
Abstract
A trochanteric fracture is one type of hip fracture. Management of postoperative pain after trochanteric fracture that is caused by decreased gliding between tissues in the lateral thigh is not established. The aim of this study was to examine the effect of compression of the thigh using an elastic bandage on trochanteric fracture after surgery. Multicenter randomized controlled trial was conducted in collaboration with the Comprehensive Rehabilitation Unit (sub-acute rehabilitation Unit) in two hospitals. Eligible volunteers (n = 34) with trochanteric fractures after surgery were randomly assigned to two groups. In the treatment group, participants practiced standing and walking under compression of the thigh with an elastic bandage. The control group was blinded to the intervention and practiced standing and walking under non-compression of the thigh with an elastic bandage. Both groups underwent a standard physical therapy program 2 times a day, daily. Two-way repeated measures of ANOVA showed significant main effect between the groups for gliding between tissue (p < .001), lateral femoral pain (p < .001), subcutaneous tissue thickness (p = .044). Compression of the thigh with an elastic bandage significantly improved subcutaneous tissue thickness, gliding between tissues, lateral thigh pain. Gait velocity improved with these functional improvements.
Introduction
Due to the aging population, prevalence of osteoporosis is rising, and correspondingly, the incidence of fragility fractures are increasing (Tsuda, 2017). The incidence of Hip fractures is increasing every year globally (Gullberg et al., 1997; Hagino et al., 2017; Sambrook et al., 2006); the ability to walk and perform activities of daily living is reduced after a fracture (Kagaya et al., 2005; Tolo et al., 1999). Hip fractures are generally divided into femoral neck fractures (intracapsular fractures) and trochanteric fractures (extracapsular fractures) (Parker et al., 2006). In particular, trochanteric fractures lead to severe functional deficits and gait disorders compared to femoral neck fractures (Fukui et al., 2012; Pfeufer et al., 2019). Physical therapy interventions recommend early ambulation following fractures unless there are surgical limitations (McDonough et al., 2021). However, in many cases, gait is challenging because of pain, which is an important factor affecting gait independence (Münter et al., 2018). Therefore, consideration of postoperative pain when planning interventions is important for patients with trochanteric fractures who have reduced gait ability.
Trochanteric fractures are often treated with intramedullary nails because of their quick operative time and their suitability for unstable fractures (Ma et al., 2014; Shen et al., 2013). In contrast to hip joint surgery with arthroplasty, intramedullary nail procedures have leave the fractured bone in situ (Foss et al., 2009). In other words, there are many free nerve endings distributed at the fracture site (Bjurholm et al., 1988; Mach et al., 2002), and pain of periosteum origin occurs. Postoperative pain after trochanteric fracture is caused by periosteal-related pain associated with inflammation and gliding between tissues in the lateral thigh (Kawanishi et al., 2020). Interventions reported to be effective include transcutaneous electrical nerve stimulation (TENS) for acute pain (McDonough et al., 2021). Cryotherapy can help reduce swelling and pain in knee replacements (Adie et al., 2012). However, the optimal management of gliding between tissues has not been established.
The deep layer of subcutaneous tissue is considered the lubricant adipofascial system and is highly mobile (Nakajima et al., 2004). Skin ligaments connect the skin and fascia (Stecco, 2014). Thickening of the thigh is common with trochanteric fractures (Kazmi et al., 2007). Thickening of the subcutaneous tissue causes excessive movement of the subcutaneous tissue by overstressing the skin ligaments, resulting in a factor that decreases the gliding between the tissues (Kawanishi, Fukumoto et al., 2022). Gliding between tissues on the lateral thigh also affects gait (Kawanishi et al., 2022). These findings suggest that reducing subcutaneous thickness improves gliding between tissues, lateral thigh pain, and gait ability.
