
Abstract
This qualitative narrative study presents three stories told by older community-dwelling partners to spouses moving into long-term care facilities because of cognitive decline. Applying Alvesson and Kärreman’s mystery method to these stories reveals that when spouses’ caring needs increase, care partners must take on increasing loads of practical work and responsibilities. These partners become lost in the transitions between care work, extended family, and attending to their couplehood. When their spouses move into long-term care, living apart presents new challenges of care and couplehood, each day presenting new and unforeseen tasks to manage. Our findings suggest that if couplehood is to be maintained, well-established habits and work division between the spousal partners are both drivers and barriers. It necessitates agency, creativity from the community-dwelling partner, as well as a supportive extended family and sufficient economic resources. More knowledge is required regarding the interdependent expectations between the next-of-kin, long-term care residents, and caregiving staff members.
Keywords
What does this paper add?
Older community-dwelling partners face unexpected and excessive demands when trying to uphold couplehood after their spouse develops cognitive decline and moves to a long-term care facility (LTCF).
LTCFs can assist and support residents and their partners in upholding couplehood by acknowledging efforts taken and hereby easing the everyday challenges of living apart.
Community-dwelling partners can be included in planning care and everyday activities for their institutionalized partner to ensure that the couple’s needs and wants are acknowledged and addressed.
Applications of study findings
Community-dwelling partners need various forms of emotional, social, and practical support when caring for a spouse who develops severe cognitive decline.
LTCFs must provide structural, material, and social resources to support the continued upholding of couplehood for partners living apart.
Staff at LTCFs must consider how they can involve community-dwelling partners in everyday planning for their residential spouse.
Moving together into LTCFs should be an option for older couples, irrespective of only one party being eligible for long-term care.
Introduction
Moving From Home Into Long-Term Care Facilities
Moving from home to a long-term care facility (LTCF) is a transition (Coleman & Boult, 2003) that is considered stressful, challenging, and energy-consuming for individuals experiencing cognitive decline and their community-dwelling partners (Groenvynck et al., 2021; Munkejord et al., 2020; Saragosa et al., 2022; Shaw & Csikai, 2024). Researchers suggest that the transition is a three-step process with three phases of care (the pre-transition, mid-transition, and post-transition phases) (Groenvynck et al., 2021, 2022; Hainstock et al., 2017). The first step begins with a discussion regarding moving to an LTCF and concludes when a decision is reached. In the mid-transition phase, preparations are made to move into an LTCF, from being on a waiting list to leaving home. The third phase starts after a spouse has moved to an LTCF and revolves around adaptation and acceptance by both parties (Torgé, 2018, 2020; Wada et al., 2020). This three-step transition represents a massive transformation for the community-dwelling partner in terms of their identity, autonomy, social status, relationships, and daily life (Wada et al., 2020). According to Groenvynck et al. (2021), the community-dwelling partner may require continual support, open communication, regular information, sufficient time to adapt to the new situation, and the need for a partnership throughout the transition from home to a nursing home. The community-dwelling partner’s transition is from being a carer back to being a spouse, from being twosome to being alone, and from having easy-to-follow circumstances of life to a life that can be difficult to grasp.
Existing studies that highlight this transition mainly focus on issues faced by the person moving to the LTCF, overlooking the needs of the partner left behind (Hammar et al., 2021; Munkejord et al., 2020; Scott & Funk, 2023). However, couplehood does not cease when one of the partners moves out of the home (Førsund et al., 2016; Gallagher & Beard, 2020; Shaw & Csikai, 2024; Stefánsdóttir & Sveinbjarnardóttir, 2019; Swall et al., 2020). The partner who remains at home may suddenly become unwell due to feeling left alone, overwhelmed and confused regarding their new relationship status, tasks, and role in their spouse’s transition to an LTCF (Anker-Hansen et al., 2018; Clark et al., 2019; Colquhoun et al., 2019; Hammar et al., 2021; Munkejord et al., 2020; Stefánsdóttir et al., 2021). However, we acknowledge that many may feel pleasure and relief at the fact their partner was relocated to LTCF.
