
Abstract
Mild Cognitive Impairment (MCI) affects 15% of adults 50 years old and over. Individuals living with MCI have shown decreased social participation, a critical activity as it may delay cognitive decline. Depression may be a key factor in limiting participation. This study is a secondary data analysis of 30 older adults living with MCI, looking for associations with participation. Participation was examined using the Patient Reported Outcomes Measurement Information System (PROMIS®) Satisfaction with Participation in Social Roles Computer Adaptive Test (CAT) form. Depressive symptoms were reported using the PROMIS Quality of Life in Neurological Disorders Depression CAT form and the Patient Health Questionnaire (PhQ-9) form. Results showed that demographics (age, sex) were not significantly associated with participation, but depressive symptoms were significantly associated. This suggests that adults living with MCI who have higher levels of depressive symptoms may be a uniquely vulnerable population who benefit from interventions that support participation.
Introduction
Mild Cognitive Impairment (MCI), a state between typical cognitive aging and dementia, can affect over 15% of community-dwelling older adults over 50 years old worldwide (Bai et al., 2022). MCI is a known correlate of reduced participation in daily activities (Avila et al., 2015). It is important to understand the correlates of social participation among individuals living with MCI because emerging evidence suggests that social participation may be protective against MCI or delay cognitive decline for those living with MCI (Hughes et al., 2013; Smith et al., 2022). Several mechanisms may explain the link between social participation and cognitive functioning: social participation may be supporting brain health by reducing stress, building cognitive reserve, and/or decreasing depression symptom burden (Sommerlad et al., 2023). Social participation has been operationalized into dimensions of structural (isolation), functional (perceived social support/loneliness) and quality (relationships) of social support, with each domain affecting outcomes differentially (Lutz et al., 2021). Less is known about what type(s) of social connectivity confer protection against MCI in older adults.
Existing research on social participation in older adults with MCI has focused largely on external or environmental barriers and less on personal or psychological factors that may impact engagement in social activities. One personal factor that is important to consider in the context of brain aging is depression. Depression is a public health relevant problem in late life and associated with an increase in disability, physical comorbidities, cognitive decline, and early mortality (Reynolds et al., 2022). Depressive symptoms are highly prevalent in older adults living with MCI (Ismail et al., 2017), and occur in as many as 50% of those individuals, leaving them vulnerable to both the negative health effects of depression as well as an elevated risk for withdrawal in social activities (Palmer et al., 2010). The associations among social participation, depression, and MCI are complex. For instance, depressive symptoms can inhibit participation in older adults, especially among individuals living with MCI (Galenkamp et al., 2016; Rovner et al., 2016). Conversely, social participation is associated with less depressive symptom burden (Zhang et al., 2023). Moreover, depression can be a risk factor for MCI/dementia leading to social withdrawal (Gardener et al., 2021). Social disconnection (i.e., a result of geographic isolation, bereavement, and/or caregiving) can also lead to cognitive decline which impacts changes in mood and depression. Further analyses on these complex relationships is needed. Additionally, it’s important to distinguish the type of depressive symptoms, which can be measured as (1) depressed mood symptoms or (2) somatic (sleep, appetite) symptoms. Clarity is needed to further understand which specific depression symptoms may increase vulnerabilities for individuals living with MCI (Carvalho et al., 2013).
The purpose of this study was to examine the role of depressive symptoms in predicting social participation in a well-characterized sample of older adults living with MCI. We hypothesized that greater depressive symptom burden would be associated with less social participation, after controlling for demographic variables known to be associated with participation in late life.
Methods
We conducted a secondary analysis of a randomized controlled (RCT) trial testing an intervention for community-dwelling older adults living with MCI (Rodakowski et al. 2018). We conducted a cross-sectional study using baseline data from this RCT. Participants were recruited using advertisements in print- and on-air media, radio advertisements, internet advertising, community-based presentations, and community mailings. The parent study obtained Institutional Review Board approval, and participants provided written, informed consent.
