
Abstract
Social isolation among older adults affects their physical and mental health. Ego-resilience is associated with flexible adaptation to various environments and acceptable behaviors. However, its association with social isolation among older people is unclear. Therefore, a health survey was conducted with 510 adults aged 65 years or older to assess social isolation, its associated factors, and ego resilience. The results showed that the social isolation group had a lower median ego-resiliency scale score (42.0) compared to the non-social isolation group (38.0). The social isolation group were mostly males without spouses, took time to move, had more depressive moods, and poorer subjective health status. The non-social isolated group had faster maximum walking speed. Low ego-resilience was newly identified as a factor associated with social isolation among older people, as were being male, having no spouse, and depressive symptoms. Mediation analysis revealed that ego-resilience affected social isolation and was partially mediated by depressive symptoms.
Introduction
Older people are prone to various psychosocial problems, in addition to a decline in physical function due to aging. In Japan, where the birthrate is declining and the population is aging, social isolation among older people is a major problem. Social isolation is defined as the complete or near-complete absence of social contact (Perissinotto et al., 2019) or participation in social groups. According to a recent meta-analysis, social isolation was reported in approximately 25% of older adults (Teo et al., 2023). Social isolation among older people in Japan is serious and increasing compared to that in other countries (Tsuji et al., 2020). Social isolation is more likely to occur among older people owing to the complex effects of physical or psychological factors, such hearing loss, depression, dementia, and frailty, as well as social factors such as educational history, economic status, marital status, and smoking habits (Iliffe et al., 2007; Merchant et al., 2020; Wen et al., 2023; Zhao & Si, 2021). Social isolation has been linked to various health problems and is a risk factor for increased mortality (Holt-Lunstad et al., 2015), various conditions such as hypertension (Grant et al., 2009), cardiovascular disease (Valtorta et al., 2016), and stress (Kubo et al., 2021). Preventing social isolation among older adults can be rephrased as activating interactions among them. Recently, the usefulness of digital tools was reported (Peng & Roth, 2022; Sakurai, Nemoto et al., 2021) to expand social interactions among older adults. However, these studies did not consider the communication skills of older people.
In general, healthy living requires the ability to adapt flexibly to changes in interpersonal interactions, the environment, and circumstances in daily life. Ego-resilience, one such ability, is defined as an individual’s ability to adapt and ego-regulate in various environments in a resilient and flexible manner (J. Block & Kremen, 1996).
Ego-resilience is a biologically or genetically supported personality trait (Davidson, 2001). Childhood nurturing experiences can contribute to ego-resilience (Lee & Lee, 2019; Zhou et al., 2023). A previous study reported that psychological first aid intervention, which included relaxation or cognitive behavioral therapy, could potentially improve ego-resilience in adulthood (Eweida et al., 2023).
Ego-resilience is associated with happiness (Fastame et al., 2022), satisfaction (Goryczka et al., 2022), and reduced social anxiety (Seo et al., 2022). When ego-resilience is high, people are flexible (Tugade & Fredrickson, 2004), which is characterized by positive emotions which are believed to induce more acceptable behaviors (Kahn & Isen, 1993). Therefore, we hypothesized that ego-resilience in older people is related to social isolation. To examine our hypothesis, we investigated the effects of multiple factors related to social isolation.
Methods
Participants
The participants were 622 older people who lived in urban centers and had participated in the “Otassha Study in 2022,” and who gave written consent to cooperate in the survey. “The Otassha Study” was a health promotion program for those aged 65 years or older who lived in Itabashi Ward, Tokyo (Fujiwara et al., 2013). Of the participants, 35 with Mini-Mental State Examination (MMSE) (Folstein et al., 1975) scores below the cutoff value of 23 (Sakurai, Kim et al., 2021) were excluded due to concerns regarding the impact of cognitive decline on test accuracy. Additionally, 77 participants with unmeasured scores were excluded. Hence, 510 participants were included.