This article presents three older community-dwelling partners’ stories about what they did and how they coped with their spouses’ transition from home to an LTCF. Their stories are analyzed as narratives, giving us access to first-person experiences and how they are shaped and affected by the broader social and material contexts in family life, the community and within institutional care. The following research questions have guided the selection of narratives and the following analysis and discussion: What unforeseen challenges emerge when a life partner develops cognitive decline and eventually moves into an LTCF? What can we learn from community-dwelling partners about their end of living together when their spouse needs to move to LTCF because of cognitive decline? We aim to create knowledge about the end of living together by highlighting turning points in these partners’ lives concerning their spouses’ transition and interactions with healthcare staff.
Theoretical Framework of the Study
We explore leaving home and transitioning to an LTCF through the theoretical lenses of critical gerontology and family systems theory. Critical gerontology provides an understanding of what it entails to have a spouse who develops cognitive decline. It adds a critical sociological approach to analyzing the material, cultural, and contextual conditions and circumstances that affect these transitions (Baars, 1991; Hooyman & Kiyak, 2008). A theoretical lens from family systems theory was applied to the three stories of community-dwelling partners (Bowen, 1993), to provide insight into the underlying family dynamics.
Since the 1950s, professionals have used systems thinking when studying families with marital conflict or dysfunction with the spouse (Bowen, 1993). When one family member experiences a transformation, the entire family system is transformed. In other words, the well-being of each family member and that of the entire family are interdependent and interrelated. When one member of a couple has a functional loss, such as cognitive decline, it affects the entire family system of relationships, societal life, financial condition, and housing status, like ripples in water.
However, families and primary carers react in various ways during this transition. For example, they may perceive themselves as having little control over their relative’s care provision or refuse publicly provided service options (Scott & Funk, 2023). Applying critical gerontology and family systems theory in interdisciplinary practice with older couples seems to bring about a change in mindsets and working methods, as the stories presented below show.
Methodology
Setting, Participants, and Recruitment
A qualitative narrative design was chosen based on critical gerontology and family systems theory to understand better older community-dwelling partners’ experiences and family-related connections (Caine et al., 2022; Creswell & Poth, 2018). The empirical material for this article is strategically selected from a larger qualitative comparative study of couplehood, aging, cognitive decline, and LTCFs in Norway and Iceland (Munkejord et al., 2020; Stefánsdóttir et al., 2021). Norwegian participants were invited to participate through advertisements in a local newspaper, and Icelandic participants were invited through gatekeepers (staff leaders) in LTCFs. Eligible participants from the comparative study (n = 25) who agreed to participate were above 67 year old. They had personal experience of caring for a spouse with cognitive impairment at home, and with having a spouse in an LTCF. Semi-structured face-to-face interviews (one with each participant) were conducted at the participant’s homes, lasting 1 to 2 hours; see Table 1 for details. The first author conducted the interviews in Iceland, and the second conducted the Norwegian interviews. The interviews were digitally recorded and transcribed verbatim, and NVivo software was used to manage the raw data.
The Interview Guide.

The three selected interviews were chosen as paradigmatic and rich stories about older people who had enjoyed or endured several relationships during their lifetime and were about to transition from living together to living apart. The stories are rich in detail, which allows for in-depth analysis and a few cases (Boddy, 2016). The transcribed interviews are analyzed as narratives and are re-analyzed with a different method for a different purpose, which is reported in the present article. The narratives presented below are rewritten from raw data to readable stories, in our words, which means highlighting specific features for our specific purpose, that is, creating knowledge about the end of living together and the transition to LTCF.
