
Abstract
The objective of this study was to evaluate the reliability and validity of the FES-I scale in community-dwelling older Mexican adults. Participants were 222 older adults, with a mean age of 70 years; 75% were women who completed a sociodemographic data sheet, a Spanish version of the FES-I scale, intended to explore measures of depression, quality of life, and instrumental activities of daily living. Discriminant validity was demonstrated for all items on the FES-I scale and when groups of older adults were compared according to age. Evidence of internal consistency was found in all the items of the FES-I scale (α = .91) and convergent and divergent validity of the FES-I scale with measures of depression and quality of life, except instrumental activities of daily living. The Confirmatory Factor Analysis shows that the FES-I scale partially retains its two-factor measurement properties since five items were removed from the model to fit the data. The FES-I scale is a valid and reliable measure for clinical evaluations of fear of falls in older Mexican adults in the community.
Applications of study findings
The exploration of other medical or psychosocial variables related to the fear of falling in Mexico.
Effective ways to evaluate clinical interventions aimed at reducing fear of falls in Mexico.
Introduction
Increasing longevity in Latin America, as elsewhere, introduces new challenges to health and research policies. According to the United Nations, the population aged 60 years and over is expected to increase from 10% to 20% during the period from 2010 to 2040 in the Latin American and Caribbean regions, making aging a priority on the public agenda (Cruz et al., 2014; Instituto Nacional de Geriatría [INGER], 2022; Marques-Vieira et al., 2016).
According to the National Center for Preventive Programs and Disease Control (Centro Nacional de Programas Preventivos y Control de Enfermedades [CENAPRECE], 2017), falls are one of the main geriatric syndromes, with the age of the person being one of the determining factors for this phenomenon. According to the World Health Organization (WHO, 2021), falls are defined as: “. . .an event which results in a person coming to rest inadvertently on the ground or floor or other lower level.” WHO (2021) figures indicate that falls are the second leading cause of death from unintentional injuries worldwide. Likewise, it calculates that about 684,000 people around the world die annually due to these, with people over 60 years of age suffering the most from these events.
According to data from the Health, Well-being and Aging Survey (SABE), carried out in 14 states of the Mexican Republic (Baja California Sur, Campeche, Durango, Guanajuato, Jalisco, Michoacán, Morelos, Querétaro, Quintana Roo, San Luis Potosí, Sinaloa, Sonora, Tamaulipas and Yucatán), the point prevalence of falls in the people interviewed was 26.5%, a trend that increases with age. Likewise, it points out that about 15% of falls in the older adult population cause serious damage and require medical treatment, of which 10% suffer complications due to head injuries, extensive skin bruising, soft tissue or musculoskeletal injuries (CENAPRECE, 2017).
It has been documented that the main consequences of falls are fractures (mainly hip), immobility, reduction in activities of daily living (ADL), and fear of falls (also called Post-Fall Syndrome or Ptophobia) (Beltrán, 2002 in CENAPRECE, 2015, 2017; Cruz et al., 2014; Secretariado Técnico del Consejo Nacional para la Prevención de Accidentes, 2016).
The fear of falling is a common concern among older adults, which can significantly impact their daily lives. This fear often leads to activity restriction and a perceived decrease in overall quality of life. Furthermore, individuals who experience this fear may also increase their use of medications, further exacerbating the problem. In spite of the fact that fear of falls is a prevalent issue, different studies define it differently, leading to widely differing estimates of its prevalence. These rates range from 12% to 92%, indicating that there is no consistent understanding of this issue. Establishing a consistent measurement methodology would improve understanding and interpretation of findings related to fear of falling, as well as in epidemiological studies, in the latter in order to identify those older adults with excessive fear of falling who require intervention, as well as to determine which activities cause greater fear and consequently set a starting point in rehabilitation (Delbaere et al., 2010; Yardley et al., 2005).
