
Abstract
Improving relative strength is important for maintaining functionality with age, and outdoor exercise structures could be useful to facilitate this. A total of 29 adults aged 65+ participated in a non-randomized crossover study with a 6-week control followed by a 6-week resistance training intervention on an outdoor exercise structure (3x/week). Relative strength (predicted maximal leg press/lower body lean mass [Dual-energy X-ray Absorptiometry]) and physical function variables were measured at baseline, post-control, and post-intervention. Represented as median (25th–75th), lower body relative strength improved from 7.91 (7.01–9.35) post-control to 8.50 (7.99–9.72) post-intervention (p = .002) in study completers (n = 17). Maximum leg press (p = .002), 30-second chair stand (p < .001), one-leg stance (p = .011), and maximum chest press (p = .009) also improved significantly during the intervention. There were no significant changes in aerobic activity, grip strength, lean mass, or muscle power. This study demonstrates that there could be potential relative strength benefits associated with the use of outdoor exercise structures in older adults.
What this paper adds
Provides evidence for an exercise option for older adults that addresses several barriers to physical activity.
The first study to assess the impact of outdoor exercise structure use on relative muscle strength in older adults.
While outdoor exercise structures are often promoted as an accessible option for physical activity and exercise, our results suggest that these structures may not be well suited for all populations, hence the dropout rate.
Applications of study findings:
Encourages the use of outdoor exercise structures for older adults in community settings.
Can be used to compel policy decision-makers and municipalities to invest in outdoor exercise structures to improve the health and wellbeing of older adults living in the community.
Highlights the need for more research regarding which populations outdoor exercise structures may be most appropriate for.
Introduction
After the age of 50, muscle mass and muscle strength decrease at a rate of 10% and 12% to 15% per decade, respectively (Doherty, 2001; Goodpaster et al., 2006). This marked loss of muscle mass and muscle strength in older adults can lead to a significant decline in physical function and eventually a loss of independence (Luppa et al., 2010). While both muscle mass and muscle strength are significantly associated with physical function in older adults, it is unclear whether one is more important than the other. However, an emerging area of research suggests that the relationship between muscle mass and muscle strength may be more important than either one independently (Radaelli et al., 2021). This is often referred to as relative strength and is depicted as a ratio between the amount of force that an individual can produce per unit of muscle mass (Radaelli et al., 2021).
One of the most efficient interventions for slowing and reversing the decline in muscle mass and muscle strength with age is resistance training (Izquierdo et al., 2021). A minimum of two resistance training sessions per week is recommended to maintain and improve health-related outcomes such as strength, balance, and physical function (El-Kotob et al., 2020). However, 67.5% of older adults report not taking part in any resistance training activities (Copeland et al., 2019). In an attempt to address the many barriers to resistance training for older adults such as cost and lack of access to exercise facilities (Cavill & Foster, 2018), municipalities worldwide have been installing outdoor exercise structures.
Outdoor exercise structures are collections of outdoor equipment that are installed to promote physical activity (Jansson et al., 2019; Lee et al., 2018). They often resemble playground equipment and are versatile pieces of equipment that can be used to perform a variety of exercises targeting strength, balance, and aerobic fitness. They are free to use, available anytime, often installed in residential areas, and usually provide instruction on proper use. Despite increased installations, usage uptake by older adults has remained low, making up only 3% to 14% of users (Cohen et al., 2012; Mora, 2012). Before attempting strategies to promote the usage of these structures, it is important to test the efficacy of using these structures to improve relative strength, functional outcomes, and overall health.
Previous research shows that outdoor exercise structures may be beneficial for increasing levels of physical activity within communities, but the potential to improve health or functional outcomes is unclear (Jansson et al., 2019). The main objective of this study was to assess whether performing resistance training on an outdoor exercise structure for 6 weeks can improve lower-body relative strength in adults aged 65 and above. The secondary objectives were to explore any functional benefits of using an outdoor exercise structure over 6 weeks and to assess any potential differences in characteristics between completers and non-completers.