The participants in our study were recognized as active and agentic citizens who shape their realities through actions and interactions with family, friends, care staff, and researchers (Creswell & Poth, 2018). The authors brought different experiences and qualifications to the study: the first is an occupational and family therapist, the second is a social anthropologist, and the last is a physiotherapist and sociologist. All three are qualified qualitative female researchers on aging and cognitive decline. The Consolidated Criteria for Reporting Qualitative Research checklist (COREQ; Tong et al., 2007) was used to guide and ensure the quality and trustworthiness of the research design.
Analytical Approach
Transcripts were analyzed using Alvesson and Kärreman's (2011) mystery method, which encourages the development of new theories rather than fitting the data to an existing theory. The mystery method has taken its name from traditional crime mysteries to underscore the importance of an open and creative approach to any empirical material and cautions researchers about foreclosing the analysis without looking for less apparent explanations, for example, contextual factors from the first marriage that re-emerges when moving cognitive decline progresses, and from home to LTCF is a fact. Alvesson and Kärreman’s process is explained as a stepwise process, but in real-life settings, it is an iterative process. The stepwise description of the process makes visible how researchers must be at pains to detect “mysteries” and their “solution,” that is, pinpoint a problem that needs to be solved (research question, research gap, lack of knowledge) and offer their contributions to the existing body of knowledge on the topic (“solution of the mystery”). Alvesson and Kärreman suggest that researchers, as detectives, bring necessary “tools” to facilitate the solving of the mystery. Our “tools” are critical gerontology and family systems theory, middle-range theories that call attention to contextual factors affecting social processes (Baars, 1991; Bowen, 1993; Hooyman & Kiyak, 2008).
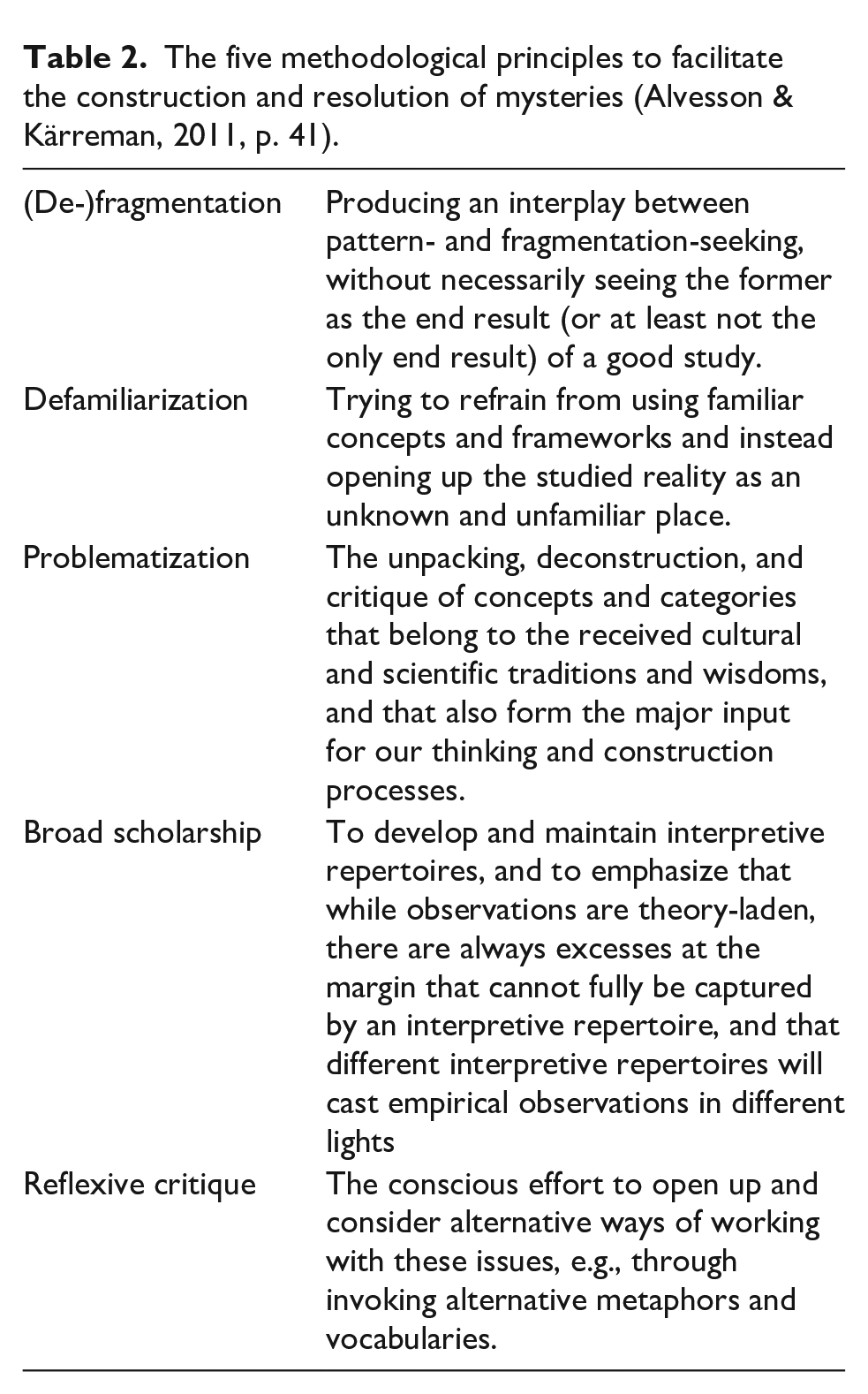
