
Abstract
Introduction
The rate of medical complications following spinal surgery in patients over 80 years old may seem frightening for both patients and surgeons. Indeed, the rate of readmissions and mortality for spinal surgery in this population have been showed to be up to 10% in the literature, but with a large variation depending on the surgical procedure (emergencies procedures, lumbar decompression alone or associated with fixation) (Cloyd et al., 2008; Deyo et al., 1993; Silvers et al., 1993).
Interestingly, prosthetic surgery for hip and knee replacement (respectively THR and TKR) for elderly patients are more routinely performed than spinal surgery and may therefore seem safer (García Rey et al., 2021; Rubin et al., 2016; Sloan et al., 2018). This is probably due to the frequency of fractures of the upper end of the femur in patients over 80 years of age. Indeed, the loss of autonomy in the event of delayed intervention would be disastrous for these patients, explaining the systematic recourse to surgery in these cases (Davanzo et al., 2021; Francony et al., 2022). On the other hand, spinal surgery provides the best improvement of quality of life, compared to all other types of orthopedic surgery, including lower limb surgery (Hansson et al., 2008). Additionally, delayed surgery for orthopedic conditions impacting ambulation leads to decreased survival, in addition to impaired quality of life. However, if the quality of life and preservation of function are particularly relevant when considering elderly subjects, the risks related to general anesthesia and surgical complications are higher. Moreover, due to the recent development of minimally invasive techniques for spinal surgery and better collaboration between geriatric specialists and orthopedic surgeons, we may think that the morbidity of spinal surgery has decreased (Yolcu et al., 2021). Does scheduled spinal surgery for patients over 80 years-old deserve such apprehension compared to THR or TKR?
The main goal of this study was to compare, within a homogeneous monocentric cohort, the rate of medical complications and the length of hospital stay of spinal surgery (SS) compared to LLPS (lower limb prosthetic surgery) in patients older than 80 years old.
Material and Methods
This was a retrospective monocentric study, registered at the APHP IRB (number 20220304155259). All patients over 80 years old that underwent spinal surgery (SS) or lower limb prosthetic surgery (LLPS) between December 2018 and December 2020 were included as a continuous study.
The data collected pre-operatively for each patient were:
- Demographic: age, sex, BMI (body mass index)
- Clinical: ASA score, hemoglobin, creatinine, diabetes (yes/no), anticoagulant use (yes/no), antiaggregant use (yes/no)
The patients were classified in groups according to the type of surgery performed. For spine surgery, the decompressed levels and the fused levels were recorded. For LLPS, the joint concerned (hip or knee) was recorded, as well as surgical indication: primary joint replacement or revision.
The patients were then classified in two groups according to the surgical severity, in order to take into account blood loss and general anesthesia duration:
- G1 (group 1):
○ For LLPS: primary joint replacement (THR or TKR),
○ For SS: decompression alone (revision or primary) or associated with spinal fusion on less than3 levels.
- G2 (group 2):
○ For LLPS: revision prosthetic surgery (RTHR or RTKR),
○ For SS: spinal fusion of more than3 levels.
The post-operative data collected were:
- Duration of hospitalization (in days)
- Destination at discharge from orthopedic surgery department: home or rehabilitation facility
- Total number of medical complications
- Type of medical complications: surgical site infection (with reintervention), neurologic (confusion, stroke), cardiopulmonary (veinous thrombosis, arrhythmia), digestive (sub-occlusion or occlusion, esophagitis bleeding. . .), acute post-operative anemia requiring blood transfusion, urinary (urinary tractus infection, acute urine retention requiring bladder catheterization), falling and metabolic (abnormality on the serum electrolytes dosage requiring corrective medical intervention).
The statistical analysis was made on XLstat, with Student’s t tests. p-Values lower than .05 were considered significant.
Results
One hundred sixty-four patients have been included in the study. The population consisted of 80 patients that underwent lower limb prosthetic surgery and 84 patients that underwent spinal surgery. The flowchart of the study is presented as Figure 1. The mean age was 84 years old. The pre-operative characteristics of the cohort are summarized in Table 1.

Flowchart of the patient’s selection for the study. G1: Group 1; G2: group 2.
Pre-operative Parameters of the Cohort Depending of the Surgery Performed.

Note. Numeric variables are expressed as mean ± standard-deviation [min-max]. p < .05 (T-test) was considered statistically significant.