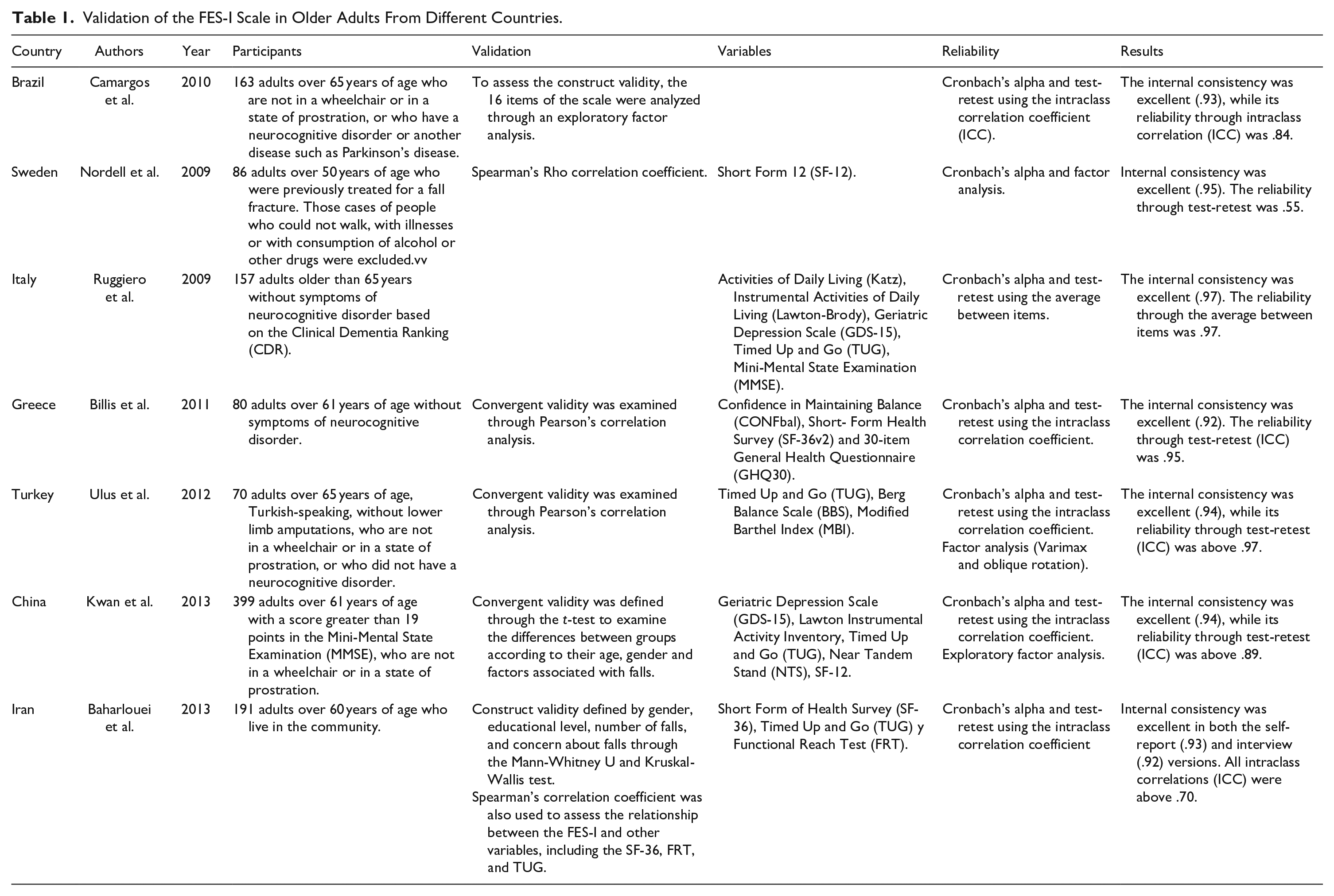
The Falls Efficacy Scale-International (FES-I) was developed and validated in 2005 by Yardley et al. (2005), seeking to improve the methodological and cultural deficiencies of a previous version called the Falls Efficacy Scale (FES), designed by Tinetti et al. (1990). This new version (FES-I) adds six items to the original scale, focusing on more complex ADL and on the social aspects of falls. Today, the scale has been translated and validated in various countries around the world (Germany, the Netherlands, the United Kingdom, Sweden, Italy, Brazil, Australia, Greece, Turkey, China and Iran). In all of them, the scale has shown an internal consistency considered from good to excellent (α ≥ .90) (Marques-Vieira et al., 2016). Table 1 describes different validation studies of the FES-I scale.
Validation of the FES-I Scale in Older Adults From Different Countries.
No validation of the FES-I scale in Mexico is reported in the literature, therefore, based on the international recommendation to adapt and validate measures in different cultures, this study aimed to evaluate the reliability and validity of the FES-I scale in community-dwelling older Mexican adults. In this context, the research question in this study was: What is the validity and reliability of the FES-I scale to measure fear or concerns about falls in older adults recruited in meeting centers and living in the community? Figure 1 details the steps that were followed for the validation of this instrument.

Steps for the validation of the Falls Efficacy Scale—International.
Methods
Participants
In this study, 222 older adults between 60 and 92 years of age participated, with an average age of 70 years, 75% are women, 49% married or with a partner, and 30% with high school studies or higher (<9 years of education). The participants were recruited in gerontological centers belonging to the state of Hidalgo and Sonora, Mexico. The authorities of each meeting center were contacted to obtain access to the older adults.