The five methodological principles (de-fragmentation, de-familiarization, problematization, broad scholarship, and reflexive critique) offered a beneficial approach to constructing and solving the mysteries uncovered in the stories; for example, how do we understand the actions and non-actions of spouses as agency and competency? Each step of the analytical process is shown in Table 2 (Alvesson & Kärreman, 2011, p. 41). When re-reading the material, variations and contradictions emerged, for example, from helplessness to proactive action. By closely reading the empirical material, alternative stories about aging and transitions emerged. After numerous data revisions and discussions, we discovered a common mystery or phenomenon of interest in these three stories, which indicates that the community-dwelling partners were lost in the transition of their spouses from home to an LTCF.
The five methodological principles to facilitate the construction and resolution of mysteries (Alvesson & Kärreman, 2011, p. 41).
Ethical Consideration
Formal ethical permissions to undertake this study were obtained in Norway and Iceland. All the Icelandic participants provided written consent to participate in the study, but in Norway, it was oral and stated at the beginning of the interview recording. All participants were informed about the research aims and assured their identities and records would remain confidential, and they were free to leave the study at any stage.
Three Paradigmatic Narratives
A paradigmatic narrative calls attention to patterns, contradictions, muted issues, and ignored features of the subject matter, challenging us to reconsider earlier interpretations and prejudices. A thorough analysis of select paradigmatic cases or single cases can uncover knowledge with broad relevance (Boddy, 2016; Caine et al., 2022; Creswell & Poth, 2018).
Ingibjörg
Ingibjörg and Friðrik met when she was 15 and he was 20 year old, and soon became a couple. Ingibjörg said that their couplehood never felt safe; they were neither close nor happy together. However, they worked well together on practical things, such as gardening, and maintaining their home and summer house, and these projects somehow kept them together. They experienced various difficulties. They had two daughters, one of whom was seriously ill as a child, and Ingibjörg’s sole task was to care for her. Friðrik was temperamental and tended to be both dominating and aggressive. He despised chaos or noise, leading Ingibjörg to constantly tiptoe around him to prevent his next tantrum. Over the years, she seriously considered divorcing him, as their life together was painful, at times.
