
Abstract
In this study, we aimed to determine the association between health literacy and the development of cardiovascular diseases (CVDs), among an older population. This cross-sectional study was conducted among Japanese health management specialists (N = 593). Higher levels (communicative and critical) of health literacy and CVD risk factors (diabetes mellitus, hypertension, dyslipidemia, and obesity) were measured. The mean patient age was 71.3 years. Logistic regression analyses showed statistically significant associations between higher levels of health literacy and the prevalence of CVDs (β coefficient = −.091, p < .05) and metabolic risk factors (β coefficient = −.084, p < .01). There was a statistically significant association between health literacy and the count of CVDs (and its risk factors) (β coefficients of Poisson regression = −.036, p < .05). The results show health literacy to be fundamentally related to low prevalence of cardiovascular diseases and their associated metabolic risk factors.
Keywords
Introduction
Cardiovascular diseases (CVDs), predominantly stroke and ischemic heart disease (myocardial infarction and angina), are the leading cause of morbidity and mortality worldwide. CVDs negatively impact quality of life and are highly prevalent among the older population (Zhou et al., 2022). Therefore, CVDs place a social and economic burden on older adults (Kubota, 2020; Lozano et al., 2012; Zhou et al., 2022). Japan is one of the most rapidly aging countries worldwide, and approaches to geriatric disease prevention is of national interest (Noji & Daida, 2017; Tsuji, 2020; Yasuda et al., 2018).
Health literacy is defined as the ability to find, understand, evaluate, and use health-related information (Sørensen et al., 2012). Health literacy has been investigated extensively in many fields and has been reported to influence health behaviors (Smith et al., 2015), disease screening and development (cancer (Morris et al., 2013; Oldach & Katz., 2014), heart failure (Cajita et al., 2016), diabetes mellitus (Al Sayah et al., 2013)), medical costs (Howard et al., 2005), and the understanding of medical conditions (Van der Heide et al., 2013). A large majority of health literacy studies have been conducted in clinical settings rather than in a community-based population (Magnani et al., 2018). It is believed that health literacy intervention can improve health outcomes; however, only a few studies have demonstrated a causative relationship between health literacy and health outcomes (Albus, 2018; Visscher et al., 2018; Walters et al., 2020).
Furthermore, it has been reported that health literacy has an important role in the primary and secondary prevention of CVDs (Chesser et al., 2016). However, only a few studies have reported on the association between health literacy and the development of CVDs (and their associated metabolic risk factors) in the older population. Thus, little is known about the association between health literacy and lifestyle-related diseases in older individuals (Geboers et al., 2016).
Therefore, in this study, we aimed to determine the association between health literacy and CVD development in an older population of health management specialists. In addition, this study aimed to provide important insights to guide CVD public health practices and risk factor prevention in the older population.
Methods
Study Design
A cross-sectional study design was employed, and surveys were completed by health management specialists. The survey consisted of health literacy questions. In addition, using questionnaires, we surveyed the current risk factor status and history of CVDs, including stroke and coronary heart disease. All questionnaires were administered at the time of enrollment.
Study Participants
Study participants were health management specialists certified by the Japanese Association of Preventive Medicine for Adult Disease (JAPA, 2021). The program was sponsored by the Ministry of Education, Culture, Sports, Science, and Technology of Japan. Health management specialists were certified through multiple courses of study. The candidates studied various topics throughout the course, including health promotion, lifestyle-related diseases, mental health, nutrition, environment and health, physical activity and exercise, emergency medicine, life support, and the healthcare system. To qualify and register as a health management specialist, candidates were required to pass the final written examination. The certified specialists were expected to engage with their residential communities and conduct health promotion workshops.
The specialists were contacted, via mail, to participate in the study, which was distributed on August 1, 2020. The following inclusion criteria were used: age 65 or older, continuing participation in professional education (active specialists), and provision of written informed consent. Specialists who did not engage in continuing education or health promotion activities were excluded. Among individuals who met the inclusion criteria (n = 1,142), 593 agreed to participate in the survey.