Compression with an elastic bandage has been reported to decrease swelling and pain (Schröder et al., 1994). However, the effect of intervention on subcutaneous tissue swelling using elastic bandages on gliding between tissues is not clear. Therefore, we hypothesized that compression of the thigh using an elastic bandage would decrease subcutaneous tissue thickness, and that therapeutic exercise, such as gait under compression, could improve gliding between tissues and lateral femoral pain, leading to an improvement in gait ability. The purpose of this study was to examine the effect of compression of the thigh using an elastic bandage on lateral femoral pain associated with decreased gliding between tissues of the trochanteric fracture after surgery.
Methods
Study Design and Setting
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the ethics committee of the relevant institute (approval number: 2019-087), and eligible patients provided written informed consent. The conduct and reporting of this study were guided by the CONSORT guidelines (Moher et al., 2010). The study was registered at the relevant Clinical Trials Registry before the inclusion of participants (Clinical Trial Registry: Application No. 20191024-133846). This was a parallel-group, multicenter randomized controlled trial with blinded participants and outcome assessor. The study was conducted in collaboration with the Comprehensive Rehabilitation Unit (sub-acute rehabilitation Unit) in two hospitals. The hospitals have 300 and 265 beds respectively. The patient population is a mix of orthopedic and neurosurgical patients. The average length of stay for both is approximately 90 days.
Participants
This study enrolled all participants with trochanteric fractures in the two Comprehensive Rehabilitation Unit. The inclusion criteria were 1) ability to walk before injury; 2) open reduction and internal fixation (Gamma nails) for at least 3 weeks; 3) lateral thigh pain with weight bearing for the study. The exclusion criteria were 1) difficulty walking more than 10 m without assistance by physical therapist; 2) inability to accurately report pain due to severe dementia; 3) absence of Numerical Rating Scale (NRS) lateral femoral pain on loading (NRS < 2); 4) hemiplegia due to stroke; and 5) unwillingness to provide consent for the study. Exclusion criteria were determined according to previous studies (Kawanishi et al., 2022).
Double-Blinded Randomization and Data Collection
Individuals who agreed to participate underwent an initial baseline assessment and were assessed immediately after, 1 week after, and 2 weeks after intervention. All assessments were performed immediately post-intervention. Participant recruitment began in June 2019 and data collection ended in November 2021. The primary outcomes were gliding between tissues, subcutaneous tissue thickness, lateral thigh pain under loading, and gait parameters. The secondary outcomes were lateral femoral pain (Rest/Stretch/Contraction), lower limb muscle strength and lower limb joint range of motion. The following participant characteristics were investigated: age, sex, gait ability before injury (No devices, T-cane, Walker), medical history, fracture type (AO/OTA classification; stable A1/A2.1, unstable A2.2/ A2.3/ A3) (Sabour, 2021), and period from surgery to assessments. This information was obtained from medical records. The permuted block method was used to randomize participants into the control group or the treatment group. An independent researcher not involved with the treatment or outcome measurements implemented randomization. All participants and assessors were unaware of group assignment. One evaluator from each hospital performed the evaluation, including the ultrasound examination.
The sample size for this study was calculated from the gliding between tissues outcomes of the pilot study. The sample size was determined using G Power 3 Software (Version 3.1.9.4; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) using the F test for two-way analysis of variance (ANOVA, power 0.8, effect size 0.4). In total, 32 participants were deemed adequate.
