
Abstract
Keywords
Introduction
Practice or retest effects are well-recognized phenomena in psychological and/or neurocognitive testing (Almkvist & Graff, 2022; Gross et al., 2015; Jendryczko et al., 2019; Machulda et al., 2013). Practice effects have been reported in healthy adults when test and retest were administered 1 day apart (Collie et al., 2003), or were separated by intervals ranging from 2 to 3 weeks up to 1 year (Bartels et al., 2010). Cooper et al. (2004) reported statistically significant practice effects in cognitively healthy older subjects. However, the possibility that healthy aging might cause divergent practice effects in different cognitive domains remains unresolved.
Practice effects on assessments of cognitive function or performance may be attributable to both procedural memory and content familiarity when testing is repeated using the same protocols and materials. Procedural familiarity likely reduces anxiety during cognitive challenges or mental stress (Gross et al., 2018) and may contribute to the improved cognitive performance during retesting. Furthermore, procedural and/or content familiarity may attenuate the cardiorespiratory responses to mental stress during cognitive retesting. However, whether cognitive test-retest assessments may differentially affect mental stress or anxiety related physiological responses in healthy adults of different ages is unclear.
This study examined the effects of age on cardiac (heart rate) and respiratory (breathing frequency) responses to mental stress during cognitive test and retest challenges, and on test-retest practice effects in different cognitive domains using Mini-Mental State Examination (MMSE) for testing global cognition, Trail Making Test – B version (TMT-B) for testing attention, executive function and coordinated visual-motor processing speed, Digit-Span Test (DST) with forward and backward recalls, and California Verbal Learning Test—2nd edition (CVLT-II). In geriatric practice and/or neurocognitive research, short-term memory is commonly assessed using DST or digital-verbal memory (Jones & Macken, 2015; Monaco et al., 2013) and CVLT-II or word-verbal memory tests (Casaletto et al., 2017; Elwood, 1995; Woods et al., 2006). The question remained if a practice effect might have different impacts on these two different memory modalities.
It has been reported that aging attenuates increases in heart rate and breathing frequency during physiological challenges, for example, postural transition from supine to standing (Stanley et al., 1997) or exposure to hypoxic air (Liu et al., 2020). However, the heart rate response to mental stress reportedly was not affected by age (Uchino et al., 1999) or attenuated in older subjects (Barnes et al., 1982; Gintner et al., 1986). Since aging is associated with reduced cardiac beta-adrenergic responsiveness (White et al., 1994) and diminished vagal modulation (Shi et al., 2000), we hypothesized that the increases in heart rate and breathing frequency associated with cognitive testing are attenuated in older adults, and that the aging-associated diminution of the practice effect will in turn lessen the impact of cognitive retesting on those physiological responses.
Methods
Participants
Ten cognitively healthy older (65 ± 2 years old: four men, six women) and 11 younger (26 ± 1 years old: five men, six women) adults participated in the study after signing a written consent and completing a medical/health questionnaire. The sample size of ≥10 per group was estimated based on the previously reported, adequately powered studies (Liu et al., 2020; Shi et al., 2000). The study protocols were approved by the North Texas Regional Institutional Review Board for Protection of Human Subjects. There were no significant age-related differences in body weight (older vs. younger subjects: 73.0 ± 5.7 vs. 69.6 ± 2.7 kg), height (1.70 ± 0.03 vs. 1.72 ± 0.02 m), or body mass index (25.1 ± 1.2 vs. 23.5 ± 0.8 kg/m2). Most of the subjects had completed two or more years of college (older vs. younger subjects: 16.7 ± 0.8 vs. 16.6 ± 0.2 years of education). The older group included 1 Black, 1 Hispanic/Latino, and 8 White subjects, whereas the younger group included 4 Asian, 1 Black, 1 Hispanic/Latino, and 5 White subjects. Persons with uncontrolled chronic conditions including hypertension (systolic/diastolic pressures >140/90 mmHg with medications), diabetes with insulin medication, chronic renal failure, nephritis, or congenital heart disease; those with acute conditions such as recurrent chest pain, seizures or epilepsies; those with asthma, allergic rhinitis, lung fibrosis, emphysema or tumor/cancer; or who had myocardial ischemia or infarct, second or third degree atrio-ventricular conduction blockade on electrocardiogram were excluded from the study. Also excluded were subjects with hemorrhagic stroke, traumatic brain injury, infectious disease, psychologic disorder or neurologic dysfunction, or who had been diagnosed with mild cognitive impairment with MMSE score ≤26. Eligible subjects ages 18 to 38 and 56 to 76 years were assigned to the younger and older groups, respectively. Wearing glasses was permitted during cognitive test-retest. No subject used a hearing aid.
