
Abstract
Keywords
Introduction
Eye Care Services in Post-Acute and Long-Term Care Facilities
Post-acute and long-term care services in the US serve a population of 9.5 million in different types of settings, including community (e.g., adult day services centers), home (e.g., home health agencies), institutions (e.g., nursing homes), and other residential settings (e.g., assisted living) (Sengupta et al., 2022). Provided services vary greatly based on the care organization type. Assisted living residents can reside independently. However, shared spaces offer general living-related possibilities and services. In contrast, nursing homes provide 24-hour care. Roughly 9 of 10 nursing home residents need help with daily activities, such as eating and toileting. Nursing homes offer various healthcare services besides skilled nursing and therapeutic services, such as dementia services, podiatry services, and dental services. Some specialty healthcare services, such as eye care, are not mandated. (Harris-Kojetin et al., 2016; Sengupta et al., 2022.)
However, the US Centers for Disease Control and Prevention recognizes the importance of regular eye examinations, which can lead to earlier detection and treatment of vision-threatening eye diseases among at-risk patients. Known risk groups for vision impairment include the elderly population, diabetic patients, and patients with existing eye conditions. Improved access to general medical services is proposed as a good opportunity for earlier recognition of eye diseases, and this offers a vehicle for referral to eye care providers. Ocular screening of diabetic patients is proposed to decrease the rates of vision and other chronic disease-related disabilities linked with diabetes. As an example, timely treatment of sight-threatening diabetic retinopathy has been found to decrease vision loss more than tenfold. (Centers for Disease Control and Prevention, 2010.)
Undiagnosed Diabetes and Diabetic Retinopathy (DR)
In 2019, the US population aged 65 years or older was 54.1 million, and it is estimated to reach 80.8 million in 2040. The growing life expectancy creates a challenge for healthy aging. Aging is one of the major risk factors for chronic diseases, including diabetes. (Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, 2022.) Two-thirds of the US population aged 65 years or older have more than one chronic disease, diabetes being one of them. Diabetes is the sixth leading contributor to all deaths in the United States among the population aged 65 years or older. Two-thirds of the national healthcare budget is directed toward caring for these conditions. (Centers for Disease Control and Prevention, 2013.) The prevalence of diagnosed and undiagnosed diabetes in the US in 2019 was estimated to be 11.3%. The undiagnosed portion represented approximately one-fourth of the total percentage. The projections indicate an increasing prevalence of total, diagnosed, and undiagnosed diabetes in the United States (Centers for Disease Control and Prevention, Data and Statistics, 2022).
Diabetes can cause life-debilitating complications, including diabetic eye disease, considered one of the primary vision-threatening eye diseases (NORC, National Center for Chronic Disease Prevention and Health Promotion, 2018; Zhang et al., 2010). Seventeen major population-based studies estimated the prevalence of DR in the US among different subgroups of populations. Four of these studies were designed to evaluate the prevalence of systemic diabetes without restrictions to persons diagnosed with it (NORC, National Center for Chronic Disease Prevention and Health Promotion, 2018). The most recent study was conducted by Zhang et al. (2010), which analyzed data from the National Health and Nutrition Examination Survey from 2005 to 2008. They used fundus photography to assess the retina for retinal dot and blot hemorrhages as a clinical hallmark finding to diagnose DR. A previous diagnosis of diabetes or elevated hemoglobin A1C measurements were used to determine diagnosed and undiagnosed diabetes. The estimated overall prevalence rate of DR among the US population was predicted to be 3.8%. However, among diabetic patients, the prevalence of DR was found to be 32.9%, of which 4.4% was found to be sight threatening. Males had higher prevalence rates than women, and race-related risk factors included non-Hispanic black and Mexican American races. Longer duration of diabetes was also found to predict higher prevalence rates for DR, making older age a risk factor (Zhang et al., 2010).
Data indicates that vision loss and ocular diseases form one of the leading healthcare-related economic costs in the United States, and expenses are projected to grow due to the aging population. Evaluation of medical expenses per person reveals diagnosed blindness as the most expensive condition, followed by retinal disorders such as DR (Rein et al., 2022).
Pathophysiology of Microvascular Diabetic Disease
Increased blood sugar levels in diabetic patients can lead to highly destructive consequences, causing cardiovascular disease (macrovascular) and neuropathy, nephropathy, and retinopathy (microvascular). As a result, these can end in life-debilitating complications such as myocardial infarction, stroke, foot amputation, kidney failure, and blindness. Vision loss occurs concurrently with the development of nephropathy, peripheral neuropathy, and cardiovascular events. (Cole & Florez, 2020.)