Variables and Measurements
Demographic data including education, marital status, income, and perceived stress and health literacy were collected. Stress was asked in the questionnaire and assessed to use 4-point Likert scale from none, low, moderate, to high. Education level was determined as junior high school, high school, college, university/graduate school. Income was asked and categorized into three-group; less than 2.0, 2.0 to 6.0, more than 6.0 million yen per year. Health literacy was measured using the communicative and critical health literacy (CCHL) scale (Ishikawa et al., 2008). We also used self-administered questionnaires to record the presence of CVD risk factors, including diabetes mellitus, hypertension, and dyslipidemia, as well as history of CVDs, including stroke and coronary heart disease. The questionnaire requested that the current use of medications be listed. Presence of CVD risk factors was determined from the current disease status of each study participant, use of medications for diabetes mellitus, hypertension, and dyslipidemia, or health maintenance exam results (hypertension, systolic BP > 140 mmHg or diastolic BP > 90 mmHg, diabetes; HbA1c > 6.5% or glucose > 200 mg/dL, dyslipidemia; LDL cholesterol > 140 mg/dL or HDL cholesterol < 40 mg/dL).
Analysis
Descriptive statistics (mean, average, standard deviation [SD], and range) were used to describe the characteristics of the study participants. Multiple logistic regression tests were performed to determine the presence of CVDs and their risk factors based on health literacy. The CCHL scale was used separately for the logistic regression analysis as an independent variable. Three different logistic regression models were fitted with adjustments for covariates. The first model (Model 1) was a simple logistic regression to explain the risk factors for CVDs (hypertension, diabetes mellitus, and dyslipidemia) and CVD history by health literacy with no covariates. The second model (Model 2) included sex, income, education, and marital status as covariates. In addition to the covariates in the second model, the third model (Model 3) included the psychological factor, stress perception, as a covariate. Poisson regressions were also performed to explain the counts of risks and CVDs by health literacy, using the same covariates as in the logistic regressions. A p value less than .05 was considered statistically significant. All statistical tests were two-tailed. All statistical analyses were performed using IBM SPSS Statistics (Version 26.0. Armonk, NY, USA). This study was approved by the Ethics Committee of Saitama Medical University (ID 926, 2020).
Results
A total of 593 certified health management specialists were included in this study. A larger number of women (N = 299; 50.4% vs. men [N = 294; 49.6%]) participated in the study. The age of the study participants ranged from 65 to 93 years. The average age of the participants was 71.3 with a standard deviation of 5.13 years. Eighty two percent of the participants were married and 64.2% received higher education. The average and SD of the CCHL score were 19.0 and 3.8, respectively. Table 1 presents the demographic characteristics of the study participants.
Characteristics of the Study Participants.

Logistic regression analyses showed a statistically significant association between health literacy, measured by the CCHL, and the prevalence of metabolic CVD risk diseases, including diabetes mellitus, hypertension, dyslipidemia, and obesity, after adjusting for confounding factors. The odds ratio for these metabolic risk factors was 0.92, with a one-point increase in the CCHL score after adjusting for sex, education, marital status, income, and stress. Table 2 shows the β coefficient, odds ratio and p value for all logistic regression models.
Multiple Regression Analyses using CCHL Scale and Metabolic CVD Risk Factors.