Procedures
To assess the impact of healthy aging on cardiorespiratory responses associated with the test-retest practice effects, cognitively normal younger and older adult subjects underwent two sessions of cognitive testing, 3 weeks apart. It has been reported that practice effects in cognitive assessment were present after a 1-week interval between test and retest (Duff et al., 2008), but after a 1-month interval, the practice effects had subsided in cognitively healthy adults (Falleti et al., 2006). We hypothesized that cognitive assessment practice effects would subside within 3 weeks in cognitively healthy older adults, but not in young adults of similar educational attainment. Before and after cognitive testing, arterial oxygen saturation (SaO2), hemoglobin content (Hb), systolic and diastolic blood pressures and pulse were measured by standard techniques of our laboratory. Heart rate (HR) and breathing frequency (BF) were continuously monitored during the pretest baseline and throughout MMSE, TMT-B, and DST.
Measurements
Cognitive assessment MMSE (PAR®, Lutz, FL) was applied to assess global cognition. Times to completion of TMT-B was recorded to assess attention, executive function and coordinated visual-motor processing speed. Correct recall numbers of DST-Forward and DST-Backward (WAIS®-IV PEARSON, Bloomington, MN) were documented to assess digit-verbal memory. Each sub-test began with two numbers and each subject undertook two attempts per span. Spans increased by 1 digit with 8 increments for DST-Forward and 7 increments for DST-Backward. Maximal score was 16 points for each DST sub-test (i.e., two points per pair of spans ×8 pairs). Accurate recall of the terms in four trials of immediate, short-delayed (30-sec) and long-delayed (10-min) free recall of CVLT-II (Short-Form, PEARSON, Bloomington, MN) were documented to assess learning ability and word-verbal memory. A perfect score was nine words in the immediate, short-delayed and long-delayed free recall sub-categories. These cognitive assessments were applied in our previous clinical study (Wang et al., 2020).
Cardiorespiratory variables were measured as described in our previous reports (Liu et al., 2017, 2020). Arterial pressures were measured using a Welch-Allyn PROPAQ® CS Vital Signs Monitor (San Diego, CA). Standard lead II electrocardiography (BIOPAC ECG100C) and abdominal plethysmography for BF (BIOPAC RSP100C) were continuously recorded on a laptop computer interfaced with a BIOPAC SYSTEMS MP150 (Santa Barbara, CA) data acquisition system. Continuous stable segments (~30 s) of heart rate and breathing frequency data during MMSE, TMT-B, and DST assessments were selected and averaged to represent the responses to these cognitive challenges. This approach to analyze continuously monitored cardiorespiratory measurements has been reported previously (Liu et al., 2017, 2020; Wang et al., 2020; Zhang et al., 2010, 2014; Zhao et al., 2022).
Data Analysis
Data were analyzed with Statistical Analysis System (SAS) software (Version 9.4, Cary, NC). The SAS t-test procedure was applied to compare the weight, height, and years of education for two independent age groups. Two-factor ANOVA was applied to test the significance of the age factor (older vs. younger subjects) and the test-retest factor (first vs. second visits) on the difference in the age groups (age factor) between the test (first visit) and retest (second visit) cognitive performances (retest factor). Three-factor ANOVA was applied to evaluate the differences in HR and BF responses before (i.e., pretest baseline) and during cognitive testing (mental stress factor) between the test-retest performances (retest factor) in the older versus younger subjects (age factor). Tukey’s Honestly Significant Difference Test was conducted post hoc if the main factor showed statistical significance. p values < .05 were taken to indicate statistically significant effects. All data are reported as group mean values ± standard error of the mean (SEM).
Results
Resting systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and heart rate (HR) did not differ significantly before versus after cognitive testing (time factor p = n.s.) during either the first or second visit, indicating that cardiovascular function returned to baseline after the cognitive challenges (Table 1).
Blood Pressure and Heart Rate at Rest and After Each Cognitive Testing Visit.

Note. Values (mean ± SEM) were obtained before and after (time factor) the cognitive challenges during the first and second testing sessions (retest factor) in the younger and older adults (age factor). Non-significant p values between the age groups (age factor) or before versus after (time factor) suggests there is no-age related difference in the resting variables or a complete recovery after the cognitive challenges. SBP = systolic blood pressure; DBP = diastolic blood pressure; MAP = mean arterial pressure; HR = heart rate.
p < .05 versus first visit at the same time.
