
Abstract
Introduction
Ulcerative colitis (UC) is a disease of repeated relapses and remissions, and the number of UC patients is increasing worldwide, including Japan (Asakura et al., 2009; Cosnes et al., 2011; Murakami et al., 2020). In the clinical setting, maintaining mucosal healing (MH) among patients with UC was an established treatment goal in several previous studies (Colombel et al., 2011; Frøslie et al., 2007; Lichtenstein & Rutgeerts, 2010; Peyrin-Biroulet et al., 2011; Sandborn et al., 2016; Shah et al., 2016).
Constipation, a common gastrointestinal symptom, might worsen quality of life (Belsey et al., 2010; Koloski et al., 2013; Wald et al., 2007) and negatively impact social labor productivity (Sun et al., 2011). Additionally, constipation is associated with chronic kidney disease (Sumida et al., 2017), incidence of cardiovascular disease (Salmoirago-Blotcher et al., 2011), and all-cause mortality (Sumida et al., 2019). In a Japanese population-based study, lower defecation frequency was associated with cardiovascular disease mortality (Honkura et al., 2016). In a United States (US) study, female gender and aging was positively associated with the prevalence of constipation (Choung et al., 2007). Similarly, in Japan, according to the 2019 Comprehensive Survey of Living Conditions, the prevalence of constipation is 34.8% in total study population and 68.6% in 65 years and older (Ministry of Health, Labour and Welfare, 2019). The prevalence of constipation increases with age in both men and women (Choung et al., 2007; Higgins & Johanson, 2004; Roque & Bouras, 2015).
Previous studies showed the close association between UC and constipation. Approximately one-third to one-half of patients with UC suffered from symptoms of constipation (James et al., 2018; Lennard-Jones et al., 1962). Disease activity is positively associated with the prevalence of constipation (OR 5.56 [1.96, 16.67]), while age, disease duration, or treatment was not associated with constipation (James et al., 2018). Despite the adverse effects of constipation on various diseases, the evidence of constipation in UC is modest. In addition, relevant evidence of constipation in Japanese patients with UC is lacking. Therefore, we aimed to evaluate the association between UC disease activity and constipation in Japanese patients.
Methods
Study Design
This was a cross-sectional study that used baseline data from a prospective cohort study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) and was approved by the Institutional Review Board of the Ehime University Graduate School of Medicine (No. 1505011). Well-trained staff obtained written informed consent from all enrolled patients. The study was registered at each hospital between 2015 and 2019.
Study Population
The study subjects consisted of 387 Japanese patients with UC seen at the Department of Gastroenterology and Metabology of the Ehime University Graduate School of Medicine, and at several affiliated hospitals and clinics in Ehime prefecture. All patients were diagnosed with UC according to endoscopic, radiological, histological, and clinical criteria. Consecutive outpatients and inpatients with UC who could understand our study were candidates. Even after being informed about the study and agreeing to participate, 97 subjects did not agree to undergo the colonoscopy and blood test; thus, some data are missing. After these 97 patients were excluded due to incomplete data, the final analysis sample in this study consisted of 290 patients (Figure 1).

Flow chart of the present study.
Measurements
Information on duration of UC, medication for UC, and disease extent was collected from medical records. Body mass index (BMI) was calculated as weight in kilograms divided by square of height in meters.
Definition of Constipation
The Rome I criteria for constipation, as recommended by an international workshop on constipation management, were used in this study (Whitehead et al., 1991). Constipation was assessed using four questions that pertained to the last 12 months and were as follows: (1) Do you experience straining during bowel movements?; (2) Do you feel a sense of incomplete evacuation after bowel movements?; (3) How often do you experience hard stools?; and (4) How frequently do you have bowel movements each week? Respondents could choose from four answer options for questions 1–3: never, sometimes (<25% of the time), often (>25% of the time), and always. Constipation was defined as meeting two or more of the four criteria, with an answer of “often” or “always” for questions 1–3 and less than three bowel movements per week for question 4. Information regarding medication for constipation was obtained using self-administered questionnaire. In this study, the definition of constipation was based on Rome I criteria and/or medication for constipation.
