
Abstract
This study investigated how elderly individuals’ exercise satisfaction in snowy areas relates to their health indicators and future care needs. Survey data were collected from individuals aged ≥65 years who lived in snowy-cold regions. Participants completed measures of exercise satisfaction, frailty, quality of life (QOL), and cardiovascular health study during the winter and spring of 2019, with a follow-up measure in 2022 to assess care needs. Findings revealed an association between exercise satisfaction, QOL, and frailty indicators, irrespective of the season. Notably, winter exercise satisfaction showed a stronger correlation with future care needs compared to spring exercise satisfaction. Those expressing low winter exercise satisfaction were significantly more likely to require increased care 3 years later than those reporting no inactivity. Although physical activity was not measured directly, the findings underscore that perceptions of exercise satisfaction during snowy seasons can predict future care needs in older adults. The influence of seasonal variations and subjective exercise satisfaction on long-term care requirements is vital for tailored interventions and improved healthcare strategies for older adults in cold regions.
Introduction
The importance of physical activity for older adults cannot be emphasized enough, and comprehensive care must include the promotion of physical activities (World Health Organization, 2017). Physical activity refers to both activities of daily living (ADL) and exercise. It contributes to health in various ways and is assessed using questionnaires and activity meters, with each having specific difficulties. For example, questionnaire-based assessments are subject to bias when answering complex questions and to memory recall. Whereas, evaluation using an activity meter involves difficulties such as handling of the device and remembering to put it on (Lee et al., 2013).
Self-evaluation (i.e., a sense of inactivity or satisfaction with own physical activity) is a simpler way to measure one’s physical activity level. Self-evaluation of physical activity level is easy and may be a useful indicator to promote physical activity, especially for those who have low self-evaluation; that is, those who are dissatisfied with their own physical activity status. Sakurai et al. (2012) compared exercise satisfaction with actual physical activity level measured by a physical activity meter and mentioned that people who are highly satisfied with their physical activity level often reported higher levels of it.
Although exercise satisfaction is subjective, it correlates, to some extent, with the objective physical activity level (Sakurai et al., 2012). If a person’s physical activity satisfaction matches the objective physical activity level, it can be used to indicate the amount of physical activity. Otherwise, it can be used to understand their health literacy level. In addition, for individuals with low satisfaction with physical activity, interventions aimed at promoting physical activities are likely to succeed if the person is clear with the reasons and is appropriately involved.
Physical activity involves challenges specific to snowy regions, and previous studies have confirmed that physical activity tends to decrease in winter (Garriga et al., 2021; Hasegawa et al., 2018). Health and medical professionals in snowy and cold regions may often encounter that older people feel more inactive because they go out less frequently during snowy seasons; however, it is unclear whether there are seasonal differences in the relationship between physical activity level and other health indicators such as the status of frailty and health-related quality of life (QOL). Moreover, restrictions of physical activities for nearly 6 months in the winter may be a precipitating factor for a subsequent decline in physical function. However, there are no reports on the relationship between exercise satisfaction and future nursing care needs or on the seasonal differences mentioned above.
Therefore, this study examined the relationship between satisfaction with physical activity and other health indicators and the level of care needed 3 years later, focusing on seasonal differences.
Methods
Participants
Elderly individuals aged 65 years or older who were living independently in the community and were members of senior citizen clubs in Tobetsu Town (northern Japan) participated. Senior citizen clubs are organizations established in each neighborhood association for voluntary participation by senior citizens, where they get together to socialize and participate in various activities and events. Those who were certified as requiring nursing care at the beginning of the survey—for example, those in home care/day dare services or facilities—were excluded.
The 2019 winter questionnaire was distributed to 260 people, and 181 responses were collected (response rate = 70%). The spring questionnaire was sent to 178 of the 181 people, excluding three whose address at the time of the survey was unknown: 158 questionnaires were collected (response rate = 89%). The data for winter and spring were valid.
For the 2022 follow-up survey, questionnaires were mailed to 178 respondents to whom the spring questionnaire was sent. Of them, 145 responded (response rate = 81%); thus, 145 individuals responded to all three surveys (Figure 1).