Mechanisms of hyperglycemia-induced tissue modifications in microvascular diabetic disease.

Inflammation processes and affected ocular structures in diabetic retinopathy.
As the disease advances, retinal ischemia causes an increase in the expression of vascular endothelial growth factor (VEGF) by activating hypoxia-inducible factor 1 (HIF-1). VEGF is known to cause proliferation of endothelial cells through the activation of mitogen-activated protein (MAP). The expression of VEGF has been detected in the vitreous of patients with center-involved diabetic macular edema and PDR. Other angiogenic factors, such as angiopoietins (Ang-1, Ang-2), are also known to have a role in regulating vascular permeability by interplaying with endothelial receptor tyrosine kinase Tie2 (Ansari et al., 2022). In summary, functional changes in DR include vascular permeability, leukostasis, and reduction in vision.
Clinical Assessment and Management of Diabetic Retinopathy (DR)
DR is classified either as non-proliferative or proliferative. Findings of the non-proliferative form can include retinal microaneurysms (dot hemorrhages), retinal hemorrhages (blot hemorrhages), exudates, cotton wool spots, intraretinal microvascular anomalies (IRMA), or venous beadings (Yang et al., 2022) (Picture 1).

Non-proliferative diabetic retinopathy (dot and blot hemorrhages and hard exudates).
The proliferative form is more severe and brittle; pathological new vessels develop, leading to leakage, vitreous hemorrhage, and eventually fibrotic strands from the retina into the vitreous. Fibrotic strands can lead to tractional retinal detachment (Zetterberg, 2016) (Picture 2).
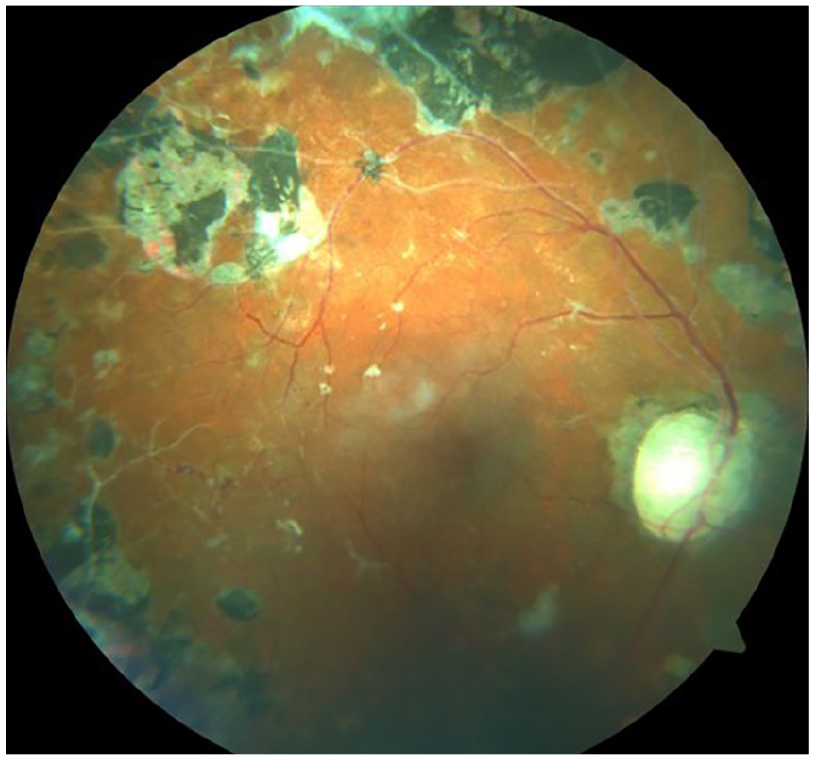
Advanced-stage diabetic eye disease (PDR with PRP).
Center-involved diabetic macular edema is a prevalent condition that leads to the most notable visual impairment in individuals with DR and can occur at any stage of the disease process (Tatsumi, 2023). Diabetic retinal changes can be observed during a comprehensive eye examination or using different types of imaging studies (Table 1).
Imaging Studies for Assessing Diabetic Patients.