Measures
Considering previous studies (Merchant et al., 2020; Wen et al., 2023; Zhao & Si, 2021), information related to social isolation was collected. Participants’ basic attributes included age, sex, educational background, smoking history, and marital status. Physical function, grip strength, maximum walking speed, and skeletal muscle mass index (SMI) were measured as parameters associated with potential sarcopenia (Chen et al., 2014) and frailty (Satake et al., 2017). The Timed Up and Go Test (TUG) was also used to measure the risk of falling (Shumway-Cook et al., 1997). Grip strength and body composition were measured with a Smedley grip strength meter and body composition analyzer (InBody770, InBody), respectively. Additionally, maximum walking speed was measured. The TUG was performed with a stopwatch. Hearing was evaluated as normal if the answer was “normal” to the question: “Can you hear normally?” A Japanese version of the GDS-15 (Niino et al., 1991), a shortened version of the Geriatric Depression Scale (GDS) (Yesavage et al., 1982) frequently used to evaluate depressed mood in old age, was used to assess mental status. Its reliability and validity have been confirmed. Respondents answered ‘Yes” or “No” for the 15 items. One point was added when the answer was “yes,” and the total score ranged from 0–15. Higher scores indicated more depressive symptoms. Self-reported health status was obtained with reference to a previous study (Zhao & Si, 2021). Participants were asked, “Do you consider yourself healthy in general?” Responses ranged from “very much so,” “fairly healthy,” “not so healthy,” and “not healthy.” Each response was given a score of 1, 2, 3, or 4, and added as a covariate.
Social isolation was assessed via the Lubben Social Network Scale-6 (LSNS-6) (Lubben et al., 2006). The LSNS-6 consisted of six items, three each related to family networks and non-family networks. Items were rated on a 5 point Likert scale (0 = nobody, 5 = nine or more). The Japanese version of the LSNS-6 was confirmed to be reliable and valid (Kurimoto et al., 2011). In this study, social isolation was defined as a score of <12 points, which was the cutoff value.
Ego-resiliency was assessed via the ego-resiliency scale (J. Block & Kremen, 1996), which consists of one factor and 14 items. Responses were rated on a 4-point Likert scale (1 = not at all true to 4 = very true). The Japanese version was confirmed to be reliable and valid (Hata & Onodera, 2013). Higher scores indicated higher adaptive ability in stressful situations (J. Block & Kremen, 1996).
Statistical Analysis
The participants were divided into socially isolated and non-socially isolated groups. First, chi-squared and Mann-Whitney U tests were used to compare demographic profiles between the two groups and each assessment item. Additionally, we extracted factors associated with social isolation via a logistic regression analysis. Social isolation and variables that showed significant differences or trends were used as the objective and explanatory variables, respectively. In addition, a mediation analysis was conducted to examine the pathways of ego-resiliency and social isolation. IBM SPSS Statistics version 29 (IBM, Armonk, NY, USA) was used for statistical analysis. The significance level was set at less than 5% and less than 10% was considered a significant trend.
Results
Participants’ Characteristics
Participants’ ages ranged from 65 to 92 years (mean: 72.8 ± 6.2 years). Among the participants, 311 were women. In total, 156 participants were defined as socially isolated based on their LSNS-6 score.
Table 1 presents the demographic comparisons between the social isolation and non-social isolation groups. The social isolation group had a significantly lower median ego-resiliency scale score (42.0) compared to the non-social isolation group (38.0). The social isolation group was more likely to be male and have no spouse. In the physical assessment, the social isolation group tended to have a longer TUG time. Meanwhile, the non-social isolation group tended to have a faster walking speed. In the psychological assessment, the social isolation group had higher depressive moods and reported poorer subjective health status.
Comparison of Participants’ Characteristics With and Without Social Isolation (n = 510).

Note. LSNS-6 = Lubben Social Network Scale-6; GDS-15 = Geriatric Depression Scale-15
Analysis of Factors Associated With Social Isolation
Table 2 presents the results of the logistic regression analysis. Being male, not having a spouse, depressive symptoms, and low ego resilience were identified as independent factors associated with social isolation. No multi-collinearity was observed among the covariates.
Multivariate Logistic Regression Analysis of Social Isolation (n = 510).

A mediation analysis was conducted to examine the mediating effects of depressive symptoms. Figure 1 presents the mediating role of depressive symptoms in the relationship between ego-resiliency and social isolation. Standardized coefficients from ego-resiliency to GDS (−0.37), GDS to LSNS-6 (−0.32), and ego-resiliency to standardized coefficient from GDS to LSNS-6 (0.30) were all significant. In addition, the standardized coefficient for the indirect effect of the GDS (0.12) was also significant, which indicated partial mediation of the GDS in the relationship between ego-resiliency and LSNS-6 (bootstrap sample = 2000, 95% CI [ 0.07, 0.14]).