When Friðrik was 75 year old, he became paralyzed and later developed cognitive decline. Ingibjörg instantly put everything else aside—friends, hobbies, knitting, children, grandchildren, and even her doubts about her entire marriage. Her whole life revolved around caring for Friðrik and helping him with his daily activities and needs. After 2.5 year of taking care of him around the clock, Ingibjörg’s health deteriorated, and she had a broken heart syndrome 1 and developed psychosis owing to prolonged stress and sleeplessness. Before her breakdown, she informed the home-care staff multiple times that she could no longer manage the situation. Friðrik was then offered a place in a nursing home, which he refused. When Ingibjörg returned from the hospital some weeks later, Friðrik alternated between spending 2 week in an LTCF and 2 week at home. However, even when in the LTCF, he insisted that Ingibjörg do the care work, such as assisting him in washing, dressing, and eating. Subsequently, Ingibjörg experienced two more nervous breakdowns at short intervals with associated hospitalizations. After her third hospitalization, she realized that if she were to survive herself, she could not return home; therefore, she moved to their summer house. She informed her daughters and the healthcare staff that she would remain there until her husband moved permanently into the LTCF because she could no longer take care of him. Ingibjörg shared her feelings of disappointment and rejection that even after repeatedly informing the home-care staff about her health situation and three breakdowns, her own health was not prioritized. Only her husband’s wish to stay at home was heard. At the end of the interview, she bitterly asked, “When will the municipality act?”, answering the question herself, “Never!”
Bjørn
When Bjørn (91) and Lára (86) met, he was a widower with four children from his previous marriage: two sons who lived abroad and two daughters who were both deceased. Lára was divorced with three children from a previous marriage who lived nearby. At the time of the interview, the couple was married for over 20 year. Bjørn told us that they had been happy together and enjoyed a close relationship for 15 years until Lára developed cognitive decline, which radically changed their relationship. Bjørn had always done the grocery shopping and cooking, which he enjoyed. They liked spending time together as a couple, and for a long time, they traveled abroad at least twice a year. Lára had recently been diagnosed with Alzheimer’s, and her children decided that the best solution was for her to move into an LTCF. Bjørn was not involved in the application process. He shared with us: I tried to tell her family and the healthcare staff that I wanted to move in with her [to that LTCF]. Nonetheless, his wishes went unheard, he told us. Lára was admitted to an LTCF with the assistance of her children while he remained alone at home. All he wanted was to go with her; however, 18 month passed before he was accepted into the same LTCF, finally able to live with his wife again. Bjørn shares that he felt terrible during those 18 month. It was such a difficult period! he said. During this time, he fought the system by writing applications, making phone calls, pleading with the manager of the LTCF to move in with his wife, and continually re-explaining his situation. At the time of the interview, he had been in the LTCF (with his wife) for 2 month. He said it seems that they do not want to have couples together here. We are the only couple in this unit. It should be an option. People should be allowed to choose. Ultimately, Bjørn stresses how fulfilling it is for him to be with his wife after their long separation. He also told us that Lára wanted him close and that she always asked for him if he was not around and tended to become agitated in his absence. However, she was calmer and more content when they were together.