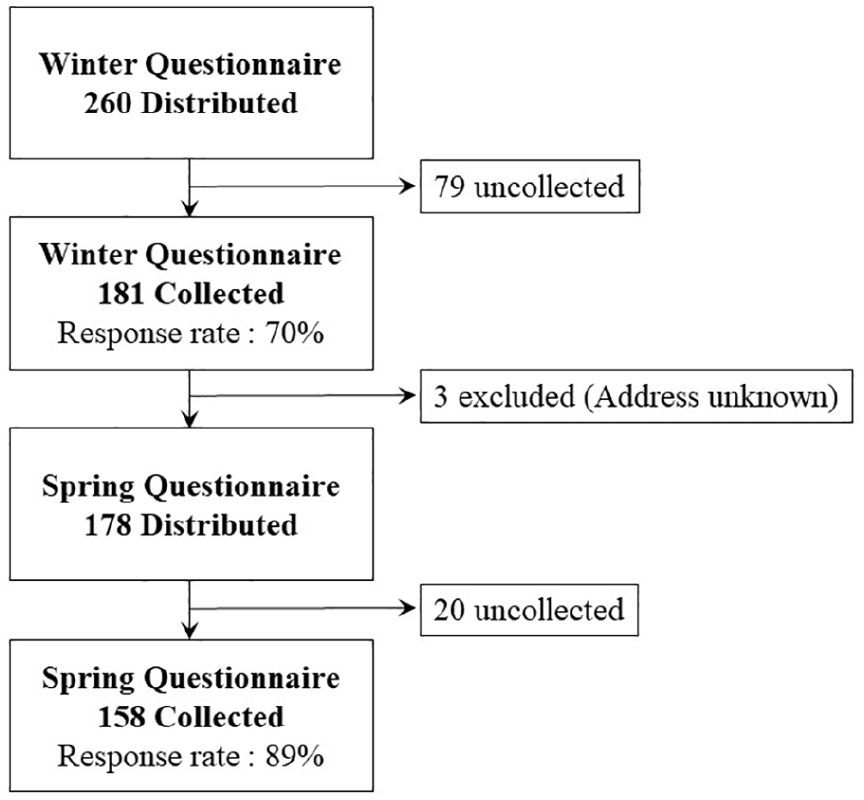
Participant selection flowchart.
Procedure
After receiving verbal and written explanations about the research from the principal investigator, participants decided on their involvement in this study. Participants were explained that they could withdraw their consent at any time. Questionnaires were distributed at regular meetings of the town’s senior citizen clubs in January and February 2019 and responses were obtained by mail from those who agreed to participate in the research (winter survey). The second survey (spring survey) was distributed by mail in May 2019 to responses were obtained from those who completed the winter questionnaire. All responses were anonymized using participants’ unique ID number.
In the questionnaire, sex, age, satisfaction with exercise, Cardiovascular Health Study (CHS) criteria, the Kihon checklist (KCL), and the Japanese version of the EuroQoL-5 dimensions-5 levels (EQ-5D-5L) were assessed. As several scales were included, the items were selected by prioritizing simplicity in responding while ensuring validity for each survey item. The KCL, comprising 25 “yes/no” questions, was used to screen the status of frailty (Satake et al., 2016). CHS criteria were used to determine frailty. The following five items were used: (1) weight loss of 2 to 3 kg or more in 6 months, (2) difficulty in climbing stairs, (3) feeling tired without reason in the past 2 weeks, (4) reduced walking speed, and (5) no light or moderate physical exercise/regular exercise or sports. Respondents were classified as frail if answers to three or more of the five questions were true, pre-frail if 1 to 2 were true, and robust if none were true. Regarding satisfaction with exercise, participants were asked whether they felt they were not exercising adequately and were classified into three groups: not at all, somewhat inactive, and very inactive.
Subsequently, in January 2022, a survey was conducted regarding the current level of care required. The level of care required is a classification of the need for long-term care in Japan’s long-term care insurance system and is classified into eight levels: independence, support required (two levels), and long-term care required (five levels). In this study, those who were judged to need support level 1 or more and those who died were classified into one group, and those who could function independently were classified as independent. This study was approved by the Human Research Ethics Committee of the Faculty of Rehabilitation Science, Health Sciences University (no. 18R090084).
