicine. This study is a step toward supporting this practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Research materials can be requested from the primary author who will follow institutional policies and regulations related to the handling and sharing of sensitive information.