Berit
Berit (79) and Oskar married when she was 54, and he was 62 year old, and they were married for 17 year. Oskar passed away 7 year before the interview. When they met, he was a widower with two children from his first marriage, whereas she was divorced with three adult children. Berit decided to retire early, which gave them five great years together before Oskar was diagnosed with Parkinson’s disease, later correctly identified as Lewy Body Dementia. His health quickly declined, but Berit cared for him for several years with no support from the municipal care services. Symptoms of Oskar’s illness included hallucinations, restlessness, difficulties maintaining balance, and kicking and punching in the air. Sometimes, Berit woke up with a black eye from his “blind boxing” in his sleep. Berit did not like the idea of an LTCF but chose to apply for a part-time room (2 week on, 2 week off) when she realized that she could not care for him alone full-time. When he was home, they did not engage any home-care services, and Berit took care of him entirely on her own; she got him out of bed in the morning, by using a rope tied to the window post. He was able to use his arms to assist with this process. She supported him with all activities of daily living. Her main challenge, however, was that she could never leave the house without him, as he could not be trusted to not climb the stairs, risking a debilitating fall. It was also challenging when they needed to go shopping, as they lived on the second floor. When they could no longer use the stairs, they used the veranda exit from the living room, crossing the hilly garden assisted by a rope and chair. When shopping for groceries, he always accompanied her, using a wheelchair between the parking lot and the store. When Oskar stayed in the LTCF, Berit visited him daily for 3 hour, providing light therapy and coffee, stimulating his memory by asking questions and taking him outside. According to Berit, the food being served in the LTCF was not impressive; for example, they served dry, tasteless bread, instant meals, and porridge on Saturday, food that Oskar would never have eaten previously. Therefore, she brought him yogurt, eggs, fruit, wine, and so on. This was her way of maintaining some sense of dignity and continued couplehood. Although she visited her husband daily and contributed substantially to his well-being, Berit never felt welcome by the care staff. For example, she and Oskar were not welcome to have a cup of tea in the living room because visitors were only allowed in the residents’ own rooms. Eventually, Oskar fell and broke his pelvis while in the LTCF. Berit realized that the time had come to apply for a permanent place in the LTCF because she could no longer bring him home and safely care for him. When the staff at the LTCF wanted to send him home, she said they were welcome to do so, but they would have to ensure that Oskar was cared for because she was going on vacation: Here is the key to our home. I am leaving tomorrow, she said. This was how she secured a permanent room in the nursing home.
The Impact of the Cognitive Decline on the Couplehood
Transitioning from a partner to a full-time carer is often challenging (Clark et al., 2019; Colquhoun et al., 2019). When the cognitive impairment is minimal, couples often cope by developing new routines and daily strategies. As cognitive decline advances, a need for home-based care and support emerges (Hammar et al., 2021). When Ingibjörg’s story is de-fragmented, their couplehood story emerges. The front-stage story of a happy marriage hid issues backstage, wherein their marriage was reduced to division of labor. However, when Friðrik falls ill, analytical defamiliarization shows us how Ingibjörg completely sets aside her needs and interests to become her husband’s full-time career. Before his decline, she had considered divorcing him. However, Friðrik does not change his style; he continues to be emotionally distant and becomes even more demanding. Analytical problematization of her story accentuates the fact that her needs are not acknowledged even after she has suffered three nervous breakdowns and hospitalizations. Her story calls attention to the culture at LTCFs, wherein the care staff provide services to Friðrik, ignoring the needs and capacities of the patient’s family members. This story illustrates how ignoring the care partner’s needs may leave them requiring long term as well.
First Marriages and Their Impact on the Second
When Bjørn and Lára’s story is broken down, analytical defamiliarization allows us to consider the fact that they are both in their second marriage. According to family systems theory, combined families are more complex (i.e., couples in their second and third marriages with children from previous relationships). His wife’s first marriage plays into their relationship through her children. Our empirical material is Bjørn’s story, and we have no direct account of the children’s or LTCF staff’s views and opinions. However, our analysis leads us to question whether her children merely want to act as guardians and proxies for their mother, or if they distrust Bjørn. This adds to Bjørn’s grief of losing his wife to the LTCF. From an analytical perspective, it is a challenging experience for Bjørn not to receive any support from the staff at Lára ’s or his own LTCF. This begs the question of whether the staff care about separated spouses, answer to children or spouses, or whether they recognize the challenges but do not have the means to address them.