Statistical Analysis
A cross-sectional analysis was conducted using the winter and spring data to evaluate whether exercise satisfaction predicted future care needs. The Kruskal–Wallis test was performed to assess the association of exercise satisfaction and the KCL frailty score and QOL score. Fisher’s exact test was performed to find the association between exercise satisfaction and frailty, determined by CHS and KCL scores.
Longitudinal analyses were conducted to examine the causal effect of exercise satisfaction on health (i.e., on future frailty determinations and the level of care needed 3 years later). The association of winter exercise satisfaction and CHS and KCL frailty scores after snowmelt was assessed using Fisher’s exact test. The association of exercise satisfaction in winter and spring with level of care needed after 3 years was assessed using Fisher’s exact test and logistic regression analysis (generalized linear model) adjusted for sex. All data were analyzed using EZR, which is a modified version of R commander (Kanda, 2013). Significance was set at p < .05.
Results
Table 1 summarizes participants’ data. KCL scores were 4.6 ± 3.9 and 5.2 ± 4.0 in the winter and spring, respectively (t(288) = 1.300, p = .19). Similarly, QOL scores were 0.85 ± 0.14 and 0.84 ± 0.15 in the winter and spring, respectively (t(265) = 0.19, p = .84). The percentage of those who felt “very inactive” was higher in the winter than in the spring. However, the percentage of people with “frail” status, based on KCL criteria, was higher in early spring. The frailty assessment based on CHS criteria was unaffected by seasonal influences.
Characteristics of the Study Participants (N = 145).

Note. KCL = Kihon checklist; PA = physical activity; CHS = Cardiovascular Health Study.
Cross-Sectional Data Analysis
A significant relationship was found between exercise satisfaction, QOL scores, and KCL in both seasons (Tables 2 and 3). The contingency tables and p-values for the two frailty measures (CHS and KCL) are presented in Tables 4 and 5. Most of those who responded as “not inactive at all” in the winter were robust. Concurrently, a certain number of respondents felt “very inactive” despite being robust (Table 4). Table 5 shows the proportion of people who were judged as frail. Based on the KCL criteria, more participants reported being “very inactive” in the spring than in the winter, although they reported not being inactive at all.
The Results of Kruskal-Wallis Test According to PA Level (Winter).

Note. KCL = Kihon checklist; PA = physical activity; QOL = quality of life.
The Results of Kruskal-Wallis Test According to PA Level (Spring).
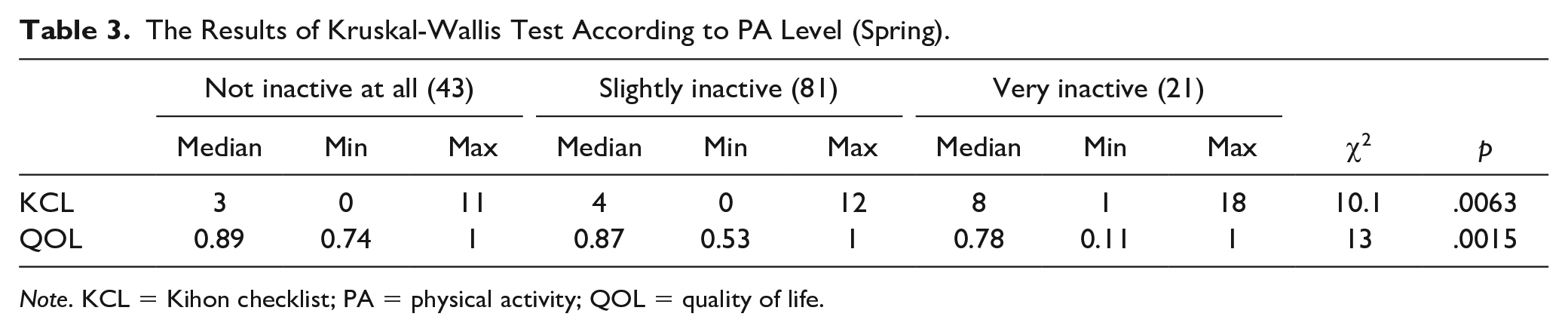
Note. KCL = Kihon checklist; PA = physical activity; QOL = quality of life.