Both older and younger adults performed the MMSE, CVLT-II, and DST similarly well (Table 2), although the older subjects took longer to complete the TMT-B test (age factor p = .044). The test-retest MMSE, TMT-B, and DST performances were statistically similar between the first and second visits (retest factor p = n.s.). However, CVLT-II scores improved in the second versus the first visit, with retest factor p values of .016 and .002 for short-delay and long-delay free-recall, respectively. In contrast, post-hoc analysis indicated that the test-retest difference between the first and second visits did not attain statistical significance for short- (p = .193) or long-delay free-recall (p = .091) in the older adults, while the younger adults showed a significant practice effect (Table 2).
Cognitive Performance of Older and Younger Adults During the First and Second Visits.
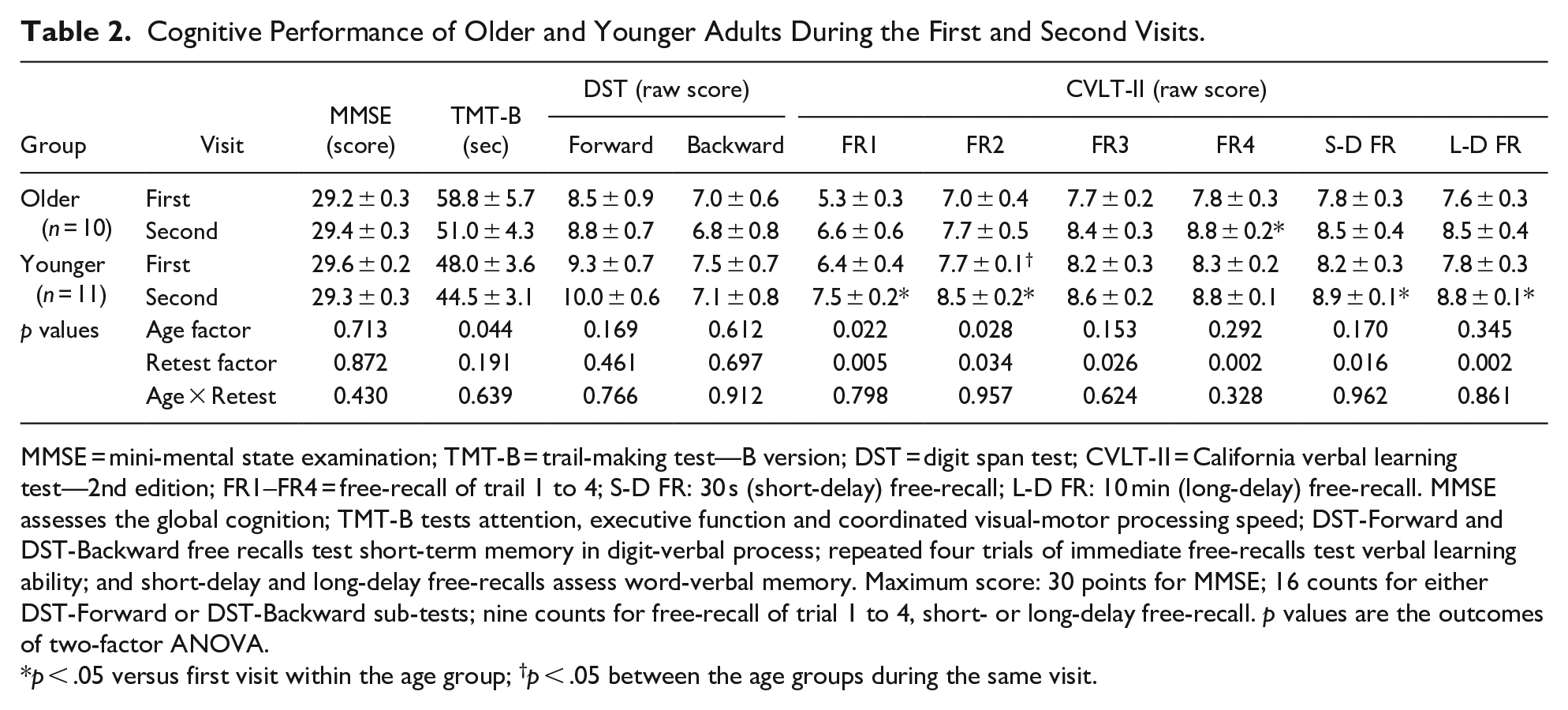
MMSE = mini-mental state examination; TMT-B = trail-making test—B version; DST = digit span test; CVLT-II = California verbal learning test—2nd edition; FR1–FR4 = free-recall of trail 1 to 4; S-D FR: 30 s (short-delay) free-recall; L-D FR: 10 min (long-delay) free-recall. MMSE assesses the global cognition; TMT-B tests attention, executive function and coordinated visual-motor processing speed; DST-Forward and DST-Backward free recalls test short-term memory in digit-verbal process; repeated four trials of immediate free-recalls test verbal learning ability; and short-delay and long-delay free-recalls assess word-verbal memory. Maximum score: 30 points for MMSE; 16 counts for either DST-Forward or DST-Backward sub-tests; nine counts for free-recall of trial 1 to 4, short- or long-delay free-recall. p values are the outcomes of two-factor ANOVA.