Measures
The Falls Efficacy Scale-International (FES-I) is a self-applied scale that assesses the level of concern about falling while performing various instrumental activities of daily living (IADL). The questionnaire consists of 16 items with four response levels (1 = “Not at all concerned”, 2 = “Somewhat concerned”, 3 = “Quite concerned”, 4 = “Totally concerned”), with a score range of 16 to 56 points. Delbaere et al. (2010) established the following cut-off points: Low concern: 16–19 points; Moderate Concern: 20–27 points; High Concern: 28–64 points).
The WHOQOL-OLD Quality of Life Questionnaire is a Likert-type scale consisting of 24 items scored in a range from 1 to 5 and which consists of six dimensions, each with four items: “Sensory abilities,” “Autonomy,” “Past, present and future activities,” “Social participation,” “Intimacy” and, “Death and dying.” The score for each dimension varies between 5 and 20 points, while the overall score ranges from 24 to 130 points. According to the validation of the WHOQOL-OLD (Acosta-Quiroz et al., 2013), the higher the score, the higher the quality of life. This questionnaire was used since it addresses relevant life situations in old age, where the impact of concerns about falls in older adults can be reflected.
The Yesavage Geriatric Depression Scale (GDS-15) assesses depressive symptoms through 15 dichotomous items. The maximum score on the scale is 15 points, adding one point for each affirmative answer. According to the validation (Acosta-Quiroz et al., 2021), a score greater than or equal to 5 points indicates the presence of depressive symptoms.
The Lawton Instrumental Activities Scale evaluates the degree of independence of the older adult for the execution of IADL. Regarding the interpretation of the scores, INGER (2020) refers that the maximum score is eight, while the minimum score is zero. On some occasions, older adults have not carried out certain activities in their lives (e.g., cooking); in this case, the activity is omitted, giving a total score of 7. This scale was used since the measurement of activities of daily living is the cornerstone in the evaluation of autonomy and functional status of older adults, and where concerns about falls are expected to affect.
A sociodemographic data questionnaire developed ad hoc to collect the following data: age, gender, diseases, education, marital status, occupation, and number of previous falls.
Procedure
The translation of the FES-I scale was carried out through the protocol established by the ProFaNE (Prevention of Falls Network Earth) working group, where the key points for its realization are indicated. The translation and re-translation process is briefly outlined below:
The English version of the 16-item FES-I scale, developed by Yardley et al. (2005), was initially used.
A first translation into Spanish was carried out by two independent translators, both native speakers familiar with the concept of “fear of falls.”
A first consensus was reached through a meeting with translators, to come up with a first translated version.
Four older adults participated in the application, and they were consulted about the clarity of the articles and the possible need for reformulation.
Modifications were made according to the comments of the older adults to the first translated version.
A second meeting was held with the translators, in order to discuss the modifications and to elaborate a second translated version.
A further translation of the second version of the scale was provided by a translator whose native language is English.
A third consensus meeting of the translators was held to discuss the re-translation. A local version in Spanish was obtained from this third meeting.
The translated FES-I scale and the measures of depression, quality of life and IADL were administered by the authors, as well as by health personnel in meeting groups of older adults in different cities of Mexico. The data of the participants were analyzed using the SPSS Statistics software in its version 21. Data analyzes were carried out to assess the discriminant validity of the FES-I scale in all its items. Groups of older adults were also compared according to variables such as age, sex, and frequency of falls in the last 6 months, using the t-test for independent samples in order to make comparisons of means. Similarly, Cronbach’s alpha coefficient was used to evaluate the internal consistency of all the items in the FES-I scale and Spearman’s Rho correlation coefficient for convergent and divergent validity of the FES-I scale with measures of depression, quality of life and IADL. Finally, a Confirmatory Factor Analysis (CFA) was performed to test the measurement model of the FES-I scale using the Root Mean Square Error of Approximation (RMSEA), the Goodness of Fit Index (GFI), the Comparative Fit Index (CFI), the Incremental Fit Index (IFI), and the Tucker Lewis Index (TLI).
These item analyzes were used based on the suggestions of classical measurement theory about obtaining evidence of discriminant, convergent, and divergent validity, according to criteria external to the theory, which reinforce the construct validity of the FES- I scale, as well as the internal consistency of the items that make it up, as suggested by the domain-sample model, which indicates that the items that make up the scale must be strongly related to each other, since they measure the same construct. The CFA provides the final evidence needed to establish that the FES-I scale has theoretical strength and measures what it purports to measure.