Methods
Design
This study used a non-randomized crossover design where participants first completed a 6-week non-exposure control period and subsequently participated in a 6-week resistance training intervention. Data collection occurred at baseline, 6 weeks (post-control), and 12 weeks (post-intervention). Before the study began, research ethics approval was obtained for this project.
Participants
Participants were recruited in a city of ~70,000 people via virtual flyers on social media outlets such as Facebook, and physical flyers placed around the community. To be eligible for this study, participants had to be over the age of 65, living in a community setting, not currently resistance training, be able to grip objects in day-to-day life (self-reported), and be cleared to exercise using the Get Active Questionnaire (Canadian Society of Exercise Physiology, 2017). Exclusion criteria included any uncontrolled medical conditions, current musculoskeletal injuries, and any vacation lasting more than 1 week during the intervention. All participants received and signed an informed consent form to ensure they understood the entirety of the research project, along with its associated risks and benefits.
To determine the appropriate sample size to test the main hypothesis, expected effect size and variation on lower-body relative strength (1.03 ± 0.825) were calculated from a previous study (Fragala et al., 2014). Based on these values and accounting for 25% attrition as reported by previous studies (Cyarto et al., 2006), using a power of 80% and an alpha of .05, the aim was to recruit 28 participants with an equal number of males and females.
Intervention
During the intervention, participants met at an outdoor exercise structure located centrally three times per week for 6 consecutive weeks. The outdoor exercise structure used in this study was comprised of mostly horizontal and vertical metal beams rather than conventional workout machines and can be seen in the online-only Supplemental Material. All sessions were supervised by a certified exercise professional from 10:00 AM until 2:00 PM every Monday, Wednesday, and Friday, and participants were instructed to come within this time to complete their workout session. As a result, participants either exercised in small groups or on their own. Each session lasted approximately 45 min and consisted of a warm-up (~10 min), a resistance training regime (~30 min), and a cool-down (~5 min). Since the exercise program occurred three times per week for 6 weeks, the goal was to have each participant complete all 18 sessions before performing the post-intervention testing. Make-up sessions were offered for 2 weeks following the initial 6-week program to allow participants to complete all sessions in case any were missed due to inclement weather or personal reasons.
The resistance training program was developed using the American College of Sports Medicine’s recommendations and Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association (Fragala et al., 2019). Participants were given eight exercises focusing on all major muscle groups, but individual modifications were made to accommodate various abilities and conditions. Each session consisted of at least one exercise for each major muscle group, including the chest, back, arms, and legs, and all exercises used body weight as a source of resistance. The intensity of the exercises was tailored for each participant to follow the training principle of individualization and to ensure the same relative intensity for all participants. To do so, each prescribed exercise included four progressions ranging from least to most difficult to guide participants as needed. A table of the prescribed exercises and progressions can be found in the online-only Supplemental Material. A mandatory familiarization session was provided prior to the intervention to teach participants the exercises and allow them to try the appropriate progressions.
When the intervention began, participants were encouraged to choose an exercise in each progression scheme for the eight exercises that was challenging for them, but that they could still perform one set of 6 to 12 repetitions while maintaining good form. To employ the training principle of progressive overload, participants were advised to start each exercise with one set of 6 to 12 repetitions and to gradually increase in sets and repetitions first before moving through exercise progressions. When participants could successfully complete one set of 12 repetitions, they were advised to progress to two sets of 6 to 12 repetitions, and then three sets of 6 to 12 repetitions. Once participants could successfully perform three sets of 12 repetitions on an exercise, they were advised to move to the next progression. Participants were encouraged to take a rest period between each set of 1 to 3 min as needed (Izquierdo et al., 2021). They were each provided with a personal booklet to record their exercises, sets, and repetitions performed in each session. Each booklet had a list of the exercises to complete, photo demonstrations of each exercise, and a copy of exercise progressions included for reference.