p < .05 versus first visit within the age group; †p < .05 between the age groups during the same visit.
Figure 1 presents four individual CVLT-II trials of immediate free-recall performance (panel A) and the sum of the trials (panel B) during the first and second visits for the older and younger adults. Immediate free-recall performance progressively improved over the four trials (trial factor p < .001, Figure 1A), indicating a significant learning ability or practice effect during the first visit. From trial 2 onward, all of the immediate free-recall trial scores exceeded (p < .05) the trial 1 scores in both younger and older subjects during both visits. However, there was a significant age factor on both trial 1 (p = .022) and trial 2 (p = .028) scores, and the trial 2 score during the first visit was significantly lower in the older than younger subjects (Table 1), indicating an age-related declined learning ability in verbal learning recall. The overall performance of CVLT-II immediate free-recall was significantly better in the secondversus first visit in terms of the individual trials (trial factor p < .001) or the sum of the trial scores (trial factor p = .001). However, post hoc analysis revealed that this practice effect was statistically significant only in the younger group (Figure 1B), while in the older group the test-retest difference between visits 1 and 2 revealed a marginally significant trend (trial factor p = .055). With stratification of the visits, the scores of total free recalls were significantly different between the age groups during the first (p = .034) but not the second visit (p = .256). The younger subjects outperformed their older counterparts in both the individual immediate free-recall trials (age factor p < .001) and the sum of the trial scores (age factor p = .021) (Figure 1). Post hoc analysis of the four immediate free-recall trials with stratification of the visits revealed only marginal differences between the two age groups in the first (p = .054) and second (p = .069) trials during the first visit.

Four individual trials of 9-word immediate free-recall (A) and the sum of the 4 trial scores (B) during the first and second visits in young and older adults with healthy cognition. Panel A: 9-word immediate free-recall (circles: first session; triangles: second session) in younger (open symbols) and older (filled symbols) adults. Three-factor ANOVA: Immediate free recall scores are greater in the younger than older subjects (age factor p < .001) and increased when the trials were repeated (trial factor p < .001) during the second visit (retest factor p < .001). Post-hoc analysis shows that from trial 2 onward, all immediate free-recall performance scores were significantly increased (p < .05) versus the respective trial 1 scores in both groups during both visits. Panel B: The sum of 4-trial immediate free-recall performance was significantly affected by both the age and retest factors of two-factor ANOVA, indicating an age-related difference in verbal learning ability and practice effect on test-retest performance in the four trials of free-recalls during CVLT-II. p values are from post-hoc analysis.
In the younger adults, the cognitive performance related mental challenges during MMSE, TMT-B, and DST increased both HR (Figure 2A; stress factor p = .003) and BF (Figure 2B; stress factor p = .005). Also in the younger subjects, physiological responses to mental stress were significantly attenuated during the second visit (retest factor p < .001 for both HR and BF), indicating a practice or retest effect that reduced the testing-related mental stress. In contrast, HR in the older subjects was essentially unchanged from the baseline during MMSE, TMT-B and DST, either during the first or second visit (Figure 2A). Consequently, there was a significant age-related difference in HR responses to mental stress (age factor p < .001): in the younger subjects, marked increases in HR during MMSE, TMT-B and DST on the first visit were sharply attenuated during the second visit, but in the older subjects, none of the tests significantly affected HR during either visit (Figures 2A and 3A–C). Age had no appreciable impact on the BF response or practice effects (age factor p = .651), although the retest factor attained statistical significance in the older adults during MMSE (Figure 3D).