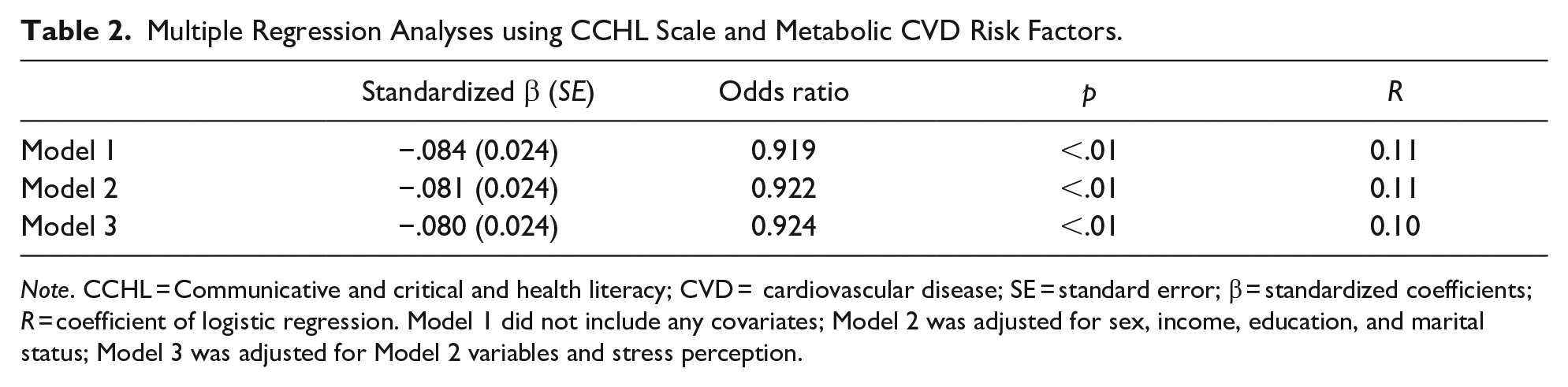
Note. CCHL = Communicative and critical and health literacy; CVD = cardiovascular disease; SE = standard error; β = standardized coefficients; R = coefficient of logistic regression. Model 1 did not include any covariates; Model 2 was adjusted for sex, income, education, and marital status; Model 3 was adjusted for Model 2 variables and stress perception.
Logistic regression analyses showed a statistically significant association between health literacy, as measured by the CCHL, and the prevalence of CVDs, including stroke and coronary heart disease, after adjusting for confounding factors. The odds ratio for these metabolic risk factors was 0.92, with a one-point increase in the CCHL score after adjusting for sex, education, marital status, income, and stress. Table 3 shows the β coefficient, odds ratio and p value for all logistic regression models.
Multiple Regression Analyses Using CCHL Scale and Total Health-Related Lifestyle Score.

Note. CCHL = Communicative and critical health literacy; SE = standard error; β = standardized coefficients, R = coefficient of logistic regression. Model 1 did not include any covariates; Model 2 was adjusted for sex, income, education, and marital status; Model 3 was adjusted for Model 2 variables and stress perception.
Poisson regression analyses showed a statistically significant association between health literacy, as measured by the CCHL and the number of CVDs and their associated risk factors. The β coefficients of the Poisson regression models of 1, 2, and 3 were −0.036 (p < .05), −0.033 (p < .05), and −0.033 (p < .05), respectively.
Discussion
We found that health literacy measured with a widely used validated tool was associated with the prevalence of CVDs and their risk factors in a community-based older population of healthcare management specialists. A significant association between health literacy and the prevalence of CVDs and their risk factors has been reported in other populations, including the general population (Albus, 2018). However, to the best of our knowledge, this is the first study to show that health literacy is associated with both CVDs and their risk factors, among the older community-dwelling older Japanese population. The results validate the evidence that health literacy plays an important role in CVD development. In addition, health literacy is associated with CVD risk factors such as hypertension, diabetes, obesity, and dyslipidemia. These results provide scientifically meaningful insights. Several studies have shown an association between health literacy and CVDs or risk factors in a community-based population (Aaby et al., 2017; Diederichs et al., 2018; Lindahl et al., 2020; Tiller et al., 2015; Yokokawa et al., 2016). However, the results of studies investigating the relationship between health literacy and CVDs or its risk factors are inconsistent. Tiller et al. (2015) reported that health literacy was associated with diabetes mellitus and stroke but not with blood pressure. Another study reported no association between health literacy and blood pressure, despite the positive association between health literacy and self-reported CVDs (Ricardo et al., 2014). These differences may be attributed to variations in race or age among the investigated population groups. In addition, the relation between health literacy and CVDs and the risk factors might be mediated and/or moderated through multiple pathways such as choice of lifestyle, access to care and providers, medication adherence, and healthcare system (Goto et al., 2019; Kalichman et al., 2008; Lindquist et al., 2011; Yokokawa et al., 2016). Since the study population is largely well-educated and specialized in health management, these factors can mediate and/or moderate the effect of health literacy on CVD and risk factors through these factors among the health professional. While the results of our study support the evidence that health literacy is associated with CVDs and their risk factors among community-dwelling older adults with specialty in health management, the causal relationship between health literacy and CVDs or risk factors needs to be studied further. Nevertheless, the current study results increase the generalizability of existing evidence to a wider ethnic and age range.