Outcomes
Descriptive variables were collected at baseline to describe the sample including age (years), sex (M/F), marital status (married; not married), education level (high school or less; college or above), employment status (full-time; part-time; retired), household income (less than $50,000; more than $50,000), and self-reported health (Short-Form 36 Health Status Questionnaire (SF-36)) (Lyons et al., 1994). Chronic conditions and medications were self-reported by presenting participants with a list of 51 chronic conditions (e.g., diabetes, hypertension) and asking participants if they have a history of any of them, and asking how many different medications they take per day. Participants were screened using the Get Active Questionnaire to assess eligibility (Canadian Society of Exercise Physiology, 2017). Height and weight were measured, and body mass index was also calculated to describe the sample.
Physical activity level was measured via a wrist-mounted Axivity AX3 accelerometer (Newcastle, UK) (Clarke et al., 2017) to account for any interference due to a change in aerobic activities. The device was worn on the non-dominant wrist for 7 days at baseline, 6 and 12 weeks (Grimes et al., 2019). Autocalibration for the accelerometers was used (van Hees et al., 2014). The raw accelerometer data were processed using the software R (R Core Team, 2022) version 4.2.2, the software RStudio (RStudio Team, 2022) version 2022.7.0.548, and the GGIR package (Migueles et al., 2019), which has been previously validated (Sabia et al., 2014; van Hees et al., 2013). Data were only included if the participant had at least 4 days of valid data with at least 16 hr of valid data per day (Chen et al., 2009). The raw accelerometry data is measured in milligravity (mg), and the cut-points for light, moderate, and vigorous physical activity were 40, 100, and 400 mg, respectively (Migueles et al., 2019).
Besides the baseline characteristics captured to describe the sample, all outcomes were captured at baseline, post-control (6 weeks), and post-intervention (12 weeks). The main outcome was lower-body relative strength (maximal leg strength/lean leg mass). Maximal leg strength was assessed by performing between a 1- and 10-repetition maximum on a Nautilus leg press apparatus with 1-repetition maximum (1-RM) estimated using the Brzycki prediction equation (Brzycki, 1993): [load in kilograms/(1.0278−0.0278×repetitions)]
Lean leg mass was measured using Dual-energy X-ray Absorptiometry (DXA) (Hologic Horizon, Massachusetts, US). Full body scans were performed following the standardized protocol to assess total body composition in terms of lean mass, adipose tissue mass, and bone mass (Bazzocchi et al., 2016). Lean leg mass was then assessed bilaterally using the “region of interest” function (Bazzocchi et al., 2016), and the lean leg mass of both legs was added together to get the value for the denominator of the lower-body relative strength equation.
Secondary Outcomes
Secondary outcomes included measures of physical function, muscle power, and muscle strength. Physical function was measured using the 30-second chair stand test (Jones et al., 1999) and the one-leg stance test with eyes open (Hurvitz et al., 2000) as per their established protocols. For muscle power, leg extension power was measured using isokinetic dynamometry testing on a HUMAC NORM (Computer Sports Medicine Inc., Stoughton, MA.) (Habets et al., 2018). Participants started seated with their knees bent at 90° and had a fixed range of motion at the knee between 90° and 0°, with a fixed speed of 90°/s (Callahan et al., 2007). Upper body strength was assessed by estimating a chest press 1-RM using the same protocol and prediction equation as the maximal leg strength. Grip strength was measured with a JAMAR hand dynamometer (Bolingbrook, IL) using a standardized protocol (Canadian Society of Exercise Physiology, 2021).
Specific baseline characteristics of completers and non-completers were also assessed as a secondary outcome, including age (years), sex (M/F), body weight (kg), body mass index (kg/m2), body fat percentage, lean mass (kg), number of chronic conditions, number of daily medications, predicted 1-RM leg press (kg), predicted 1-RM chest press (kg), 30-second chair stand (repetitions), one leg stance (seconds), grip strength (kg), leg extension power (W), sedentary time (hours/day), moderate-to-vigorous physical activity (minutes/week), and whether or not they were meeting the aerobic physical activity guidelines of 150 min per week. All characteristics analyzed as part of this secondary outcome used the same protocols as outlined previously. A participant was identified as a completer if they completed the entire study protocol, including all 18 exercise sessions and the post-intervention testing.