Evaluation of Gliding Between Tissues and Measurement of Subcutaneous Tissue Thickness
Based on previous studies, gliding between tissues was evaluated (Kawanishi et al., 2020, 2022). First, an ultrasonography (Canon Aplio 500; Canon Co. Ltd., Tokyo, Japan/Noblus; Hitachi-Aloka Medical Ltd., Tokyo, Japan) and a linear probe (PLT1204ST; Canon Co. Ltd., Tokyo, Japan/L64; Hitachi-Aloka Medical Ltd., Tokyo, Japan) were used to capture the dynamics of the lateral thigh during −10° extension to 100° flexion of the knee. Next, the gliding coefficient was calculated from the flow velocity in the subcutaneous tissue and the superficial of the vastus lateralis muscle using fluid image analysis software (Flow PIV fluid measurement software; Library Co. Ltd., Tokyo, Japan). A lower gliding coefficient was defined as better gliding between tissues. The measurement of subcutaneous tissue thickness was performed as described in previous studies (Kawanishi et al., 2022), and the subcutaneous tissue was captured at the center of the lateral thigh in the side-lying position with −10° knee extension. The subcutaneous tissue thickness was measured using Image J software (Ver.1.44; National Institutes of Health, Bethesda, MD, USA)
Assessment of Lateral Femoral Pain
Lateral femoral pain (rest, stretch, contraction, weight loading) was categorized according to NRS (0-no pain and 10-very severe pain) (Hawker et al., 2011). Participants were evaluated for stretch pain during range of motion measurement, contraction pain during muscle strength assessment, and loading pain during gait.
Assessment of Gait Parameters
For gait analysis, an inertial sensor (MVP-RF8-HC; MicroStone Corporation, Nagano, Japan, sampling frequency, 100 Hz) was attached to the third lumbar vertebra (McCamley et al., 2012). Thereafter, maximum gait velocity on a 14-m gait path, including a 2-m reserve path in front and behind was measured using stopwatch. Additionally, the initial contact and toe off of the left and right sides of phases 6 to 10 of the gait cycle were identified from the measured acceleration waveform and the tablet (Nexus 7; ASUSTeK Computer Inc., Taipei, Taiwan, sampling frequency, 30 Hz) linked to the inertial sensor. Based on these phases, we calculated the percentage of single-leg and double-support phases on the affected side in one gait cycle. The stride time variability (STV) in phases 6 to 10 of the gait cycle were also calculated. The STV was calculated as the standard deviation of each stride time divided by the mean stride time (Na & Buchanan, 2019). The participants used assistive devices to help them gait as needed.
Assessment of Range of Motion
Bilateral ranges of motion of hip flexion, adduction, and knee flexion were measured using a goniometer to 5° intervals. ranges of motion of hip flexion, adduction, and knee flexion were measured using a goniometer to 5° intervals.
Muscle Strength Assessment
Bilateral muscle strength was evaluated using a hand-held dynamometer (Mobie MT-100; SAKAI Medical Co., Ltd., Tokyo, Japan). The measurement approach was based on previous work (Pfister et al., 2018; Shimizu et al., 2017), and the muscle strength evaluation of knee extension and hip abduction was performed with the participants in the sitting and supine positions, respectively. Each measurement was performed 3 times, and the maximum value (KgF) was used.
Compression Intervention on the Thigh Using Elastic Bandage and Standard Physical Therapy Intervention
In the treatment group, participants practiced standing and walking under compression of the thigh with an elastic bandage (Figure 1). The control group was blinded to the placebo sham compression intervention and practiced standing and walking under non-compression of the thigh with an elastic bandage. Two elastic cotton bandages (Elascot, wide 7.5 cm/length 4.5 m; ALCARE Co. Ltd., Tokyo, Japan) were used in both groups. Both groups performed standing and walking exercises with elastic bandages twice a day, every day (20 minutes × 2 sets). Elastic bandages were applied by the therapist in the participant’s assigned therapist who received instruction. Adverse events from elastic bandage application were identified as needed. In addition, both groups underwent a standard physical therapy program according to guidelines (McDonough et al., 2021) (range of motion exercises, stretching, and strength training) 2 times a day, every day (40 minutes × 2 sets). Elastic bandage compression was applied at maximum intensity without discomfort. The intervening physical therapist confirmed that the participants was able to stand up and gait under an elastic bandage. Adverse events from elastic bandage application were identified as needed. In order to blind the participants to the presence or absence of the intervention, the control group was fitted with elastic bandages without compression. There were no outward differences between treatment and control. The only difference appeared to be the presence or absence of compression under the application of elastic bandages.

Method of wearing an elastic bandage: (a) front side, (b) lateral side, and (c) back side.