Between Maintaining and Letting Go of Caregiving
As discussed, care partners often struggle to hand over their caring obligations (Cash et al., 2019), as exemplified in Berit’s story. She continued showing consideration and solicitude for her husband until his death, first at home and later in the nursing home. She also attempted to manage without home-care services for a long time. Berit’s story tells us that she found it uncomfortable that they were only allowed in her husband’s room and were not welcomed to the LTCF living room as a couple. We do not know whether this is to protect other residents from seeing the treats and generosity that Oscar receives from his wife, the staff’s discontent with her concerns, or the role Berit is ascribed by the staff. For Berit, this led to unease, insecurity, and decision paralysis. Additionally, it is pertinent to inquire whether Berit feels caught between providing and surrendering caregiving responsibilities (Torgé, 2020). For her, being able to assist her husband with everyday chores in the LTCF can be interpreted as acts of love rather than doing mere “care duties” as salaried staff are expected to do.
Discussion
On analyzing these three stories using the five-step mystery method (Alvesson & Kärreman, 2011), our findings indicate that the partners felt lost in their efforts to translate or understand their spouse’s transition between home and the LTCF. Community-dwelling spouses risk becoming worn out from physical, functional, economic, personal, relational, and cultural challenges, and misunderstandings or communication breakdowns. They unwillingly respond to the duties and tasks forced upon them and are continuously negotiating the roles they are ascribed or have achieved. They enact the roles of transporters, housekeepers, logistics, cooks, and cleaners, that is, doing all of the chores that they used to share with their spouses. Furthermore, they enact lover, friend, and partner roles. Simultaneously, the burden of caring at home perpetually increases, which elicits mixed feelings, such as (im)patience, gratitude, sadness, anger, angst, and exhaustion. The three stories reveal that the family system is at risk of breakdown when lifelong habits are disturbed or broken. They tell stories of malfunctioning family systems that require relief, amendments, and support. Therefore, the storytellers felt abandoned and lost during the transition and translation between systems.
Using qualitative narrative research, a thorough analysis of the material revealed valuable knowledge and insights which may be relevant to larger populations and audiences. We suggest four areas wherein appropriate support can be offered to community-dwelling partners who are left alone at home.
First, community-dwelling partners might benefit from interdisciplinary healthcare professionals’ support in voluntarily deciding the activities they want to participate in and choosing their role in their spouse’s transition process (Groenvynck et al., 2021). Growing research on couples and cohabitants living apart in old age has enhanced our awareness that couplehood does not end abruptly when one of the partners needs to move into an LTCF (Stefánsdóttir et al., 2021). Relationships and intimacy have equal importance in later years. Nevertheless, the roles change, and care partners have to assume responsibility for housing, financing, and decision-making and advocate for them as a couple.
Second, through these stories, we consider how caregiving affects married life and how marital history affects caregiving. Echoing the findings of Graneheim et al. (2014) and Torge (2020), we found that when spouses have developed caring patterns over several years, or even decades, of couplehood, handing them over to others is not easy. Cash et al. (2019) argue that caregiving is an expectation of couples in long-term marriages, regardless of the relationship’s quality and spouses’ willingness to care. This applies to Ingibjörg’s story, as she changes her priorities to take on full-time care of Friðrik, despite the apparent lack of intimacy throughout their couplehood. Such normative expectations can affect decision-making concerning future care planning and transition to an LTCF and come at a cost. Ingibjörg and Berit show us that the burden of care poses a risk to their health and well-being. The costs of family-based care must be considered when developing or revising policies for elder care.
Third, the three stories call attention to the structural and administrative organization of LTCFs. To our knowledge, few LTCFs are designed to support the maintenance of close personal relationships between community-dwelling partners and admitted spouses. Community-dwelling partners constantly face unexpected and excessive demands when maintaining couplehood-like relationships after their spouses enter LTCFs. To sustain couplehood, partners should be included in planning care and everyday activities for spouses living in LTCF. This issue is crucial in future discussions of services for older couples and cohabitants, and when considering adapting structural, material, and social resources provided by LTCFs to support couplehood under any circumstances.