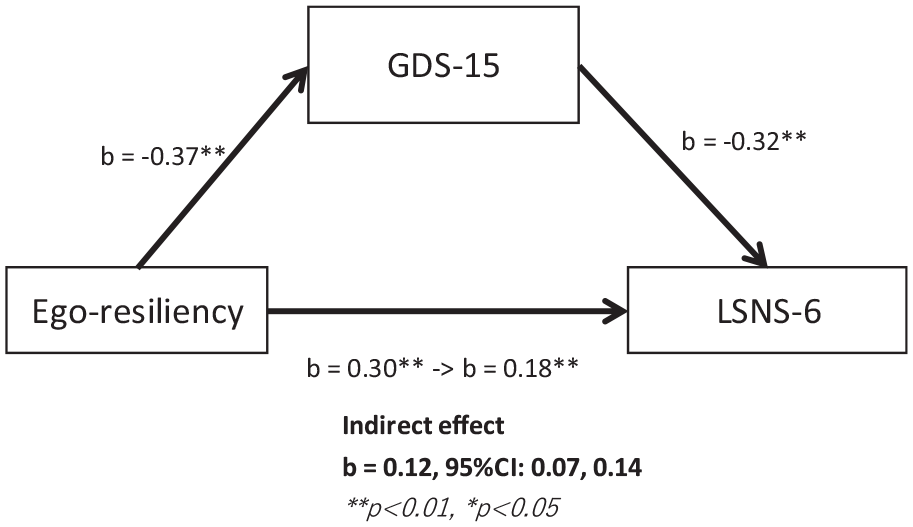
Path diagram of the mediation analysis of depressive symptoms on the relationship between ego-resiliency and social isolation.
Discussion
Ego-resilience was identified as an independent factor associated with social isolation among older urban residents.
High ego-resilience is associated with high extraversion (Paulhus & Martin, 1987). Extraversion is a characteristic mediated by social support and enhanced well-being (Zhu et al., 2013). Therefore, high ego-resilience may reflect the ability to construct interpersonal relationships that are more likely to receive social support. Hence, it may be the ability to adapt flexibly to ambiguity in interpersonal relationships (J. Block & Kremen, 1996).
Ego-resilience is fostered by repeated flexible and adaptive interactions in secure attachment relationships during childhood (J. H. Block & Block, 1980). Furthermore, positive emotions may enhance ego-resilience (J. Block & Kremen, 1996). Positive emotional impulses such as children’s play, contribute to the construction of social resources (Fredrickson, 2001) and are considered an important basis for ego-resilience. This is similar to the status of free children in transactional analyses and is not necessarily limited to childhood.
Depressive symptoms may lead to low motivation and pessimistic thinking, which may affect interpersonal interactions. According to transactional analysis, when depressive symptoms are strong, the critical parent and adapted child act despite low psychological energy (Dusay, 1977). People with depressive symptoms tend to avoid interaction with close relatives, even though it has a positive effect on their medical condition (Brown et al., 2011). Depressive symptoms may lead to a negatively biased interpretation of facial expressions (Bourke et al., 2010), which may transmit negative moods to those with whom the individual interacts (Joiner & Katz, 1999). Therefore, depressive symptoms decrease sociability which causes psychological distress (Elmer & Stadtfeld, 2020; Kawachi & Berkman, 2001) which, in turn, increases depression in a reciprocal relationship. Hence, the stagnation of social interaction due to depressive symptoms plays a significant role in the formation of social isolation.
Results of the mediation analysis showed a partial mediation of depressive symptoms as an indirect effect on the relationship between ego-resiliency and social isolation. Therefore, high ego-resiliency directly influenced social isolation when associated with depressive symptoms. Combined with evidence that older adults’ capacity for adversity and depression are important factors for subjectively determined successful aging (Jeste et al., 2013), depressive symptoms and high ego-resilience are likely particularly important factors in the bio-psychosocial model. These results also support the findings of a previous study (MacLeod et al., 2016) that higher resilience in older adults is associated with lower depression.