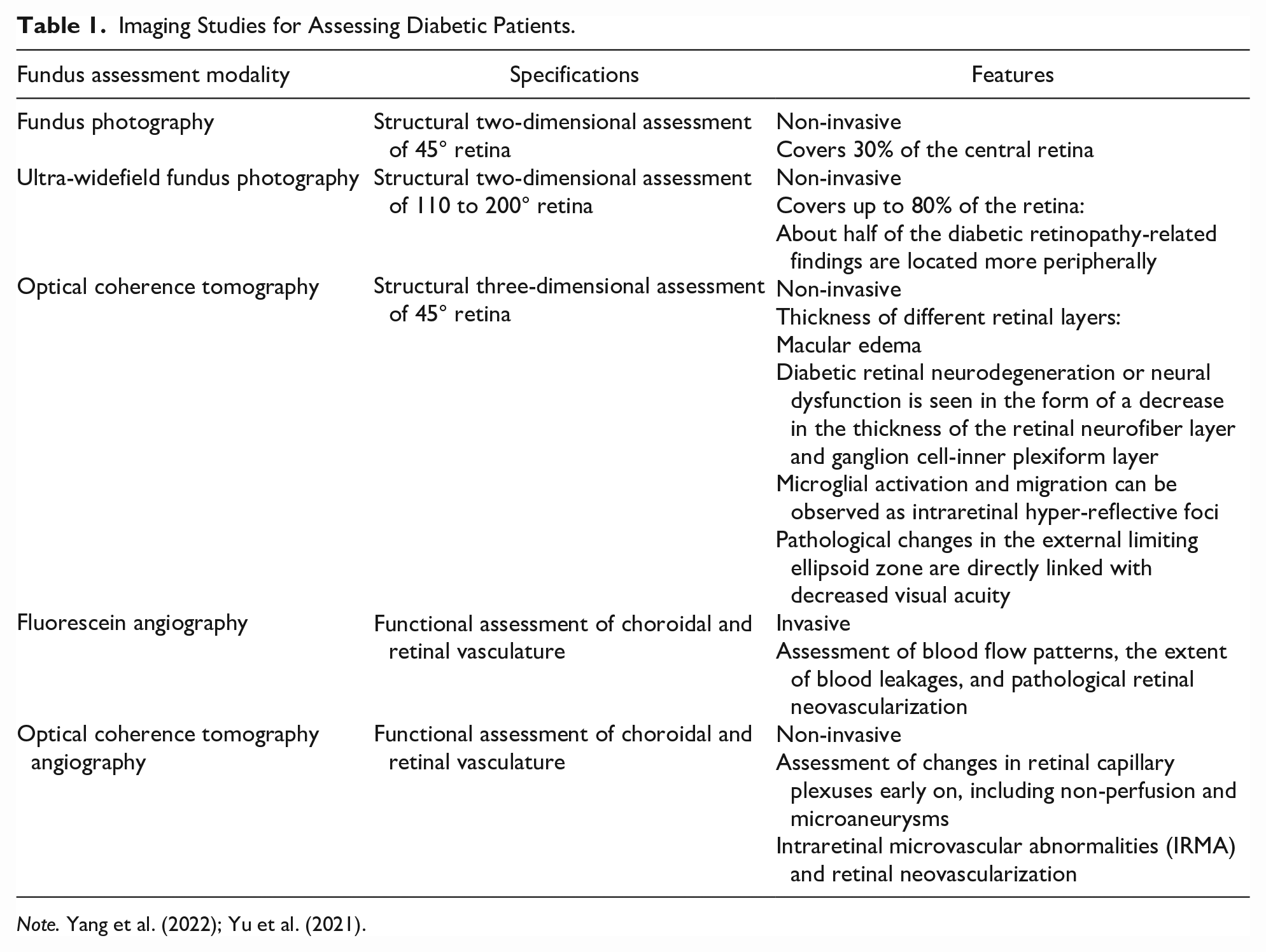
Note. Yang et al. (2022); Yu et al. (2021).
Early Treatment Diabetic Retinopathy Study (ETDRS) is the widely accepted standard for the classification (Bowling, 2015; Solomon & Goldberg, 2019). Management of non-proliferative DR includes careful assessment of the ocular findings and communicating with the primary care doctor to achieve control of the blood sugar levels (Arabi et al., 2022). Hypertension is another well-recognized risk factor for vision impairment in diabetic patients. Adequate control of blood pressure has a significant benefit in preventing DR-related vision impairment by reducing the dysfunction of endothelial cells (Arabi et al., 2022; Lee et al., 2015; Raum et al., 2015).