Statistical Analysis
Due to a small sample, non-parametric tests were used to evaluate the results. The descriptive data are presented as the median (25th–75th percentile) for each variable. Friedman’s ANOVA was used to assess any changes over time in the main variable and secondary outcomes between baseline, control, and intervention. An alpha of 0.05 was used to determine significance over time. If a significant difference was detected, Bonferroni post hoc analyses were performed to determine where the effect occurred with a corrected alpha of .0167. A Mann-Whitney U test was conducted on the baseline characteristics of completers and non-completers to assess for any significant differences.
Results
Twenty-nine subjects initially agreed to participate in this study, and 17 completed the protocol (Figure 1).

Flowchart diagram of study participation.
During the control period, one participant dropped out due to an unrelated injury. During the intervention, 11 participants were lost to follow-up due to a change in health condition (n = 5), unforeseen circumstances (n = 2), unrelated injury (n = 1), inability to cope with the time commitment (n = 1), and two participants did not provide their reasoning for not completing the protocol. The baseline characteristics of the sample (n = 29) are presented in Table 1.
Participant Characteristics at Baseline (n = 29).
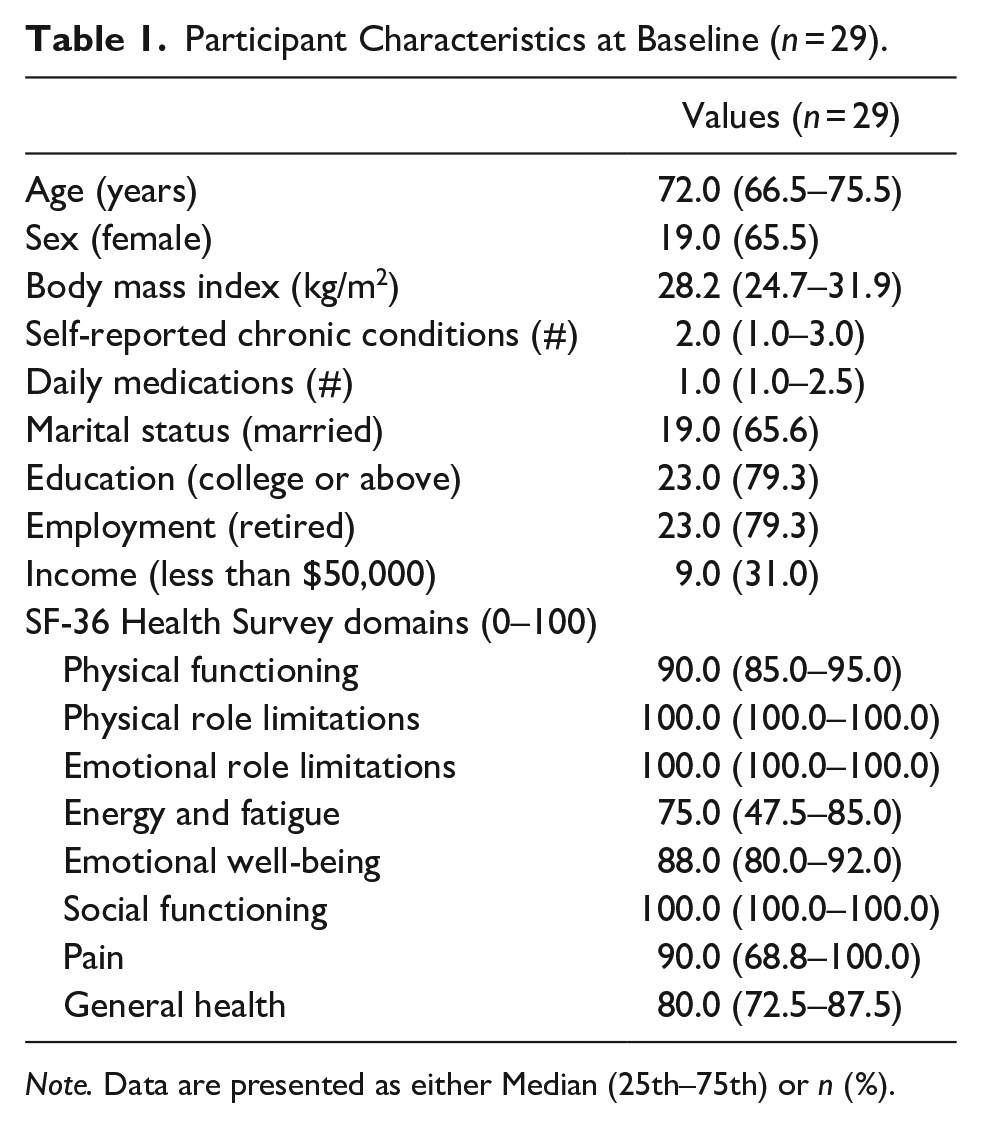
Note. Data are presented as either Median (25th–75th) or n (%).