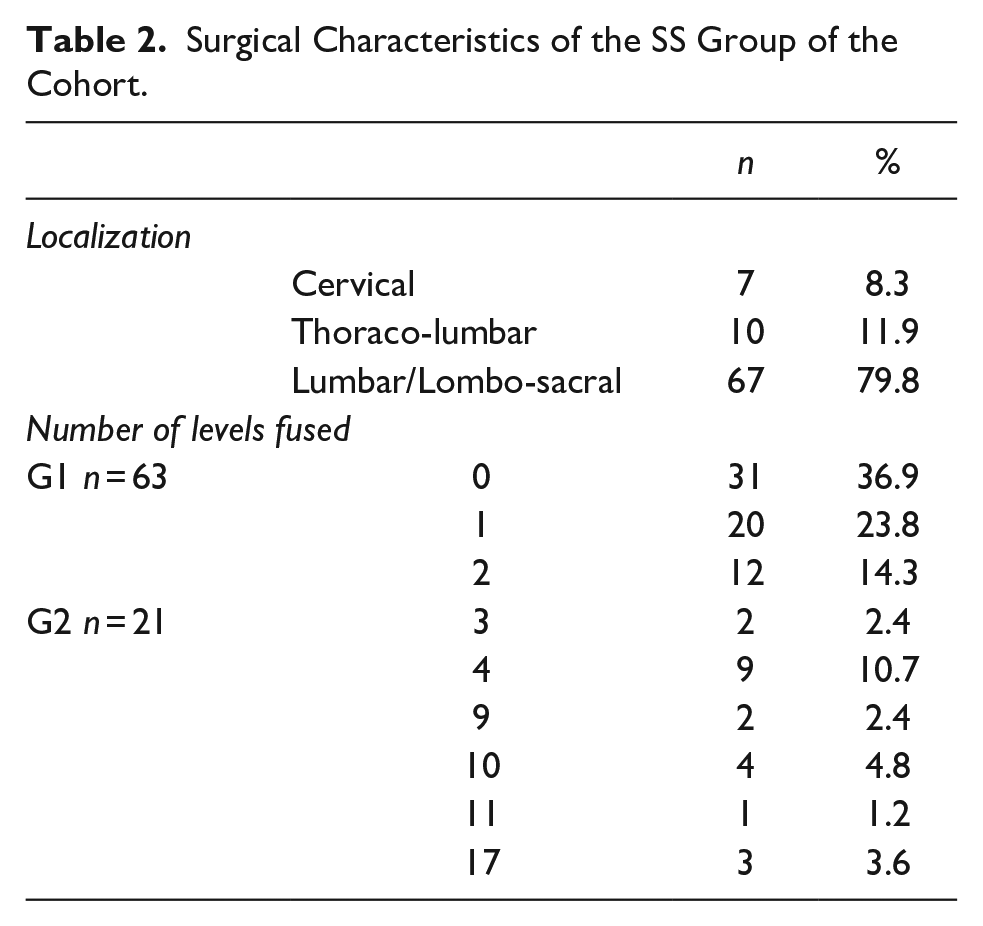
There were 84 patients in the SS group and 80 in the LLPS group. Out of the 80 LLPS group, 16 patients underwent revision surgery and were classified in the G2 severity group. Twenty-one patients of the SS group underwent a fusion or three levels or more, classifying them as G2. The characteristics of the surgical indications on the SS group are summarized in Table 2.
Surgical Characteristics of the SS Group of the Cohort.
The mean number of peri-operative complications, occurring during hospital stay was 1.11 ± 0.6 [0–6] for spinal surgery and 1.09 ± 1.0 [0–3] for LLPS (p = .87). The length of hospitalization was statistically comparable between the two groups: 10.7 ± 4.9 days [2–36] for SS and 10.7 ± 3.0 days [5–11] for LLPS (p = .96). The most frequent types of complication encountered for the whole cohort were cardiopulmonary events (36 patients, 22%), followed by urinary complications (31 patients, 19%), metabolic (29 patients, 18%), digestive (27 patients, 16%), anemia (18 patients, 11%), surgical site infection (16 patients, 10%), neurologic (14 patients, 9%), and falls (11 patients, 7%). The peri-operative data are summarized in Table 3.