Diseases including hypertension, diabetes mellitus, and dyslipidemia are established risk factors for CVDs among community-dwelling populations, as reported previously (Mendis, 2010; O’Donnell et al., 2016; Yan et al., 2017; Yusuf et al., 2004). We observed that health literacy was associated with CVDs and their risk factors. Thus, health literacy may mediate or moderate the causative relationship between CVDs and their established risk factors. Baker et al. (2007) showed that CVD-related mortality rates were higher in patients with poor health literacy; this was due to several factors, including poor health behaviors. In addition, it was previously reported that higher mortality rates are observed among individuals with poor health literacy, which can be attributed to poor health behaviors (due to a lack of knowledge) and subsequent disease development, such as the development of CVD risk factors (Mayberry et al., 2018). It is of great scientific interest to further investigate health literacy as a causative factor for the development CVD risk factors (such as hypertension, diabetes mellitus, and dyslipidemia), and ultimately CVDs.
Several studies have shown that health literacy can be improved through interventions. It has been shown that improved health literacy positively influences health outcomes. Health behaviors, such as smoking, poor diet, and physical inactivity cause CVD risk factors, including hypertension, diabetes mellitus, and dyslipidemia, which leads to stroke, coronary heart disease, and atherosclerosis. These results indicate that health literacy may be a causative factor for the development of CVD risk factors, and ultimately CVDs. In addition, CVDs are prevalent among the older population, whose health literacy may be lower than that of the younger population (Patel et al., 2011; Wolf et al., 2010). While robust evidence is required to confirm that health literacy interventions improve CVD outcomes, the current evidence suggests that health literacy prevents the development of several diseases, including CVDs and their risk factors, and therefore has the potential to decrease the diseases-associated economic burden in an aging society.
Our study has several strengths. First, health literacy was measured using a previously validated and widely used tool, the CCHL scale. This scale is relatively easy to use in research and daily clinical practice. It allows investigators and clinicians to measure health literacy in a wide variety of settings. Second, our study measured the prevalence of CVDs and its risk factors among community-dwelling older individuals. The consistency of the results showing that health literacy was related to both CVDs, and their established risk factors sheds light on the biological plausibility of the effect of health literacy on CVD development, in the older population. Health literacy influences CVD risk factors, which ultimately influences CVD incidence, therefore health literacy influences CVD development in the older adults. However, causality needs to be confirmed by longitudinal studies in the future. Additionally, the study participants are specialists in health management. There were studies to show the necessity among healthcare professional to increase awareness the health literacy (Alsubaie et al., 2019; Mor-Anavy et al., 2021). The study results may assist the notion that improving health literacy among health professionals benefit not only for patients but themselves. Finally, the age range of our study participants was wide, 65 to 93 years, which increases external validity.
This study has a few limitations. First, it did not involve random population sampling. Convenience sampling, which was used here, may not allow the application of the results to the general population of older adults. Generalizability to other populations or to the general population requires a more robust sampling methodology, which is our future target. Second, the measurements were self-administered and may have included reporting bias.
Conclusions
High-levels of health literacy is fundamentally related to a low prevalence of cardiovascular diseases and metabolic risk factors, such as diabetes mellitus, dyslipidemia, and hypertension among the older adults with specialty in health management. Health literacy may be a practical target for preventing CVDs and lowering the societal and economic burdens of a rapidly aging society.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Grant-in-Aid for Young Scientists (JSPS KAKENHI Grant Number JP20K19645).
Ethical Approval
This study was approved by the Ethics Committee of Saitama Medical University (ID 926, 2020).