The median (25th–75th) age of the participants was 72 years (66.5–75.5) and the sample was mainly composed of females, mostly married, those with a BMI between 25 and 30 kg/m2, those who have at least a college degree, and those who scored above a 75/100 on all eight domains of the SF-36.
For the main outcome of the study, a significant improvement was observed over time in lower-body relative strength (p = .002) (Figure 2).

Lower-body relative strength at all three time points.
Post hoc analyses revealed that there were no significant differences between lower-body relative strength at baseline and post-control at 6 weeks [7.82 (6.48–9.11) vs. 7.91 (7.01–9.35); p = .075], but there was a significant improvement between post-control and post-intervention [7.91 (7.01–9.35) vs. 8.50 (7.99–9.72); p = .002]. The individual values for lower-body relative strength are also plotted at each timepoint in Figure 2.
The median (25–75th) values for the secondary physical outcomes at baseline, post-control (6 weeks), and post-intervention (12 weeks) are presented in Table 2.
Physical Variables at All Three Time Points (n = 17).

Note. Data are presented as Median (25th–75th).
p < .0167 between post-control and post-intervention.
Maximal leg press improved significantly from post-control to post-intervention [102.4 kg (87.5–115.5) vs. 116.14 kg (87.01–134.9); p = .002)]. However, lower-body lean mass did not show a significant effect between post-control and post-intervention [12.3 kg (10.8–14.6) vs. 12.7 kg (10.8–15.0); p = .035). Between post-control and post-intervention, significant improvements were also observed in the 30-second chair stand (p < .001), one-leg stance (p = .011), and 1-RM chest press (p = .009). While a significant effect over time was observed in leg extension peak power (p = .039), Bonferroni-corrected post hoc analyses showed no significant differences between baseline and post-control (p = .492), or post-control and post-intervention (p = .022). No significant changes were noted in grip strength at any point (p = .138).
A comparison between participants who completed the program and those who did not are presented in Table 3.
Baseline Characteristics of Completers and Non-Completers.