Heart rate (A) and breathing frequency (B) at rest and during mini-mental state examination, trail-making test and digit-span test. Panel A: Three-factor ANOVA revealed increased heart rate during cognitive testing-related mental stress (stress factor p = .003) in the younger but not older adults (age factor p < .001) and decreased stress effect during the second visit (retest factor p < .001). Panel B: Breathing frequency increased during cognitive testing (mental stress factor p = .005), but this effect diminished during the second visit (retest factor p < .001). The breathing frequency responses to the cognitive challenges were similar in the two groups (age factor p = .650).

Relationships of cognitive test scores versus heart rate (A–C) and breathing frequency (D–F) during test-retest of mini-mental state examination (MMSE), trail-making test (TMT-B) and digit-span test (DST). Panels A–C: heart rate was significantly higher in the younger than older subjects during the first testing session in different cognitive domains. Furthermore, the differences in heart rate between the first and second sessions (retest practice effect) was attenuated in the older adults. Panels D–F: there were no age-related differences in breathing frequency during the three tests. The retest factor on breathing frequency was present. However, the cognitive retest effect on breathing frequency was attenuated in the older subjects, except during MMSE.
Discussion
This study assessed, for the first time, the effect of healthy aging on cognitive testing familiarity effects and the associated cardiorespiratory responses to test-retest cognitive challenges. There was no evidence of practice effect on MMSE, TMT-B, and DST in the cognitively normal older and younger adults. CVLT-II immediate free-recall test performance improved in the second testing session in both age groups. Thus, retesting familiarity effects were limited to the word-verbal memory free-recall test and, not the digit-verbal memory free-recall test. The absence of statistically significant age factors on MMSE, DST-Forward, DST-Backward, or CVLT-II 30-sec short-delay and 10-min long-delay free-recall scores suggested that overall cognitive function and/or short-term memory seemed was not appreciably affected by healthy aging. However, verbal learning ability showed a declining trend with healthy aging.
Cardiorespiratory stress responses to cognitive testing and retesting diverged in the younger versus older adults. Although heart rate and breathing frequency increased during the first round of cognitive testing of the younger adults, the breathing frequency response was diminished and the heart rate response essentially absent in the older adults. The cardiorespiratory responses in the younger subjects were attenuated during retesting 3 weeks later. In contrast, in the older adults there were no appreciable test-retest effects on heart rate, which remained near baseline throughout both visits. Although breathing frequency fell by ~1.5 breaths/min during the second MMSE administration in older adults, it was unaltered in the secondversus first TMT-B and DST. Thus, practice effects attenuated cardiorespiratory responses to cognitive testing in younger adults, but less appreciably in their older counterparts.
The test-retest performances in MMSE and DST did not differ between the cognitively intact older and younger subjects (Table 2). The initial MMSE scores were near the maximum value of 30 points in both groups, severely limiting a potential practice effect. However, performance on the DST was only about 50% to 70% of the maximum in both age groups (Table 2). The lack of significant improvement during the DST-Forward or DST-Backward free-recalls suggested that the ceiling factor alone cannot entirely account for the absence of a practice effect. Furthermore, TMT-B performance was slightly superior in the younger than older adults (age factor p = .044), yet the retest improvement factor was not significant (p = .191). Nonetheless, practice effects were evident in the word-verbal memory or CVLT-II performance, suggesting that practice effects may have varying impact in different cognitive domains. Word-verbal memory testing (CVLT-II) appeared to be more prone to practice effects than digital-verbal memory testing (Digit-Forward and DST-Backward) or visual-attention/executive function (TMT-B).
Duff et al. (2018) assessed in elderly adults (mean age 77.5 years) the test-retest effect on TMT A and B and Hopkins Verbal Learning Test—Revised (HVLT-R) with a 1-week interval between tests. They found that HVLT-R but not TMT was significantly improved during the retest performance, although performances on both tests correlated with bilateral hippocampal volumes (Duff et al., 2018). These findings are concordant with the present results, which revealed a significant retest factor in CVLT-II performance, but no practice effects on TMT-B and DST in either the older or younger subjects. However, improvements in the CVLT-II short-delay and long-delay free recall scores upon retesting attained statistical significance only in the younger subjects in the present study (Figure 1, Table 2). This divergence between the present study and that of Duff et al. in the retest short-term memory on verbal memory testing of older adults is probably due to the shorter (∼1 week) gap between test and retest in the study by Duff et al., whereas the practice effects may have largely subsided over the 3-week between-visit hiatus in the present study, especially in the older adults.