Peri-operative Medical Complications of the Cohort, Depending of the Surgery Group (Spinal or Lower Limb).

Numeric variables are expressed as mean ± standard-deviation [min-max]. p < .05 (T-test) was considered statistically significant.
Considering the two severity groups, G1 and G2, the mean hospital stay was 9.8 ± 4.2 days [2–31] for G1 spine, 9.6 ± 3.2 days [3–27] for G1 lower limb, 13.3 ± 6.1 days [4–36] for G2 spine and 15.6 ± 10.4 days [4–69] for G2 lower limb. The difference between the two G1 groups was not statistically significant (p = .78), neither between the two G2 groups (p = .59).
The variation between groups of the mean number of complications is summarized in Figure 2.

Barplot showing the mean number of medical complications according to the surgical group of the cohort.
The difference in the number of medical complications was statistically significant between G1 lower limb and G2 lower limb (p = .008), as well as between total G1 and total G2 (p = .02). No statistically significant difference was found between G1 spine and G2 spine (p = .08), G1 spine and G1 lower limb (p = .68), and G2 spine and G2 lower limb (p = .61).
Discussion
These results show that the global rate of peri-operative complications and the length of hospital stay were similar between spinal surgery and lower limb prosthetic surgery for patients over 80 years old on comparable groups. When analyzing the impact of the surgical severity (G1 vs. G2), it does seem that its increase leads to more complications in lower limb surgery than spinal surgery.
Although comparison between lower limb and spinal surgery is interesting, a question that may be more accurate is how to optimize peri-operative course for these patients. Indeed, enhanced recovery after surgery (ERAS) has shown satisfactory results in both lower limb and spinal surgery (Frassanito et al., 2020). ERAS allows the reduction of complication rates, including transfusion rates, post-operative pain and opioid consumption, which may be particularly deleterious in elderly patients (Hardy et al., 2022; Jenny & Gisonni, 2022; Jeschke et al., 2022; Picart et al., 2021). Considering elderly patients, experiences from traumatology showed that the association with geriatric post-operative care-units improved both mortality and post-operative quality of life (Davanzo et al., 2021; Francony et al., 2022). These units may notably improve peri-operative immunonutrition, a major factor based on biological and physiological landmarks for decreasing peri-operative complications (Gonçalves et al., 2021). Management strategy for elderly is indeed based on early mobilization, accurate pain management, swallowing disorders detection, stool impaction and urinary retention detection, delirium detection, and malnutrition management. If surgical complications in spinal surgery, such as PJK (proximal junctional kyphosis) and non-union, have been extensively studied in adult spinal deformity, medical complications tend to get fewer attention in the surgical community (Bouyer et al., 2017). However, in fragile population, such as elderly patients, complications impacting quality of life and rates of re-admissions are mostly medical and often the consequences of decompensation of underlying medical conditions (Saleh et al., 2017; Schwab et al., 2012; Zanirato et al., 2018). The management of these patients has therefore to be a tripartite approach (surgeon – anesthesiologist – gerontologist) rather than the usual duo (surgeon – anesthesiologist). Notably, gerontologists are aware of concept of frailty that appears to be predictive of post-operative complications. It should be used systematically in the ortho-geriatric population, for assessment and correction of modifiable factors pre-operatively (Rogers et al., 2020). Frailty has also been linked to hospital length of stay increase and long-term mortality in femoral neck fractures in elderly patients (Krishnan et al., 2014; Patel et al., 2014).
This study may have some limitations. First, its retrospective nature may lead to recognition bias. However, complications were collected in the same manner for LLPS and SS, decreasing the impact of possible bias. In terms of groups comparison (G1 and G2), the defined threshold may lead to some discrepancy (e.g., all THR revision procedures do not lead the same blood losses and operative times), but it reflects daily practice in an orthopedic center. Secondly, the sample size of patients in G2 groups calls for caution in the interpretation of the results. Indeed, the size of these sub-cohorts may be explained by the selection of patients eligible to undergo such heavy surgeries, this analysis being realized a posteriori.
In conclusion, spinal surgery in elderly patients does not seem to lead to more early post-operative complications than lower limb prosthetic surgery. However surgical indications must be carefully chosen with both geriatric, anesthetic and surgical pre-operative evaluation, and patients should benefit from centers with geriatric expertise.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics
This study was conducted according to the World Medical Association Declaration of Helsinki.