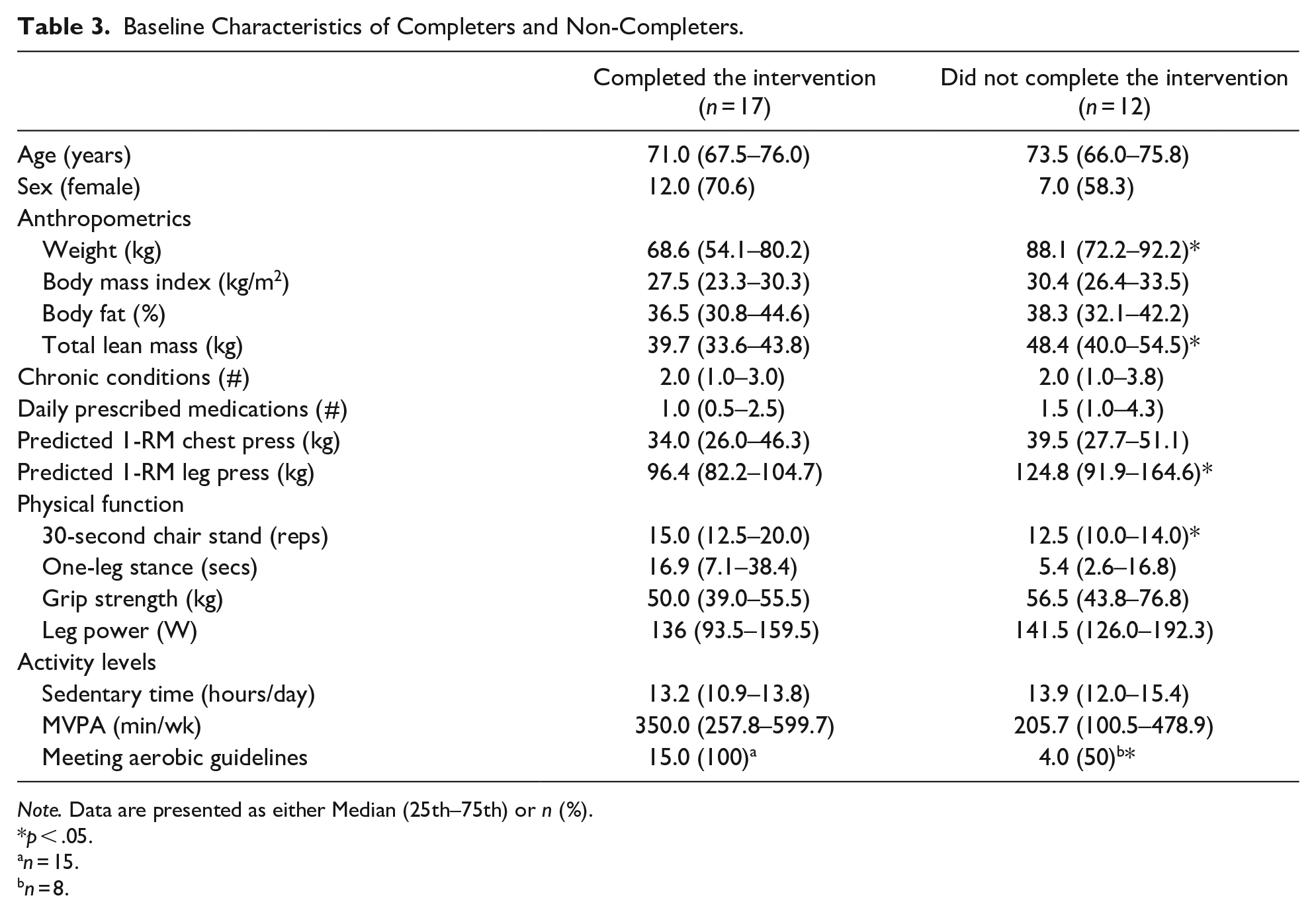
Note. Data are presented as either Median (25th–75th) or n (%).
p < .05.
n = 15.
n = 8.
Compared to those who did not complete the study protocol, completers at baseline weighed significantly less [68.6 kg (54.1–80.2) vs. 88.1 kg (72.2–92.2); p = .013], had significantly less lean mass [39.7 kg (33.6–43.8) vs. 48.4 kg (40.0–54.5); p = .034], performed a greater number of chair stands in 30 s [15.0 repetitions (12.5–20.0) vs. 12.5 repetitions (10.0–14.0); p = .029], and had a lower 1-RM leg press [96.4 kg (82.2–104.7) vs. 124.8 kg (91.9–164.6); p = .037]. Additionally, only 50% of non-completers were meeting the aerobic physical activity guidelines of 150 min of moderate-to-vigorous physical activity per week at baseline, while 100% of completers were meeting these aerobic guidelines at baseline (p = .003).
Discussion
The purpose of this study was to investigate the potential changes in lower-body relative strength after performing resistance training on an outdoor exercise structure for 6 weeks in adults aged 65+. Despite a drop-out rate of 41%, a significant improvement was observed in lower-body relative strength for those who completed the intervention, which was driven by an increase in maximal leg strength with a maintenance of lower-body lean mass. This study confirms the hypothesis that performing resistance training using an outdoor exercise structure for 6 weeks significantly improves lower-body relative strength in adults aged 65+.