Participants
Inclusion criteria included (1) being determined to have MCI [REDACTED: AUTHOR’S CITATION], (2) being community-dwelling, (3) being 60 years old or older, (4) reporting a challenge with one or more daily activities, and (5) scoring a 1 or greater on the Patient Health Questionnaire 2-item version (PHQ-2) (Kroenke et al., 2003). Older adults were excluded if they (1) self-reported having major depression based on the PRIME-MD, (2) reported a lifetime history of schizophrenia or bipolar disorder, (3) had an alcohol or substance use disorder reported in the past 5 years, or (4) had a complex medical history, such as a central nervous system disorder.
Procedures
Potential older adult participants were screened using a three-step process comprised of a phone screen, initial in-person screening, and full in-person screening. In the parent study, 236 participants were screened. Of the 236, 170 (72%) did not meet study criteria and 36 (15%) declined participation prior to consent. Baseline assessments were completed by 30 participants.
Primary Outcome
Participation was measured using the Patient Reported Outcomes Measurement Information System (PROMIS®) Item Bank v1.0—Satisfaction with Participation in Social Roles Computer Adaptive Test (CAT) form (Hahn et al., 2010). This tool measures satisfaction with performing one’s usual social roles and activities in the past 7 days. Items are rated on a 5-point scale from 1 (not at all) to 5 (very much). We computed a T score in which a higher score indicated more satisfaction with participation.
Correlates of Participation
Demographic Characteristics
Participant demographic characteristics were collected based on participant report of their demographics. Age and sex were used to control for potential confounding factors within participants living with MCI, as they are known risk factors that increase vulnerability within this diagnostic group. As a part of their screening process, participants completed the Generalized Anxiety Disorder 7-item (GAD-7) (Spitzer et al., 2006), the Quick Mild Cognitive Impairment Screen (Qmci) (Clarnette et al., 2017), and the Modified Mini-mental State Examination (3MS) (Teng & Chui, 1987).
Depressive Symptoms
Depressive symptoms were reported using the PROMIS Quality of Life in Neurological Disorders (Neuro-QoL) Item Bank v1.0—Depression Computer Adaptive Test (CAT) form (Cella et al., 2010; Segawa et al., 2020). This tool measures depressive symptoms in the past 7 days on a 5-point scale from 1 (never) to 5 (always). We computed a T score in which a higher score indicated a higher level of depressive symptoms. A majority of these items represented depressive mood symptoms.
Depressive symptoms were reported using the Patient Health Questionnaire (PhQ-9) (Kroenke & Spitzer, 2002). This self-administered tool measures depressive symptoms in the past 2 weeks on a 5-point scale from 0 (not at all) to 3 (nearly every day). We computed a mean score in which a higher score indicated a higher level of depressive symptoms. A majority of these items measured somatic symptoms.
Data Analyses
The data were analyzed using IBM SPSS Statistics (version 28) (IBM Corp, 2022). We performed tests of normality for variables. We described our participant characteristics using descriptive statistics. We computed bivariate correlations among all continuous measures using Pearson statistics and Kendall’s Tau. We set a benchmark (p < .05) for the correlation of any mental health measure with satisfaction in participation in social roles to move forward in our analysis and be assessed for inclusion in our model. We compared the PROMIS and PhQ-9 depressive symptom measures for correlations with participation. We ran a hierarchical multiple regression analysis and assessed variables for multicollinearity. Age and sex were entered into the analysis because of their known risk factor in this sample of older adults, providing a foundation for comparison. Block 1 included the demographics of sex and age. The PROMIS depressive symptom measure was added into the analysis in Block 2 to answer the research question of understanding the unique contribution of depressive symptoms to the variance in participation. The Results explicate the exclusion of the Ph-Q score and the PROMIS Anxiety T score in the model.