Panretinal laser photocoagulation (PRP) treatment is the gold standard therapy in proliferative DR, and intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections are the first choice to treat center-involved diabetic macular edema. Anti-VEGF injections are also combined with PRP to treat proliferative DR (Tatsumi, 2023). Advanced diabetic eye disease, including tractional retinal detachment and persistent blood leakage into the vitreous cavity, is managed using a surgical vitrectomy (Tan & Wong, 2022).
Methodology
The Delaware Nursing Home Eye Study (DNHES) by Andersson et al. (2020) is the largest population-based eye care study on long-term care patients describing vision loss in Delaware nursing homes. A second study by Monaco et al. (2021) extended the results by quantifying the associations between vision loss and primary age-related eye diseases.
Our study analyzes the prevalence rates of diabetic retinopathy and undiagnosed diabetes among Delaware skilled care and assisted living residents. Unlike our earlier reports, age was not used as an exclusion criteria in this study.
All patient data were initially de-identified. The institutional review board at Salus University in Philadelphia approved the study for the exemption of a project involving human subjects, and the study followed the tenets of the Declaration of Helsinki.
The following inclusion and exclusion criteria were established for this study:
Clinical Assessment.

Results
Initial patient visits of 2,093 residents met the inclusion criteria of the study. Of these, 30 residents were eliminated because of the lack of demographic data. The resultant study sample was 2,063 residents.
% Distribution of Delaware Nursing Home and Assisted Living Facility Residents by Age, Gender, and Race.

Dot and/or Blot Hemorrhages and Diabetes Cross-Tabulation.

Discussion
Diabetes is a growing, life-debilitating disease that may be considered an epidemic (Forbes & Cooper, 2013; Yu et al., 2021). Unrecognized diabetes forms a significant part of the total prevalence and remains a public health challenge (Centers for Disease Control and Prevention, Data and Statistics, 2022). A significant number of diabetic patients will develop vision-threatening DR (Zetterberg, 2016). Vision is essential for maintaining sufficient physical and social activity levels that allow improved quality of life and promote healthier aging (Andersson et al., 2020). Early treatment warrants significantly better outcomes and is cost-effective (Centers for Disease Control and Prevention, 2010; Rein et al., 2022).
Vascular diseases with ocular manifestations, such as diabetes, cerebrovascular disease, and heart disease related to hypertension, co-occur with vision impairment and are among the 10 leading causes of death (Centers for Disease Control and Prevention, 2013). Ocular posterior segment assessment provides a unique window to observe the retina, an extension of the brain. The retina also has a very rich vascular supply from retinal blood vessels and a layer behind the retina, choroid. The retina is the only body part where cardiovascular functions can be observed, directly reflecting what is happening in different-sized blood vessels throughout the body, providing an opportunity to detect diabetic changes (American Optometric Association, 2019).
Regular eye assessments are recommended for patients with previously diagnosed eye conditions needing follow-up, geriatric patients, and diabetic patients. Institutionalized patients receive health care, offering primary care providers an excellent opportunity to recognize the need for eye care (Centers for Disease Control and Prevention, 2010).
Geriatric eye care providers must be equipped to assess and manage challenging patients, usually suffering from multiple chronic diseases, which can be non-ambulatory (U.S. Department of Health and Human Services, 2010). This can mean providing care in domiciliary or institutional settings instead of typical clinical practice. Competency to deal with complex cases using an evidence-based and interdisciplinarity approach is an essential skill. The interdisciplinary approach requires good communication with all stakeholders, keeping the patient and caregivers at the center of the process.
Although the demographics in this dataset closely resemble nationwide nursing home data, this study did not include sufficient information on Hispanic and Asian races. Therefore, study results reflect and are limited to white and black populations.
The second limitation of this study was that it included all patients with blot hemorrhages. However, blot hemorrhages are present in hypertensive retinopathy in more severe staging, and the other conditions contained in the differential diagnosis have a low prevalence (Bowling, 2015).
Conclusion
The high prevalence of dot and blot hemorrhages without a systemic diagnosis of diabetes indicates that undiagnosed diabetes is a public health challenge in nursing homes and assisted living facilities that should be addressed proactively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval Statement
The institutional review board at Salus University in Philadelphia approved the study for the exemption of a project involving human subjects, and the study followed the tenets of the Declaration of Helsinki.