Relationship Between Frailty and Satisfaction on PA (Winter).

Note. KCL = Kihon checklist; PA = physical activity; CHS = Cardiovascular Health Study.
Relationship Between Frailty and Satisfaction on PA (Spring).

Note. KCL = Kihon checklist; PA = physical activity; CHS = Cardiovascular Health Study.
Longitudinal Data Analysis
There was a significant relationship between winter exercise satisfaction and KCL and CHS scores in the spring (Table 6). Logistic regression analysis showed a significant relationship between exercise satisfaction in each season and the level of care needed 3 years later for those who responded that they were “very inactive” in the winter (Table 7). Those who responded, “very inactive” in the winter season showed a significant increase in the level of care needed 3 years later (odds ratio = 10.3; 95% confidence intervals [CI]: [2.10, 50.30]) compared to those who responded, “not inactive at all.” In contrast, the same comparison showed an odds ratio of 2.74 [CI: 0.807, 9.280] in the spring; however, it was not significant (p = .103) as shown in Table 8.
Relationship Between Satisfaction on PA in Winter and the Status of Frailty After Snow-Melt.

Note. KCL = Kihon checklist; PA = physical activity; CHS = Cardiovascular Health Study.
Relationship Between Satisfaction on PA and Care Need in 3 Years.

Adjusted Odds Ratios of Care Needs in 3 Years According to Satisfaction on PA.

Discussion
As shown in Table 1, a wide range of elderly individuals, spanning from early to late old age and from both sexes were included. A notable proportion of participants reported insufficient perceived activity levels during the winter compared to the spring—a trend similar to findings reported in previous research indicating decreased physical activity during the winter months (Garriga et al., 2021; Hasegawa et al., 2018). Frailty was assessed using two criteria: the CHS and the KCL. While the CHS criteria exhibited minimal seasonal variation, the KCL criteria showed an increase in frailty assessments during spring compared to winter. Further, the CHS criteria identified fewer robust individuals and more pre-frail individuals compared to assessments using the KCL criteria. Owing to constraints associated with data collection during the winter season, direct measurements of grip strength and gait speed, which are integral to CHS criteria, could not be conducted. As such, frailty assessment using CHS criteria were treated as reference values. However, the differing methodologies for frailty assessment suggest potential variability in susceptibility to seasonal effects. The CHS criteria, primarily focusing on physical frailty; and the KCL criteria, which include outdoor activities susceptible to seasonal variations, each possess distinct characteristics in frailty assessment. Future investigations should further scrutinize these differences, particularly in conjunction with physical examination-based frailty assessments using the CHS criteria.
The results suggest the validity of exercise satisfaction as an indicator of QOL and psychosomatic functioning. Relationships between exercise satisfaction, QOL, and KCL were observed regardless of season. Exercise satisfaction is also significantly related to the frailty assessment based on the CHS and KCL criteria. The correct perception of own physical activity status has been reported to provide health benefits (Crum & Langer, 2007). The current results were consistent with the CHS criteria. In addition to perception, a high subjective view of health is related to actual health behaviors (Storey et al., 2020). A high exercise satisfaction may promote positive feelings toward exercise and contribute to the health-related QOL as well as health benefits derived from physical activity. Consequently, physical functions, ADL, and instrumental ADL, expressed by KCL scores, improved. Based on these results, exercise satisfaction could be used in clinical practice as a simple screening question for QOL and frailty status.
We examined the longitudinal effects of exercise satisfaction on frailty status. As noted above, an overwhelming percentage of the respondents who reported not being inactive during the winter months were robust, supporting previous research that strong lower extremity muscle strength ensures activity during the winter months (Hasegawa et al., 2018). People with low exercise satisfaction in winter were more likely to be in a frail state after the snow melted in early spring (Table 6). As shown in the cross-sectional analysis, low exercise satisfaction may be associated with frailty. However, notably, exercise satisfaction in the winter, immediately preceding the spring, was more strongly associated with early spring frail status than was exercise satisfaction in the spring. While the lack of exercise during the winter months is temporary, its impact should not be underestimated, as the season lasts for almost 6 months, significantly influencing the frailty situation in early spring. These results suggest that low winter exercise satisfaction affects the resilience of mental and physical functions in early spring. Although the present analysis only focused on the post-snowmelt frailty, it is necessary to examine the resilience of mental and physical functions after snowmelt by assessing whether the post-snowmelt frail status improves before the next winter.