Physical function and upper body strength also improved significantly. However, lower body strength improved at a higher rate than upper body strength from baseline to post-intervention. This could be due to the fact that the outdoor exercise structure used in this study was comprised of beams rather than conventional workout machines, so the majority of the exercises used were body-weight exercises using the beams for support. Because of this, the total load used would be greater for the lower body exercises than the upper body exercises.
The results of this study demonstrating that only 6 weeks of resistance training is associated with a significant increase in lower-body relative strength is important considering relative strength has been shown to be the strongest predictor of functional capacity, accounting for up to 42% of the variability in physical function (Misic et al., 2007). Also, since lean mass has been shown to decrease with age, performing resistance training activities could contribute to a greater lower-body relative strength by delaying the loss of muscle mass while improving muscle strength. The lack of change in lower-body lean mass observed in this study is consistent with a randomized control trial by Kim et al. (2018) who also observed an improvement in muscle strength, but not muscle mass. One could argue that this observation is in part due to the short duration of the intervention, however, Radaelli et al. (2021) found no association between intervention length and changes in lower-body relative strength in older adults, therefore a longer intervention may not have had any additional effect. More likely, the mechanism by which muscle strength was increased independently of muscle mass was an improvement in motor unit recruitment and coordination (Moritani, 1993). Research shows that neuromuscular adaptations such as improved neural drive, improved motor unit discharge, and improved movement pattern coordination occur around 6 weeks of resistance training and are primarily responsible for the initial increase in strength gains in inactive individuals (Van Cutsem et al., 1998).
In addition to significant improvements in the main outcome, a significant increase in the 30-s chair stand was also observed following the intervention, which is important given that older adults perform this movement at least 45 times per day on average (Bohannon, 2015). Additionally, an improvement of three repetitions was observed during the intervention, surpassing the minimal clinically important difference of two repetitions (Wright et al., 2011). Whether or not the use of an outdoor exercise structure can result in improvements in the 30-s chair stand is inconclusive in the literature, as the two existing randomized control trials which measured this variable have had conflicting results (Kim et al., 2018; Sales et al., 2017). An explanation for these discrepancies could be that in the Kim et al. (2018) study, only three exercises were included in the program and only one of those was a lower-body exercise, which was non-weight-bearing. Therefore, it was lacking in specificity for the 30-s chair stand assessment.
The potential for older adults to improve their balance following an exercise intervention using outdoor exercise structures is also disputed in the literature (Ng et al., 2021). Three randomized control trials which have assessed balance in older adults following the use of an outdoor exercise structure have found conflicting results (Kim et al., 2018; Leiros-Rodríguez & García-Soidan, 2014; Sales et al., 2017). However, it is worth noting that all three previous studies used different measures of balance and only one specifically targeted balance exercises during the intervention (Leiros-Rodríguez & García-Soidan, 2014), making it difficult to compare the findings and conclude whether the use of an outdoor exercise structure could lead to balance improvements.
Despite an improvement in lower-body relative strength and functional outcomes for participants completing the program, one of the most intriguing observations was a very high attrition rate (41%) in such a short period compared with previously reported attrition rates in the same demographic when performing resistance training (Cyarto et al., 2006). However, when looking at studies conducted by Leiros-Rodríguez and García-Soidan (2014) and Kim et al. (2018) with older adults using outdoor exercise structures, the attrition rates were 33.3% and 25.4%, respectively; therefore, it could be possible that attrition rates when using outdoor exercise structures are greater than in traditional and indoor settings.
Additionally, the present study found that non-completers were heavier than completers, had a greater absolute lean mass, and had a higher predicted 1-RM leg press, but had a lower 30-s chair stand score. This could suggest that heavier people may not be as functionally able, regardless of having more lean mass and higher absolute strength, and that they may have more difficulty performing body-weight exercises such as the ones performed in this study. These findings further support the importance of relative muscle strength rather than muscle mass or muscle strength independently for maintaining functional capacity. Our results and those from the literature suggest that outdoor exercise structures might not be well-suited for all people living in the community, and future studies should assess which populations would benefit the most from these resources. For this study, individuals who dropped out of the intervention were offered a free fall-prevention exercise program that had a lower exercise intensity than the outdoor exercise structure program.