Definition of Mucosal Healing and Clinical Remission
A certified endoscopist evaluated mucosal status by total colonoscopy. Endoscopy was performed as required by the attending physician. In patients with newly diagnosed UC, colonoscopy was performed regardless of the severity of symptoms. Complete MH was defined as Mayo endoscopic score (MES) category 0 (Schroeder et al., 1987). Clinical remission (CR) was defined as no rectal bleeding and no abnormally high stool frequency (<3 times per day) at the time of this study’s research. One endoscopic specialist was responsible for evaluating MES, CR, and MH, and was blind to constipation.
Statistical Analysis
Duration of UC was divided into two groups: (1) <7 years and (2) ≥7 years. Disease extent was divided into two groups: (1) pancolitis and (2) non-pancolitis. Age was divided into five groups of 10 years each: (1) Under 40 years old, (2) 40–49 years old, (3) 50–59 years old, (4) 60–69 years old, and (5) 70 years old and over. Multiple logistic regression analyses were used to adjust for potential confounding factors. Sex, age, BMI, current drinking, and current smoking were selected as confounding factors. Trend of association was assessed using a logistic regression model assigning consecutive integers to the categories of the age variables. Statistical analyses were mainly performed using the SAS software package ver. 9.4 (SAS Institute, Cary, NC, USA). All probability values for statistical tests were two-tailed, and a p-value of < .05 was considered statistically significant.
Results