Results
Most participants were women (66.67%, n = 20), white (86.66%, n = 26), and received a high school education (40.0%, n = 12). Their mean age was 78 years (SD = 8.68 years). Participants’ mean scores on the PHQ-9 were 5.60 (SD = 4.75) and their scores on the GAD-7 were 3.90 (SD = 4.16), indicating mild depression and anxiety symptom burden. Their mean Qmci scores were 57.33 (SD = 7.37) and their mean 3MS scores were 93.57 (SD = 3.80) (Table 1), indicating that participants’ scores were consistent with MCI but not consistent with moderate cognitive impairment.
Demographic Characteristics of Participants at Baseline.

Note. PhQ-9 = Patient Health Questionnaire(Kroenke & Spitzer, 2002); GAD-7 = Generalized Anxiety Disorder 7-item Scale (Spitzer et al., 2006); Qmci = Quick Mild Cognitive Impairment Screen (Clarnette et al., 2017); 3MS = Modified Mini-mental State Examination (Teng & Chui, 1987); M = mean; SD = standard deviation.
Correlation Analyses
All T score measures met the assumptions of normality. The PhQ-9 scores deviated from normal, W(30) = 0.891, p = .005. Pearson’s and Kendall’s tau correlations were run between all continuous variables. Correlation coefficients are presented in Table 2. Both anxiety and depression T scores were correlated with satisfaction with participation in social roles (i.e., r > .10) and statistically significant. The PROMIS depressive symptom measure was included in the regression model because of its higher correlation coefficient (r = −.619), than the PhQ-9 (r = −.374).
Correlates of Satisfaction with Participation in Social Roles.

Note. Pearson correlations, unless noted with T (Kendall’s Tau correlation).
p ≤ .05. **p ≤ .01.
Hierarchical Multiple Regression Analysis
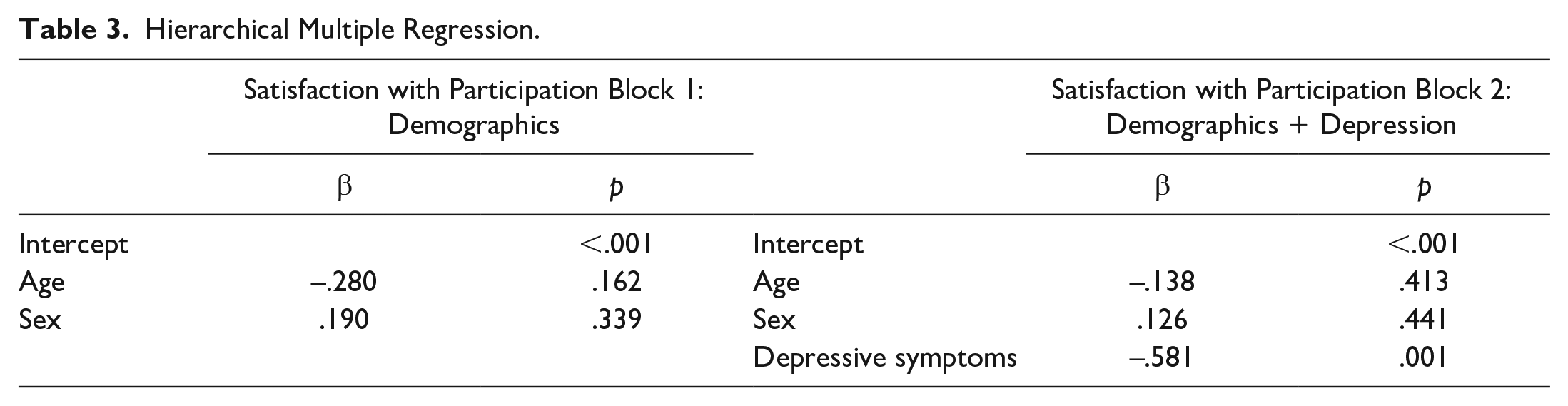
In addition to depression, anxiety was initially included in the model and assessed for multicollinearity. Due to a correlation of r = .828, anxiety was removed. In Block 1, demographic characteristics contributed 2% of the variance in satisfaction with participation in social roles. In Block 2, after controlling for demographic characteristics, depressive symptoms contributed an additional 31.6% of the variance in participation (F (3,24) = 5.546; R2 adj = .336, p = .005).