Considering these results from a public health perspective, we believe there are two important aspects of measuring ego-resiliency among community older adults. First, older people with low ego-resiliency are at risk for increased depressive symptoms in addition to social isolation. Hence, identifying individuals at risk is important from a preventive medicine perspective. Furthermore, since ego-resiliency is associated with extraversion and happiness, improving it may at least facilitate good interactions in society. Inclusion of sessions designed to improve ego-resiliency in group work in the community might be an important public health practice to address the risk of social isolation. Furthermore, it may be important for older people to understand their own ego-resiliency as internal state to activate their interactions. Therefore, among older people, understanding their own ego-resiliency could enable them to reflect on their interaction activities. This may help them identify areas for improvement in their relationships with others and contribute to the prevention of social isolation.
Additionally, we observed an association between the male sex and social isolation. Previous studies on social isolation among older people in Japan and the UK reported that men were associated with social isolation. Furthermore, activating interactions with family members was important for Japanese people and friends in the UK (Saito et al., 2021). Similarly, a study on Koreans in the US considered vulnerability regarding interactions with family and friends among men as a factor of social isolation (Jang et al., 2016). These results are consistent with those of the present study. Furthermore, social isolation was promoted among men when interactions with close relatives was interrupted. A cohort study on older adults’ activities of daily living (ADL) reported that men who had less interaction with their families showed a more pronounced decline in ADL than women (Seeman et al., 1996). In addition to being more likely to experience social isolation, older men may also experience adverse health effects due to social isolation.
In the present study, marital status was an important factor related to social isolation. Presence of a spouse implied at least one social connection, a protective factor. Furthermore, since older adults tend to maintain their social networks by focusing on a small number of intimate relationships to meet their emotional needs (Carstensen, 1992), spousal presence may have a greater influence than in younger adults.
In contrast, physical function and self-reported health status were not associated with social isolation. According to a 20-year follow-up study (Viljanen et al., 2023), successful older adults had higher life satisfaction, even if their physical and subjective health status declined, which was related to higher resilience. Although physical function and self-reported health status were lower in the social isolation group, the results of the logistic regression analysis identified just ego resilience as an associated factor for social isolation, which generally supported the results of previous studies (Viljanen et al., 2023).
We found, however, that mental health was more closely associated with social isolation, which suggests that the effect of physical health on social isolation may be mediated by mental health. There is no unified international view on the causal relationship between mental health and physical health. Previous studies have differing opinions. Some believed that physical health was defined by mental health (Heidrich, 1994; Levine et al., 2021; Pembroke et al., 2006). Others found strong indirect cross-effects in both mental and physical health (Ohrnberger et al., 2017). Our analysis did not extract physical health as an associated factor for social isolation, which suggested that maintenance of good mental health could be a more important factor to prevent social isolation.
This study was the first to identify a link between social isolation and ego-resilience among older adults, a social problem of international importance. However, this study has several limitations. First, although this study was conducted on older people in urban centers, participants’ attributes may have influenced the results. Our sample may have included a larger percentage of participants with higher physical functioning than typical older people. Therefore, conducting a similar study over a wider area is necessary.
Second, this study used several established questionnaires to assess participants’ psychosocial aspects. However, we did not examine the possibility of similar aspects among the items in the questionnaires. Furthermore, we cannot ignore the influence of latent factors not measured in this study. For example, the observed phenomenon might be linked to specific characteristics of older people (e.g., pessimism or economic conditions) that may synchronously lead to inability to cope flexibly with various challenges and a higher likelihood of social isolation. Hence, full generalizability cannot be assumed. These limitations would be resolved by selecting a suitable instrumental variable or employing artificial intelligence in the future studies.
Conclusion
Higher ego-resilience affected social isolation independent of related factors, such as the male sex, depression, and marital status, among older urban people.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214241238069 – Supplemental material for Association Between Ego-Resilience and Social Isolation Among Urban Older People
Supplemental material, sj-docx-1-ggm-10.1177_23337214241238069 for Association Between Ego-Resilience and Social Isolation Among Urban Older People by Kazuaki Hashimoto, Takeaki Takeuchi, Kazushige Ihara, Shuichi Obuchi, Hisashi Kawai, Hirohiko Hirano, Yoshinori Fujiwara, Kim Hunkyung, Yutaka Watanabe and Masahiro Hashizume in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Declarations
This study was conducted in accordance with the Declaration of Helsinki and its future amendments. This study was approved by the Ethics Committee of the Tokyo Metropolitan Institute of Gerontology (protocol code R22-034, 2022).
Informed Consent
Written informed consent was obtained from all participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.