Table 1 shows the characteristics of the 290 study participants. The percentage of men was 57.6% in this study population. The mean age and BMI were 50.4 years and 22.54 kg/m2, respectively. The percentage of <40 years, 40–49 years, 50 to 59 years, 60 to 69 years, and >70 years was 29.0%, 23.8%, 17.6%, 17.6%, and 13.5%, respectively. The prevalence of constipation, complete MH (MES 0), and CR was 12.4%, 25.2%, and 57.6%, respectively.
Clinical Characteristics of 290 Study Participants.
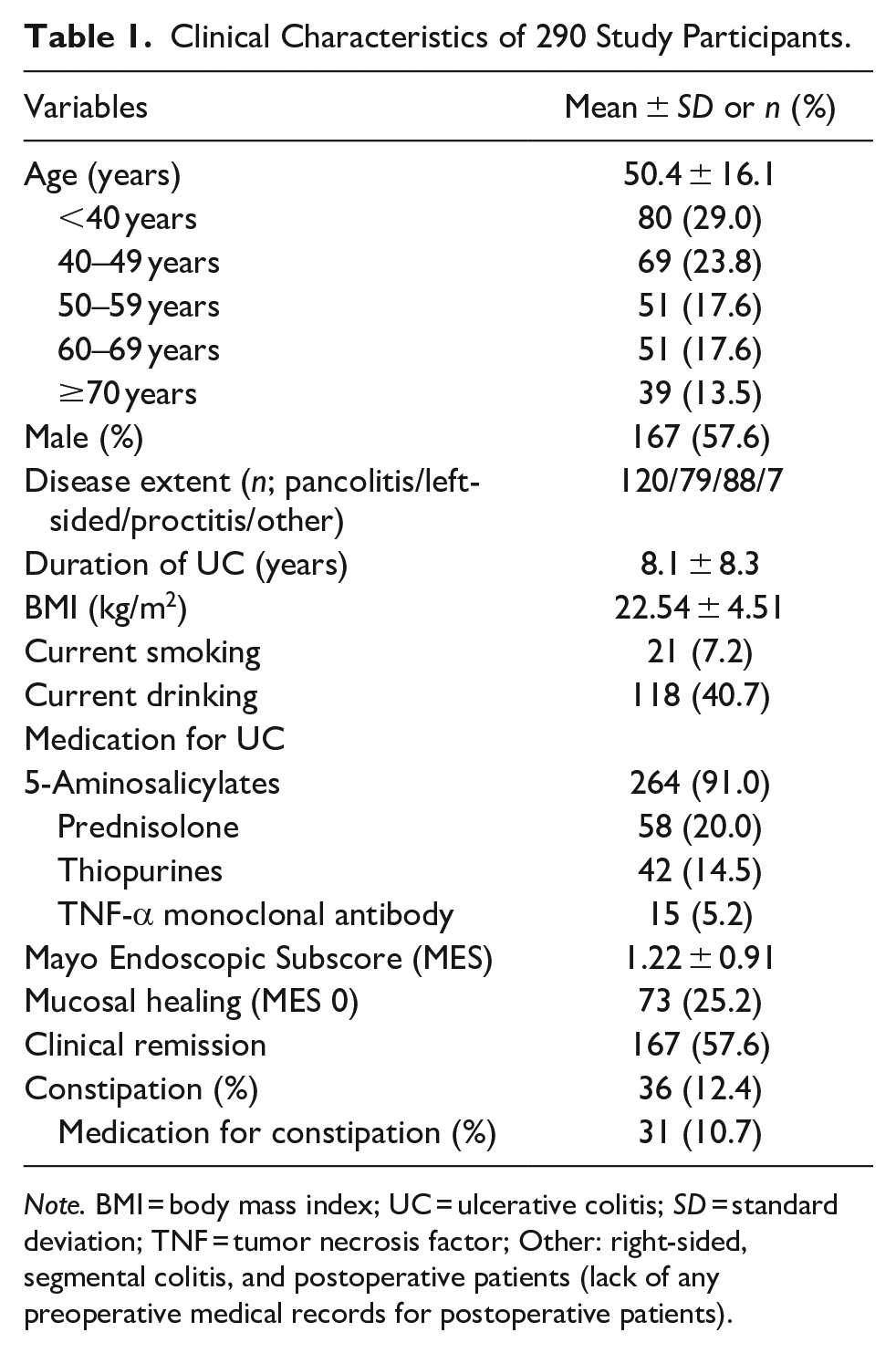
Note. BMI = body mass index; UC = ulcerative colitis; SD = standard deviation; TNF = tumor necrosis factor; Other: right-sided, segmental colitis, and postoperative patients (lack of any preoperative medical records for postoperative patients).
Table 2 shows the crude and adjusted ORs and 95% CIs for the association between UC disease activity and constipation. The prevalence of constipation among MH (MES 0), CR, long duration (>7 years), and pancolitis was 8.2%, 13.4%, 12.9%, and 12.5%, respectively. MH, CR, long duration, and pancolitis was not associated with the prevalence of constipation. The prevalence of constipation among age groups, <40, 40–49 years, 50–59 years, 60–69 years, and >70 years was 10.0%, 5.8%, 15.7%, 11.8%, and 25.6%, respectively. Age groups were independently associated with constipation (adjusted OR with age groups, <40, 40–49 years, 50–59 years, 60–69 years, and >70 years: aOR 0.59 [95% CI 0.15, 2.00], aOR 1.65 [95% CI 0.56, 4.87], aOR 1.45 [95% CI 0.44, 0.4], and aOR 3.64 [95% CI 1.26, 10.95], p for trend .001). Only >70 years was independently positively associated with the prevalence of constipation (p = .018).
Crude and Adjusted Odds Ratios and 95% Confidence Intervals for the Associations Between Ulcerative Colitis (UC) Disease Activity and Constipation.