Statistical Analyses
The distribution of all data was tested using the Shapiro-Wilk normality test. Baseline participant characteristics between the groups were compared using Mann–Whitney U tests and chi-square tests for categorical variables. Repeated measures of two-way ANOVA were used to determine any significant changes in the tested variables in each group after interventions. Post-hoc analyses with the Tukey method were conducted when there was a significant group-time interaction. In case of an interaction, one-way analysis of variance and post-hoc analyses with the Tukey method were conducted for each factor. Two-way ANOVA and post-hoc analyses with the Tukey method were performed for the ratio scales of gait velocity, subcutaneous tissue thickness, muscle strength, and joint range of motion using the degree of improvement (Value at Post, 1 week, and 2 weeks divided by the value before the intervention). A two-way ANOVA by improvement was performed to adjust for the variability in measurements between groups. All statistical analyses were performed using SPSS Version 24.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < .05.
Results
A total of 137 participants were screened for the trial, of whom 34 were eligible. Of these participants, 18 were assigned to the treatment group; 16 were assigned to the control group. In the control group, 2 participants were lost to follow-up for early discharge and were excluded from the statistical analysis. There were no adverse events. Figure 2 shows the flow of participant enrollment in the study. Participant characteristics and baseline assessments showed no significant differences in any variables between the treatment (Age: 79.7 ± 15.5 years, Sex: 5 male/13 female, Fracture type, stable 11/unstable 7) and control (Age: 85.8 ± 6.5 years, Sex: 2 male/12 female, Fracture type, stable 7/unstable 7) groups (Table 1).

Participant flow diagram.
Participant Baseline Characteristics.

Note. n = number.
Two-way repeated measures of ANOVA for the primary outcome showed significant main effect between the groups for gliding between tissue (p < .001), lateral femoral pain (p < .001), subcutaneous tissue thickness (p = .044), hip abduction muscle strength (p = .018), and knee extension muscle strength (p = .015) (Tables 2 and 3). In addition, two-way repeated measures of ANOVA showed significant interaction between the groups and time for gliding between tissue (p = .003) and pain on loading (p = .021) (Table 2). Repeated one-way ANOVA and post-hoc tests were performed for each of the treatment group and the control group, and significant improvements at all time periods in gliding between tissues were found only in the treatment group (p < .001) (Table 4). Load pain showed a significant improvement in both groups (treatment group; p < .001, control group; p = .003 (Table 4). The treatment group showed improvement at all time points. In contrast, the control group improved only between the pre-intervention and 1 week and between the pre-intervention and 2 weeks. In addition, two-way repeated measures of ANOVA with ratio scales showed that gait velocity also had a significant main effect in the treatment group (p < .001) (Table 5). There were no significant differences between the two groups in terms of other outcomes.
Comparison of Intervention Between Two Groups and Change Over Time in Two-Way Repeated ANOVA With Tukey Post-Test (Primary Outcome).