Fourth, analyzing these stories using Alvesson and Kärreman's (2011) mystery method contributed to unique outcomes and novel insights into the topic of transitions from home to LTCFs. According to the existing literature on the topic, Ingibjörg, Bjørn and Berit would easily emerge as vulnerable and powerless individuals at the mercy of the LTCF and the healthcare system at large (Anker-Hansen et al., 2018; Munkejord et al., 2020; Seaman, 2018; Tatangelo et al., 2018). However, through a systematic hunt for a mystery to solve, phrased as “What happens when someone gets lost in transition?,” the five-step mystery method (de-fragmentation, de-familiarization, problematization, broad scholarship, and reflexive critique) facilitated an alternative reading and interpretation of the narratives, allowing counternarratives of helplessness to emerge. The storytellers relate about exercising agency, maneuvering in treacherous waters, and how they try to do what is best for themselves and their spouses while managing expectations from the LTCF.
Lastly, this interpretation uncovers the community-dwelling spouses’ stamina and unwillingness to give up; they are advocates for their partners, wanting to retain their rights and take control of their couplehood and situatedness. However, the system may not entirely favor them owing to laws and standard procedures. However, these narratives highlight that community-dwelling partners need emotional, social, and practical motivation, reinforcement, and support, both when living at home with a spouse developing cognitive decline and when their partner has moved into an LTCF (Saragosa et al., 2022; Zmora et al., 2021). Our data does not provide specific evidence that the home-care phase is more or less taxing than the LTCF phase, which appears to vary on an individual level. Allowing for such dialogs will inform professional care workers, whether homecare and in LTCFs, about competencies, agency, needs and wants of the individual spouses and their couplehood. Furthermore, our findings add to the body of knowledge on family systems theory and the sociology of aging.
The stories in this study are used as paradigmatic examples of how qualitative material can be re-interpreted. Nonetheless, not all participants in the larger study experienced loss in their spouse’s transition process. For example, seven interviewees were satisfied with the LTCFs’ services. They felt welcomed at the nursing home as spouses. They were invited to have coffee and dinner with their spouses and could visit them as they pleased. They also felt great relief in obtaining support and assistance with their spouses’ care, both at home and after their move to an LTCF. They appreciated having the healthcare staff listen to and empathize with their account of hardships faced in caring for their spouses. Finally, being able to rest, think, and go about their life while continuing to be a partner, without carrying the constant burden of care for their spouse, brought great comfort.
Conclusion
This study presented paradigmatic examples of how community-dwelling partners exercise agency and stamina by exploring possibilities and engaging resources to maintain couplehood and ensure their spouses receive appropriate care in LTCFs. They reveal how their ruler of everyday life capacities are used strategically, and how they assertively demonstrate their needs and expectations in complicated situations. However, the underlying demand for a partnership throughout the transition process is missing from these three stories. Consequently, community-dwelling partners feel lost in their spouses’ transitions into an LTCF. Our contribution to the literature is to endorse the need for professional interdisciplinary support for and acknowledgments of community-dwelling partners agency, in parallel with their spouse who is in an LTCF. Cognitive decline is more than an individual diagnosis; it is a condition that affects couples and families and should be comprehensively examined at the social and relational level in gerontology rather than only focusing on the patient’s illness as an individual geriatric medical problem (Gallagher & Beard, 2020; Shaw & Csikai, 2024). The family-centered approach to helping couples sustain couplehood should depend on the acquired practices at the couple’s home before, during, and after the spouses move into an LTCF, and in the larger social context of housing, family, and financial status (Groenvynck et al., 2021). More knowledge is required regarding the mutual expectations between next-of-kin, LTCF residents, and healthcare staff. Without any changes, community-dwelling partners are at risk of being lost and exhausted in caring for their spouses.
Footnotes
Acknowledgements
The authors sincerely thank the study participants for sharing their time and experiences during the interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study’s necessary permissions in Iceland were obtained from the National Bioethics Committee (VSN-18-149), and in Norway from the Norwegian Centre for Research Data (NSD-48366).
Data Availability
We will share our research data in a relevant public repository, including data availability linked to our data.