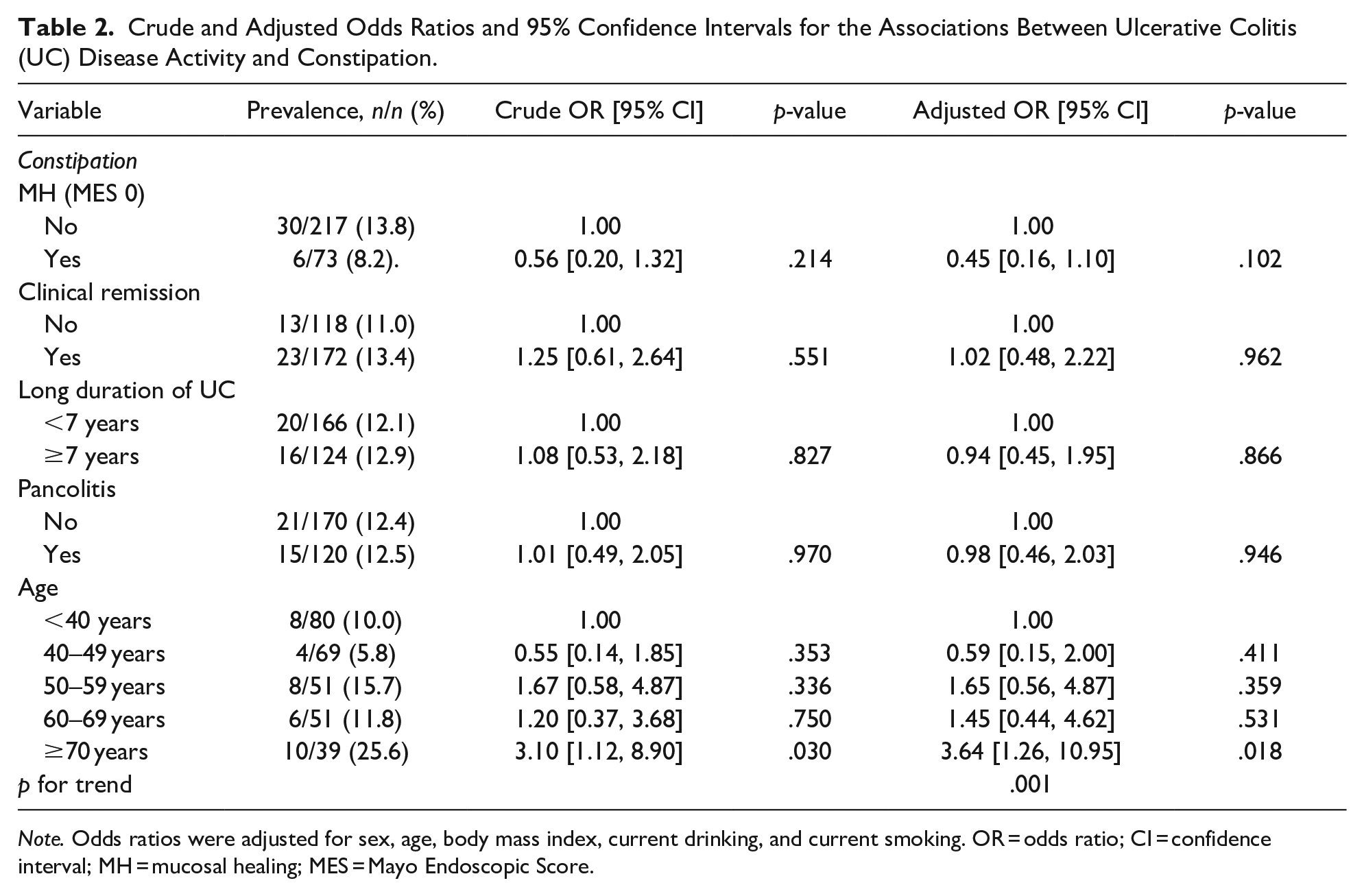
Note. Odds ratios were adjusted for sex, age, body mass index, current drinking, and current smoking. OR = odds ratio; CI = confidence interval; MH = mucosal healing; MES = Mayo Endoscopic Score.
Discussion
This is the first study to investigate the association between disease activity and the prevalence of constipation in Japanese patients with UC. In the present study, aging was significantly positively associated with the prevalence of constipation. However, no association between disease activity and constipation was found in this study population.