The next step was to examine the long-term effect of exercise satisfaction on frailty. Logistic regression analysis adjusted for sex showed that exercise satisfaction in winter and that after the snow melted predicted the degree of need for nursing care 3 years later. The same results were obtained for spring; however, the results indicated that exercise satisfaction in winter was a more effective predictor. This may indicate that exercise satisfaction in winter is more likely to accurately reflect actual physical performance.
A larger proportion of people in the spring reported being active but would need care in the future compared to those in the winter. Previous studies showed that activity is more likely to be limited in winter; however, it remains consistent in winter if one’s leg strength is maintained (Hasegawa et al., 2018, 2019). If people are aware of their ability to exercise adequately in the winter, they actually maintain physical activity; while in the spring, it is easier exercise outside than in the winter. Therefore, people may feel that their exercise is sufficient in the spring even if they do not get enough exercise to effectively maintain physical functioning.
This study is significant in that it suggests that elderly individuals who are less active in the winter in snowy and cold regions may need nursing care more than those who perceive themselves to be inactive during the winter. Further, the degree of exercise satisfaction may affect the degree of future need for nursing care.
Limitations
This study has some limitations. It did not measure actual physical activity levels, and the causal relationship between exercise satisfaction and future nursing care needs could not be fully explained. Moreover, self-reported data introduces the possibility of response bias. The influence of recall bias owing to participants’ age and social desirability bias inherent in health-related surveys is not negligible; thus, the importance of analyses based on measured data is acknowledged. Finally, this research was conducted in a specific region and the findings may not be generalizable to other geographical areas.
Future Directions
One of the specific health interventions for elderly individuals residing in snowy and cold regions would involve improving indoor exercise facilities accessible during the winter season. Enhancing the accessibility of exercise facilities for the elderly, by considering factors such as proximity to their residences, could prove effective. It is also advisable to explore diverse avenues for creating exercise opportunities tailored to local conditions. This could include leveraging private facilities and community halls, among other options. Moreover, considering the prevalence of digital technology, the provision of web-based exercise classes for home participation could be beneficial. Intensive exercise programs akin to those observed in Hasegawa et al. (2019), which reported increased winter activity levels following participation in such programs during the preceding 3 months, may hold promise for older adults in snowy and cold regions.
Future research endeavors could mitigate data bias inherent in questionnaire-based methodologies by incorporating direct measurements. Additionally, the utilization of large, anonymized datasets comprising physical activity data from smartphones and similar sources could enrich the scope of investigation.
Conclusion
This study sheds light on the significance of perceived physical activity as an indicator of both QOL and physical function in older adults. The observed relationships between satisfaction with own physical activity, QOL scores, and frailty status persisted irrespective of the season, highlighting its consistent impact. Longitudinal analysis revealed that satisfaction with winter physical activity was a stronger predictor than that with spring physical activity, possibly owing to its closer reflection of actual physical performance. Notably, a higher proportion of individuals anticipated the need for care in the future in spring, despite reporting adequate activity levels. The results suggest that adequate exercise satisfaction in winter reflects the actual health status. Although this study did not measure the actual activity data, it provides valuable insights, suggesting that older individuals perceiving themselves as less active in winter, particularly in snowy regions, may require more nursing care in the future and underscores the potential impact of exercise satisfaction on future care requirements. A detailed study should be conducted with actual measurements of physical activity and background factors of satisfaction with own physical activity to verify whether perceived physical activity level influences future caregiving needs.
Footnotes
Acknowledgements
I appreciate the advice and expertise of Prof. Taro Yamauchi of Hokkaido University and Prof. Hideki Suzuki of Health Sciences University of Hokkaido. I am also grateful to Tobetsu Council of Social Welfare. My sincere appreciation is extended to all the participants of this study. I would like to thank Editage for English language editing.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author received no financial support for the research, authorship, and publication of this article.