Results
The objective of this study was to evaluate the reliability and validity of the FES-I scale in community-dwelling older Mexican adults. The discriminant validity of the FES-I scale, Table 2 shows that all the items discriminate individually between those participants who obtained high scores from those who obtained low scores on the FES-I scale. Scores obtained in the other administered measures are found in Table 3.
Items That Discriminate Between Participants With High Scores and Low Scores on the FES-I Scale (n = 222).

Scores Obtained in the GDS-15, Lawton Scale and WhoQoL-OLD.

Discriminant validity was also evaluated through contrasted groups, comparing the means of the scores of the FES-I scale in relation to sociodemographic variables such as age (less than 75 years vs. 75 years and over), sex (men vs. women), and if they have suffered one or more falls in the last 6 months (Table 4).
Discriminant Validity of the FES-I Scale.

p ≤ .05.
Regarding the reliability of the FES-I scale, internal consistency was obtained through the Cronbach’s Alpha coefficient of α = .916 in all the items. Table 5 shows the “Corrected item-Total correlation” and “Alpha if item deleted” in each of the items.
Reliability of All the Items of the FES-I Scale (n = 222).

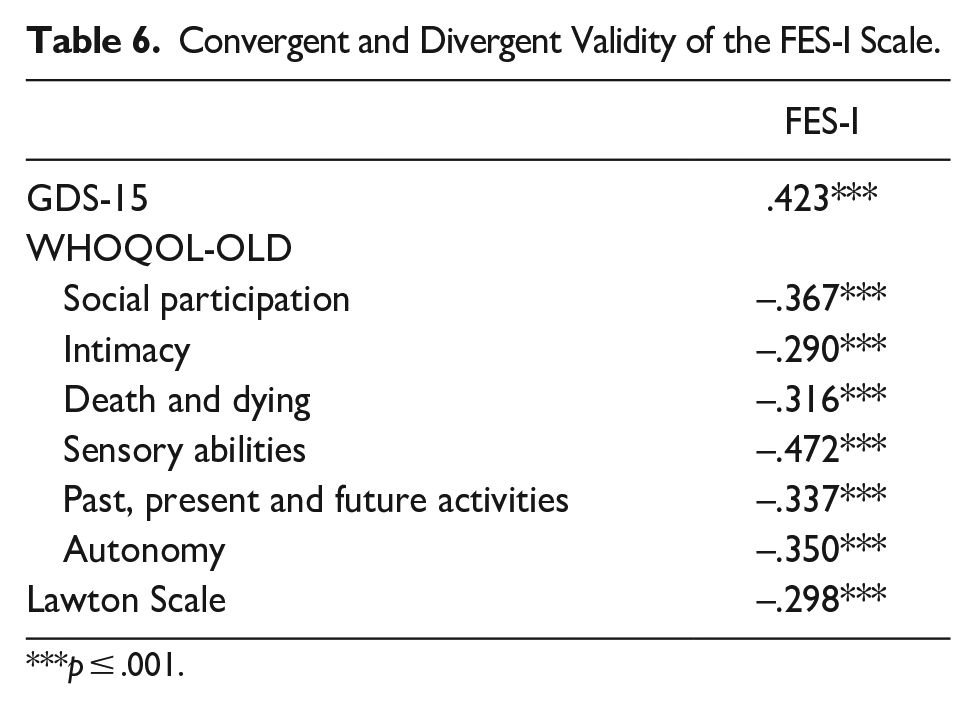
Similarly, convergent validity was evaluated through Spearman’s Rho correlation coefficient, between the total scores of the participants on the FES-I scale and the Geriatric Depression Scale (GDS-15). Divergent validity also was evaluated through the correlation between the scores of the FES-I scale, the WHOQOL-OLD dimensions and the Lawton Instrumental Activities Scale (Table 6).
Convergent and Divergent Validity of the FES-I Scale.
p ≤ .001.
Finally, a CFA was carried out considering that in the original version of the FES-I scale (Yardley et al., 2005), two factors are indicated: “Concern for low-demand activities” and “Greater physical demand outside the home.” Items belonging to Factor 1 are: 1, 2, 3, 4, 5, 6, 7, 10, 12, and 16. Items belonging to Factor 2 are: 8, 9, 11, 13, 14, and 15. The indices of fit of the measurement model in the FES-I scale are RMSEA: .059, GFI: .940, CFI: .967, IFI: .968 and TLI: .958. Figure 2 shows the final measurement model that best fits the data, where five items from the FES-I scale were removed.

Final measurement model of the FES-I scale.