Bloody stools and diarrhea are well-known UC-related gastrointestinal symptoms, but some patients also suffer from constipation (James et al., 2018; Lennard-Jones et al., 1962). However, the association between constipation and UC remains inconsistent. The prevalence of constipation was similar between UC and the general population in a US study (Lee et al., 2017). In the present study, the prevalence of constipation might be lower than that in previous research (12.4% vs. 32%–46%) (James et al., 2018; Lennard-Jones et al., 1962). However, the discrepancies between our study and previous studies may be explained, at least in part, by differences in sex, age distribution, definition of constipation, BMI, and treatment of constipation.
In general, aging is associated with constipation (Choung et al., 2007; Higgins & Johanson, 2004; Roque & Bouras, 2015). The findings in the present study are consistent with the results of previous general population studies. Recently, the number of elderly patients with UC has been increasing in Japan (Higashiyama et al., 2021; Shimodaira et al., 2021). Thus, the prevalence of constipation in patients with UC might be increasing in the future. As constipation is associated with poor quality of life, several diseases, and all-cause mortality, healthcare professionals should be aware that UC is associated with a high frequency of constipation, particularly in older patients with UC, regardless of disease activity. In an Australian study of 125 patients with UC, however, age was not associated with constipation (James et al., 2018). It is of note that there are several differences between our study and the previous Australian study, including the ratio of males (57.6%vs. 48.8%), mean age (50.4vs. 47 years), definition of constipation (Rome I criteria and/or medication vs. Rome III criteria), and sample size (n = 290vs. n = 125).
Although the underlying mechanism linking aging and constipation remains unclear, there are several biological plausible possibilities. Age-related changes in physical activity, fluid and food intake, and microbiota (Simrén et al., 2013) may lead to constipation. In previous studies, slow transit constipation represents 15% to 37% of constipated patients (Bassotti et al., 2004; Probert et al., 1994; Surrenti et al., 1995). Older adults have slower colonic transit than younger adults, but there is no difference in gastric emptying capacity or small bowel transit (Madsen JL et al., 2004). In addition, the rectal sensory threshold of older healthy individuals is higher than that of younger healthy individuals (Lagier E et al., 1999). Higher rectal sensory thresholds have also been associated with constipation (Ratuapli et al., 2013). Slower colonic transit and higher rectal sensory thresholds in the elderly may be associated with constipation. Slower colonic transit and higher rectal sensory thresholds in the elderly may be associated with constipation. Thus, aging might cause constipation via some of the mechanisms described above.
This study has several limitations. First, it was a cross-sectional analysis, and therefore, we cannot conclude that there is a causal association between age and constipation. Second, the exclusion rate for this study population was high, resulting in a small sample size. Third, the definition of constipation differed from other papers, as it was extracted using a self-administered questionnaire. However, many other papers have also reported unclear definitions. Fourth, in this study, information was obtained using self-administrated questionnaire but not interviews. These different methods of information acquisition might affect the association between disease activity and constipation. Finally, the subjects of the present study might not be representative of Japanese patients with UC. Nevertheless, the use of prednisolone and biologics was similar between the present study and a Japanese national study based on UC claims data in 2016 (15.5% and 9.0%, respectively) (Matsuoka et al., 2021).
Conclusion
Age may be independently and positively associated with constipation among Japanese patients with UC. In this study, disease activity was not associated with constipation. However, the evidence on this issue is still limited and further larger studies and longitudinal studies are needed in the future.
Footnotes
Acknowledgements
The authors would like to thank Kenichiro Mori, Keitarou Kawasaki, Yuji Mizukami, Satoshi Imamine, Masamoto Torisu, Harumi Yano, Makoto Yano, Masato Murakami, Aki Hasebe, Masumi Hino, and Tomo Kogama.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) and was approved by the Institutional Review Board of the Ehime University Graduate School of Medicine (No. 1505011). Well-trained staff obtained written informed consent from all enrolled patients. The study was registered at each hospital between 2015 and 2019.