Depressive symptom scores (β = −.581, p = .001) were significantly associated with participation, while age (β = −.138, p = .413) and sex (β = .126, p = .441) were not, based on standardized beta scores (Table 3).
Hierarchical Multiple Regression.
Discussion
The purpose of this study was to examine the contribution that depressive symptoms made to social participation in community-dwelling older adults living with MCI. We found the PROMIS measure of depressed mood (r = −.619), rather than the PHQ-9 measure of somatic symptoms (r = −.374), to be stronger in the relationship between depression and social participation. Depression symptoms in late-life can be grouped into the domains of depressed mood, anhedonia, somatic symptoms, and sleep complaints, among others. Our finding that depressed mood is associated with less social participation contrasts with other studies that suggest that somatic mental health was associated with participation in older adults (Rashedi et al., 2014). Our results suggest that it may be important to distinguish between psychological and somatic symptoms of depression when trying to increase participation in social activities.
Social disconnection has been operationalized into structural (isolation), functional (perceived social support/loneliness), and quality (relationships) domains (Lutz et al., 2021). This study utilized the PROMIS measure of Satisfaction with Participation in Social Roles, which suggests an alignment with functional support. These findings build evidence for understanding the link between the functional aspect of social participation and depression symptoms.
Knowing that age and sex may be a risk factor of decreased social participation during cognitive decline, depressive symptoms accounted for over 30% of the variance in participation scores (Ferguson, 2009). Our findings suggest that higher levels of depressive symptoms were associated with decreased levels of participation, which is consistent with other studies (Rovner et al., 2016). Knowing that adults living with Mild Cognitive Impairment and depressive symptoms are likely more vulnerable to decreased participation can inform community social support services of a key population to support.
Older adults living with MCI are at high risk of developing dementia, making this a potent time for developing interventions that protect against cognitive decline. Interventions have been developed to support cognition but have shown mixed results [REDACTED: AUTHOR’S CITATION]. Given that social participation delays cognitive decline and may be protective against MCI (Hughes et al., 2013; Smith et al., 2022) our findings help clarify a subset of those living with MCI who may be particularly vulnerable to decreased participation. Additionally, knowing that a proposed mechanism of social participation’s support of cognitive functioning is that participation decreases depressive symptom burden, these findings add knowledge for further mechanism testing. However, more research is needed to determine whether longitudinal change in depression is associated with change in social participation (and vice versa). It is possible that adding a social component to current lifestyle interventions may have a synergistic effect on both depression and cognitive health outcomes.
Study Limitations
We acknowledge several study limitations. First, participants were predominantly white, and therefore the sample may not be representative of older adults living with MCI. Second, the sample was drawn from a single geographic location, which also may limit generalizability. Third, this is a cross-sectional analysis, so we cannot infer causal interpretations of these findings. However, this study has strengths. The MCI diagnoses followed the National Institute on Aging-Alzheimer’s Association criteria [REDACTED: AUTHOR’S CITATION], creating a clearly defined group of people living with MCI. Our findings provide the basis for future studies of older adults living with MCI.
Conclusions
In summary, more depressive symptom burden—particularly depressed mood—are associated with less social participation in older adults living with MCI. This finding improves our understanding that a distinct population of older adults living with MCI—those with depressive symptoms—may be particularly vulnerable to a decrease in participation. This may be useful for identifying ways to support depressive symptoms and inform future interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Acknowledgement of financial support funding was received from the National Institutes of Health grants KL2 TR001856, P30 MH090333, P50 AG05133, R01 AG056351, UL1 TR000005.
Financial Disclosure
We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated.
Ethical Approval
University of Pittsburgh Institutional Review Board protocol number: PRO14070341.