Discussion
The objective of this study was to evaluate the reliability and validity of the FES-I scale in community-dwelling older Mexican adults. Referring to discriminant validity, Table 2 shows evidence that all the items of the FES-I scale are sensitive to distinguish between those older adults who have high concerns about falls from those who have low concerns. It is important that the FES-I scale can identify older adults with high concerns about falls, due to their relationship with the deterioration in well-being. Psychosocial care in older adults should include the assessment of concerns about falls.
Similarly, Table 4 shows differences in terms of concerns about falls between participants under and over 75 years of age, which contrasts with what was reported by Chan et al. (2018), who found no differences according to these age groups. This can be interpreted as a directly proportional relationship between age and concerns about falls, indicating a greater perception of frailty with advancing age. These same authors found differences in concerns about falls between men and women, and between those who had not suffered a fall and those who had fallen at least once in the last year. In the current study, no differences were found according to sex and falls in the last 6 months.
The internal consistency of all the items on the FES-I scale coincides with that reported internationally by Camargos et al. (2010), Nordell et al. (2009), Ruggiero et al. (2009), Billis et al. (2011), Ulus et al. (2012), Kwan et al. (2013), Baharlouei et al. (2013). Table 5 shows in the column referring to the correlation of each individual item with the rest of the items, and in the column referring to if item is deleted, that the items of the FES-I scale show high correlations among themselves, which is evidence of a strong internal consistency in the structure of the FES-I scale. Therefore, the FES-I scale is reliable.
Table 6 shows that the FES-I scale has convergent validity with depressive symptoms, as reported by Chan et al. (2018), and divergent validity with sensory abilities, which can be interpreted as the fact that concerns about falls affect the mood of older adults, with a negative impact on well-being and quality of life. However, these same authors report divergent validity of the FES-I scale with IADL measures. In this study a low correlation was identified between concern about falls and the performance of instrumental activities. This indicates that concerns about falls can have a psychological impact on the mood of older adults, but it does not affect the performance of IADL.
Although the existing literature on anxiety and its consequences in the older adults indicates a negative impact on carrying out IADL (Brouwer et al., 2004; de Beurs et al., 1999), various studies have indicated a minimal relationship in carrying out activities due to fear of falls. According to Howland et al. (1998), fear of falls has defined three subpopulations: those who are not afraid of falls, those who are afraid of falls but do not restrict their activities because of their fear, and those who are afraid and restrict valued activities. The findings in our study are consistent with those of Howland et al. (1998), where neither worry about falling nor the experience of falls were associated with activity restriction, mainly due to the presence of social support.
Finally, in Figure 2 the CFA shows that the FES-I scale partially preserves its measurement properties, since it was necessary to remove five items with high error components so that the measurement model would fit the data, considering the two factors proposed in the literature. Similarly, other studies have found valid fit indices considering a single factor and in versions of the FES-I scale with seven items (Norouzi et al., 2023) and with images (Moreira et al., 2020).
There are several considerations that should be taken into account when applying the FES-I Scale. First of all, it is important to consider the educational level of the older adults evaluated. If the FES-I Scale is administered to people with low levels of education, it may be necessary to provide additional explanations or examples to ensure that they understand the questions being asked.
Likewise, it is necessary to consider the health conditions that prevail in the Mexican older adult population. For example, conditions like osteoporosis and diabetes can affect a person’s fear of failure and their ability to complete certain activities. Therefore, it may be necessary to adapt the FES-I questions or scoring criteria to better reflect these specific health problems. It should be mentioned that the difference in proportions between the sexes is mainly explained by cultural factors associated with the use of time in the older Mexican population (Carmona & Ribeiro, 2010).
Conclusion
It is concluded that the FES-I scale is reliable and valid for its application in community-dwelling older Mexican adults. This opens the possibility of lines of research in Mexico where an important clinical value is given to concerns about falls in older adults and the impact that these have on the mood and daily functioning of older adults. Even more, to evaluate the effects of psychological interventions with the aim of reducing the negative impact of concerns about falls on the quality of life and well-being of older Mexican adults.
Footnotes
Acknowledgements
We would like to thank the Institute for the Care of Older Adults of the State of Hidalgo (IAAMEH) and the National Institute for Older Adults (INAPAM) for their support in carrying out this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was carried out with the support of a maintenance scholarship from the National Council of Humanities, Sciences and Technologies (CONAHCYT), number 919084.
Institutional Review Board
This study was reviewed and approved by the Institutional Ethics Committee of the Instituto Tecnologico de Sonora (ITSON), on July 6, 2022 in Dictamination #175.