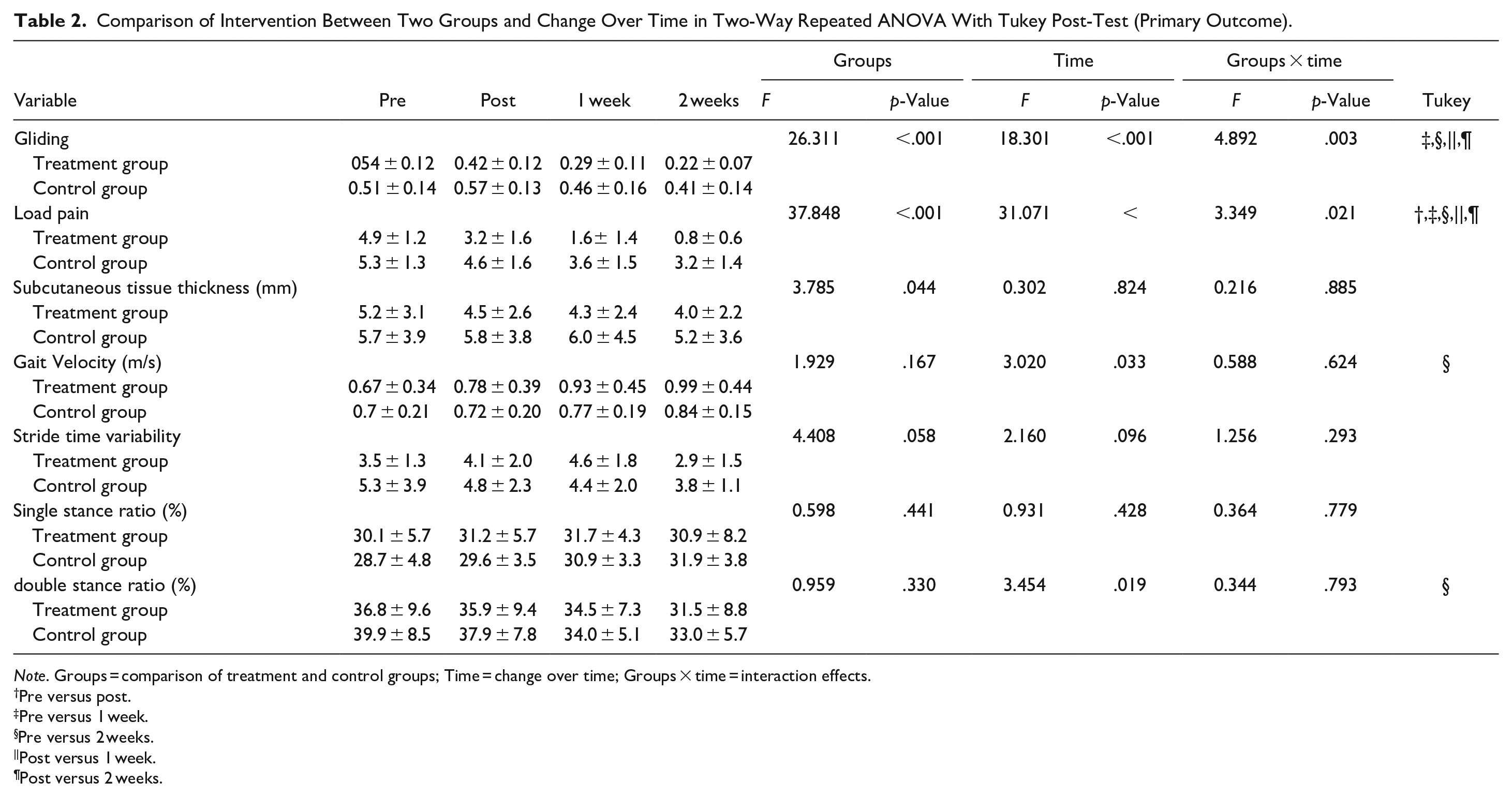
Note. Groups = comparison of treatment and control groups; Time = change over time; Groups × time = interaction effects.
Pre versus post.
Pre versus 1 week.
Pre versus 2 weeks.
Post versus 1 week.
Post versus 2 weeks.
Results of Two-Way ANOVA for Secondary Outcomes.

Note. Groups = comparison of treatment and control groups; Time = change over time; Groups × time = interaction effects.
Pre versus post.
Pre versus 1 week.
Pre versus 2 weeks.
Post versus 1 week.
Post versus 2 weeks.
One-Way Repeated Analysis of Variance (ANOVA) With Tukey Post-test.

Pre versus post.
Pre versus 1 week.
Pre versus 2 weeks.
Post versus 1 week.
Post versus 2 weeks.
Two-Way Repeated Analysis of Variance (ANOVA) With Tukey Post-Test (Ratio Scale).

Pre versus post.
Pre versus 1 week.
Pre versus 2 weeks.
Post versus 1 week.
Post versus 2 weeks.