Interestingly, most participants in this study (65%) met the aerobic physical activity guidelines of a minimum of 150 minutes of moderate-to-vigorous intensity weekly at baseline, suggesting that generally active older adults may be more interested in taking part in a program using outdoor exercise structures. This proportion is much higher than what is reported in the literature for aerobic physical activity levels in the general population of older adults (2.5%–17%) (Sun et al., 2013). Additionally, nearly two times more completers (n = 15) met these guidelines compared with non-completers (n = 8). This could suggest that those who are already active can add to their healthy behavior more easily, a phenomenon referred to as “habit-stacking” (Fiorella, 2020). More research should be conducted to explore which populations these outdoor exercise structures attract, and if the benefits are the same for those who are already physically active and those who are not.
As noted in a systematic review by Lee et al. (2018), outdoor exercise structures vary immensely from site to site, making it difficult to replicate studies and findings at different locations. While some outdoor exercise structures consist of equipment that resembles conventional exercise machines such as a leg press or stationary bicycle, others consist solely of an array of vertical and horizontal metal beams/bars. While it is unclear which style of equipment is most beneficial, some perceived benefits and drawbacks should be noted for each. While those that consist primarily of metal beams/bars (such as the one used in the present study) would likely be cheaper to install, require less maintenance due to the lack of moving parts, and may be more versatile in terms of which exercises can be performed, they may not be very beneficial to individuals who have little to no prior knowledge of exercise. As for the machine-based designs, they may be more costly to install and maintain, but would likely be easier to use for novice exercisers and may present less of a risk of injury due to clearer usage instructions and more stability provided. More research should be done regarding the types of outdoor exercise equipment available, and what the benefits and drawbacks are of each design to guide future installations.
Finally, some limitations need to be noted for this study. First, this study had a small sample size and a high attrition rate. Secondly, three sessions were canceled due to rain. However, because make-up sessions were offered after the initial 6 weeks, participants did not miss out on the total number of sessions. It is possible that limiting the study period to 6 weeks would not lead to a significant change in lower-body relative strength. The use of a ratio as the main outcome could be considered a limitation as a reduction in lean mass with the maintenance or even a loss in strength at a lower rate could result in an improvement in the relative strength ratio, even though the loss of lean mass or strength would theoretically be an unfavorable outcome. Finally, the baseline information of the sample does not seem to represent adults aged 65+ in terms of aerobic physical activity levels.
In conclusion, the current study demonstrates that performing resistance training on an outdoor exercise structure for 18 sessions has the potential to result in significant improvements in lower-body relative strength, as well as other functional outcomes. However, the attrition rate observed in this study calls for more research to understand if these structures should be promoted for seniors living in the community.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214241232552 – Supplemental material for Resistance Training on an Outdoor Exercise Structure Improves Lower-Body Relative Strength in Older Adults
Supplemental material, sj-docx-1-ggm-10.1177_23337214241232552 for Resistance Training on an Outdoor Exercise Structure Improves Lower-Body Relative Strength in Older Adults by Brianna Leadbetter, Martin Sénéchal, Ken Seaman and Danielle R. Bouchard in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-2-ggm-10.1177_23337214241232552 – Supplemental material for Resistance Training on an Outdoor Exercise Structure Improves Lower-Body Relative Strength in Older Adults
Supplemental material, sj-docx-2-ggm-10.1177_23337214241232552 for Resistance Training on an Outdoor Exercise Structure Improves Lower-Body Relative Strength in Older Adults by Brianna Leadbetter, Martin Sénéchal, Ken Seaman and Danielle R. Bouchard in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
Before the study began, this project was reviewed and approved by the University of New Brunswick Research Ethics Board under the file REB #2022-080
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.