During cognitive testing, both heart rate and breathing frequency increased in the younger adults, but only breathing frequency increased in the older adults (Figure 2). Increases in heart rate were not statistically significant in the older adults during either the first or second rounds of cognitive testing. The heart rate and, to a lesser extent, the breathing frequency responses were attenuated during retesting with the same procedures and content (Figures 2 and 3). These cardiorespiratory responses suggested that practice effects reduced the mental burden of cognitive testing challenges and their associated physiological responses. Attenuation of cardiorespiratory responses could, in turn, help improve cognitive testing performance. Indeed, mental calming associated with slow deep breathing may improve memory-learning and cognitive performance (Jella & Shannahoff-Khalsa, 1993; Yadav & Mutha, 2016). However, in the present study there were no significant improvements in the retesting performance of MMSE, TMT-B or DST. Thus, the practice effects seemed to more effectively alleviate the mental burden than improve mentation or cognitive performance in cognitively healthy older and younger adults.
In this study, all subjects, regardless of age or cognitive function, showed progressive improvement in word-verbal memory with repeated trials during immediate free-recall performance (Figure 1, Table 2). Since significant improvement began in the second immediate free-recall trial, this acute practice effect or leaning ability likely resulted from growing familiarity with the testing procedure, content and materials over the testing session. However, the trial 2 scores during the first visit were significantly lower in the older than younger subjects, indicating a trend of the age-reduced learning ability (Table 2), despite the factor that short-term memory, as evident by DST-Backward and DST-Forward or 30-sec short-delay or 10-min long-delay free-recalls, was not significantly affected by healthy aging.
Study Implications and Limitations
Working memory training is known to improve cognitive function in older adults (Heinzel et al., 2014), which may be ascribed in part to training-associated familiarity in cognitive processing of testing procedure and materials. However, a single training session may not sufficiently engage working memory, especially in older adults. Practice effects may dampen augmentation of cardiorespiratory responses during cognitive testing. Studies with larger sample size and including assessments of blood flow responses to cognitive testing in different age groups with impaired or normal cognition are needed to define further the relationships between cognitive training effects and cardiorespiratory responses. Physiologically, mental challenges during cognitive testing may stimulate blood flows to muscle (Barcroft et al., 1960; Widegren et al., 2010), skin (Fencl et al., 1959) and brain (Shoemaker et al., 2019). Resting cardiac output (Guo et al., 2005), cerebral tissue oxygenation (Liu et al., 2020) and middle cerebral artery flow velocity (Liu et al., 2020) are lower in older than younger adults despite similar resting heart rates. It remains unclear whether the responses of these cardiovascular variables to mental challenge during cognitive testing vary in different age groups with normal or impaired cognition. Such physiological assessments may yield diagnostic insights into cognition- and/or age-related changes in neurovascular coupling.
This study utilized a 3-week interval between cognitive tests and was conducted in subjects who had completed on average 3 to 4 years of college education. Educational attainment reportedly correlates with cognitive function level (Wilson et al., 2009) and protects older adults from cognitive decline (Jester et al., 2023; Vigoureux et al., 2021; Wight et al., 2006). It is unclear if the present findings would emerge after shorter or more prolonged test-retest intervals, or if the subjects had represented broader ranges of formal education attainment.
Conclusions
Procedural familiarity practice effects seem to be more substantial in word-verbal recall than in digit-verbal recall or visual-attention/executive function in cognitively healthy adults. Cardiorespiratory responses to cognitive challenges are attenuated in young adults when the same testing procedures and materials are repeated after a 3-week interval, but these test-retest differences are limited in older adults. Thus, healthy aging may limit the practice effects on cognitive testing performance and the associated cardiorespiratory responses to cognitive testing, despite the absence of cognitive impairment. However, there was no age-related decline in overall cognition and short-term memory, despite a downward trend in learning ability associated with healthy aging.
Footnotes
Author Contributions
PMR, KA, and XS contributed to the study design, data collection, data analyses, and manuscript preparation; SER, SD, and RTM contributed to data interpretation and manuscript preparation. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by grant R01-AG076675 from National Institute on Aging.
Ethical Approval
The study protocols were approved by the North Texas Regional Institutional Review Board.
Data Availability Statement
The original data are available from the corresponding author upon request.