Discussion
The purpose of this study was to investigate the effect of compression of the thigh using an elastic bandage in trochanteric fracture after surgery. Compression at maximum pressure without uncomfortable of the thigh with elastic bandages twice per day (total 40 minitus) significantly improved gliding between tissues, lateral thigh pain under load, and subcutaneous tissue thickness, hip abduction muscle strength, and knee extension muscle strength. Two-way repeated measures of ANOVA with ratio scales showed that gait velocity also had a significant main effect in the treatment n group. Thus, compression intervention on the thigh using an elastic bandage was shown to be effective in improving impairment and disability after trochanteric fracture.
Interventions for acute pain of lateral thigh after trochanteric fracture surgery have been previously reported. Hip pain and gait ability after trochanteric fracture improved using TENS within 10 days of surgery (Elboim-Gabyzon et al., 2019; Gorodetskyi et al., 2007; McDonough et al., 2021). Cryotherapy for inflammatory pain has also been shown to improve rest pain and movement pain within 2 days of surgery (Adie et al., 2012). However, there is no evidence of intervention for patients with lateral femoral pain after trochanteric fracture in the comprehensive rehabilitation phase (sub-acute rehabilitation phase), when aggressive gait practice is necessary. Kawanishi et al. (2020) demonstrated that pain and gliding are related to inhibitors of gait training. Only fascia manipulation is known to treat gliding (Stecco et al., 2004, 2009), although the effectiveness of this approach has not been verified. Thus, there is no clear consensus on effective physical therapy for lateral femoral pain, gliding, and gait ability in the comprehensive rehabilitation phase (sub-acute rehabilitation phase) of trochanteric fractures. This is the first study to show that physical therapy intervention using elastic bandages is effective for lateral femoral pain and gait disorder.
Compression on the thigh stabilizes the thigh, reduces edema, facilitates proprioceptive sensations, and affects biomechanics during gait (Cheng et al., 2019; Perlau et al., 1995; Schröder et al., 1994). The reduction of edema may be associated with pain reduction by improving circulation and also with a reduction in subcutaneous tissue thickness (Hassan et al., 2002; Schröder et al., 1994; Winge et al., 2017). Subcutaneous tissue thickness is associated with lateral thigh pain under load and gliding between tissues (Kawanishi et al., 2022). The decrease in subcutaneous tissue thickness and fixation of the thigh may have decreased the excessive movement between the subcutaneous tissue and the vastus lateralis muscle. As a result, gliding between the subcutaneous tissue and the vastus lateralis muscle in the lateral thigh improved. Pain reduction and improvement in muscle strength were considered to improve gait velocity. The recovery of pain and muscle strength facilitated gait training and improved gait ability. Femoral compression was found to be effective and noninvasive for trochanteric fractures with lateral femoral pain.
Study Limitations
There are several limitations to this study. We were not able to investigate the long-term process beyond 2 weeks following the intervention, future long-term follow-up should also be investigated. The dynamics of the thigh under elastic bandage compression on the lateral side of the thigh remain unclear. An elastic bandage may help stabilize the joint, but the details are unknown. The compression pressure on the thigh with the elastic bandage is not standardized. Moreover, the minimum compression intensity required to intervene is unclear. The difference in the level of activity (quantity of gait practice) with and without the intervention is unknown. In other words, not all of the effects can be determined to be the result of the compression of the elastic bandage. Future studies should evaluate the efficacy of different materials, such as floss bands (Kaneda et al., 2020), for more effective compression.
Conclusions
Compression of the thigh with an elastic bandage significantly improved subcutaneous tissue thickness, gliding between tissues, lateral thigh pain, hip abduction muscle strength, and knee extension muscle strength. In addition, thigh compression was found to be an effective intervention for improving gait velocity.
Footnotes
Acknowledgements
We thank the staff at the Morinomiya University of Medical Sciences, Kano general hospital, and Higashi Osaka hospital for their detailed comments, suggestions, and constant support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Morinomiya University President’s Research Encouragement Award (Grant Number 2023MPA2).