
Abstract
Introduction
The United States’ population median age has been increasing: in 2016, US residents over age 65 were almost 50 million of the population, a significant increase of over 40% since 2000 (US Census Bureau, 2017). Each year, approximately one-quarter of community-residing older adults 65 years of age and older, and half of those over age 80, experience a fall (Burns et al., 2022, 2010). Fall related injuries are the major cause of accidental death and disability among older adults. Alarmingly, the rate of fall-related mortality has recently increased over 30% between 2007 and 2016 (Burns & Kakara, 2018). Further, falls remain the most common cause of nonfatal injury in the United States (Centers for Disease Control & Prevention, 2022), and fall-related hip fractures are a major contributor to morbidity. The number of hip fractures in the US is projected to reach 840,000 annually by the year 2040, and worldwide, the number is expected to surpass 6 million by 2050 (Kannus et al., 1996). Additionally, hip-fracture related mortality is significant, with reported 1-year mortality of 20% to 30% (Brauer et al., 2009; Schnell et al., 2010) and among those who survive, approximately half are never able to regain the ability to live independently (Morrison et al., 1998).
Identification of risk factors and referral to/participation in appropriate fall-risk reduction programs are established as an effective, evidence-based approach to reduce falls (Burns et al., 2022). Specifically, targeted strength and balance exercises have consistently been shown to improve fall risk, and accordingly, the Centers for Disease Control and Prevention (CDC) has outlined an evidence-based clinical approach to identify those at risk for falls. The toolkit is able to assess known fall risk factors and provide a gauge for which to refer those to community-based fall-prevention programs (Sarmiento & Lee, 2017; Stevens & Phelan, 2013). However, this CDC resource and workflow has been slow to penetrate in routine clinical practice, as physicians report barriers to implement comprehensive falls-prevention screening because of time constraints, poor reimbursement for falls screening, and existing toolkit utilization does not easily fit into a Medicare wellness visit (Casey et al., 2017). Because of this, only approximately one-third of older adults report being asked about fall risk, and similarly only around one-third of those who fall report discussing this with their healthcare provider (Stevens et al., 2012; Wenger et al., 2003).
Shared medical appointments (SMA) have shown promising outcomes in geriatric populations, including in fall prevention (May et al., 2014), and have the potential to create sustainable workflows to be incorporated within medical practices. These programs have the potential to be highly impactful for patient education and screening for fall risk reduction, and ultimately in reducing falls in older adults. We therefore aimed to establish a workflow using SMA to comprehensively screen and evaluate fall risk, and to provide medical advice and community resources or clinical referrals based on fall-risk assessment. A secondary aim was to improve our understanding of patients’ experience through this clinic model, including their acceptability of the SMA and nurse visit, and their use of educational materials and similar resources available to them.
Methods
The study was designed as a non-randomized, individually delivered intervention to patients undergoing a shared medical appointment (SMA) for fall prevention. The population comprised a convenience sample referred by their primary care physician to the SMA.
We designed and launched a novel, ongoing quality improvement, evidence-based project, utilizing existing workflows within the electronic health record (EHR) system of our medical practice. Using an integrated medical system, we advertised the availability of the program within our academic internal medicine, primary care, and geriatric medicine clinics. Patients who were interested in a fall-prevention appointment, were referred with a standard “Internal Medicine” referral order in Epic. The referring provider was asked to forward the chart to one of the two key providers (RM and MR) championing the SMA. Patients were then contacted and scheduled to meet with a nurse to conduct appropriate screening before being scheduled into the shared-appointment visit.
Intervention: The intervention comprised an in person nurse visit followed by, on a separate day, a SMA led by a clinician. These are described below in detail:
Nurse visit: We provided standardized training to champion licensed vocational nurses (LVNs) to conduct in person pre-visit nurse assessments as suggested by the CDC. This nursing visit included completion of the STEADI Staying Independent Questionnaire (US Department of Health and Human Service, 2019), completion of a Snellen eye screening, conducting a Timed Up-and-Go (TUG) test (Barry et al., 2014; Schoene et al., 2013; Sprint et al., 2015; US Department of Health and Human Services, 2017b), and 30-Second Chair Stand, (30s-Chair Stand) (Ambrose et al., 2013) to assess physical function. The results were to be documented on a templated note within the EMR that was shared with champion LVNs. At this nurse visit, patients were provided details about the SMA format, scheduled in person or virtually based on preference, and provided informed consent to participate in a SMA.
Clinician SMA: The SMA was co-hosted by two clinicians with experience in exercise science in general, and fall risk reduction specifically, with up to six patients per session. The visit lasted approximately 2 hr. The first hour was spent reviewing fall-risk, fall history, medical history, and fall risk assessment from the nurse visit with focus on identifying potentially concerning findings and abnormal screens per CDC cuff offs (Centers for Disease Control & Prevention, 2022). Patient stories, concerns, and interests were emphasized, including previous successes and failures related to fall-risk reduction. Time was also spent answering patient questions. The second hour was spent in interactive didactic instruction highlighting available evidence about falls, fall risk, home safety, environmental safety, and reviewing specific low risk exercises that have been shown to be effective at improving posture, balance, and strength. Based on clinic risk screening and patient interest, a semi-tailored prescriptive recommendation and information booklet was provided by email within a week, with digital and community-based resources including group-based fall prevention exercises, differentiated by difficulty and physical location to facilitate participation. Most of these programs were selected in partnership with the local Public Health Department to be free or low cost and evidence-based.
Measures
In brief, data were obtained from patients who were referred to, and attended a SMA for fall prevention. We utilized clinic fill rates, nurse assessment timings prior to the clinic assessment, completion of entire nurse assessment, no-show rates, and questionnaires to patients who participated in the SMA to determine programmatic feasibility and success. Additionally, we captured basic demographic information regarding patient participation in the SMA, the STEADI Staying Independent score, Snellen results, orthostatic vital results, and appropriate cutoffs for objective measures of fall risk. For the TUG, we utilized the CDC suggested cutoff of 12 s to discriminate fall risk (US Department of Health & Human Services, 2017b). For the 30-s chair stand test, we utilized age and gender adjusted cut-offs (US Department of Health and Human Services, 2017a). Finally, in the context of studying the usability and acceptability of a novel platform for this preventive modality, all participants who attended were sent a questionnaire by email approximately 4 weeks after completing the SMA (Qualtrics, Provo, UT) with an appropriately worded System Usability Scale (Brooke, 1996); SUS, a non-proprietary validated questionnaire which is designed to understand the ease of use of new systems or programs using a five element Likert scale. This questionnaire includes the 10 questions typically included in a SUS, and we additionally included nine questions designed to assess the patient’s experience and their use of educational materials and resources discussed and made available.
Analysis: We evaluated baseline demographics of the first 52 patients seen within our shared medical appointments, including age, gender, fall relevant medical history and a as a history of osteoporosis or osteopenia via DXA scans, all obtained from review of the EHR, and measures of fall risk. We evaluated the associations between baseline demographic variables and clinically assessed measures of fall risk (Chi-square, Fischer’s Exact or ANOVA where appropriate). In addition, we included a descriptive analysis of common follow up recommendations, and for the subset of patients who responded to our survey, the patients’ perception of the program. All statistical analysis was performed on SPSS v.28 (IBM Armonk NY).
Results
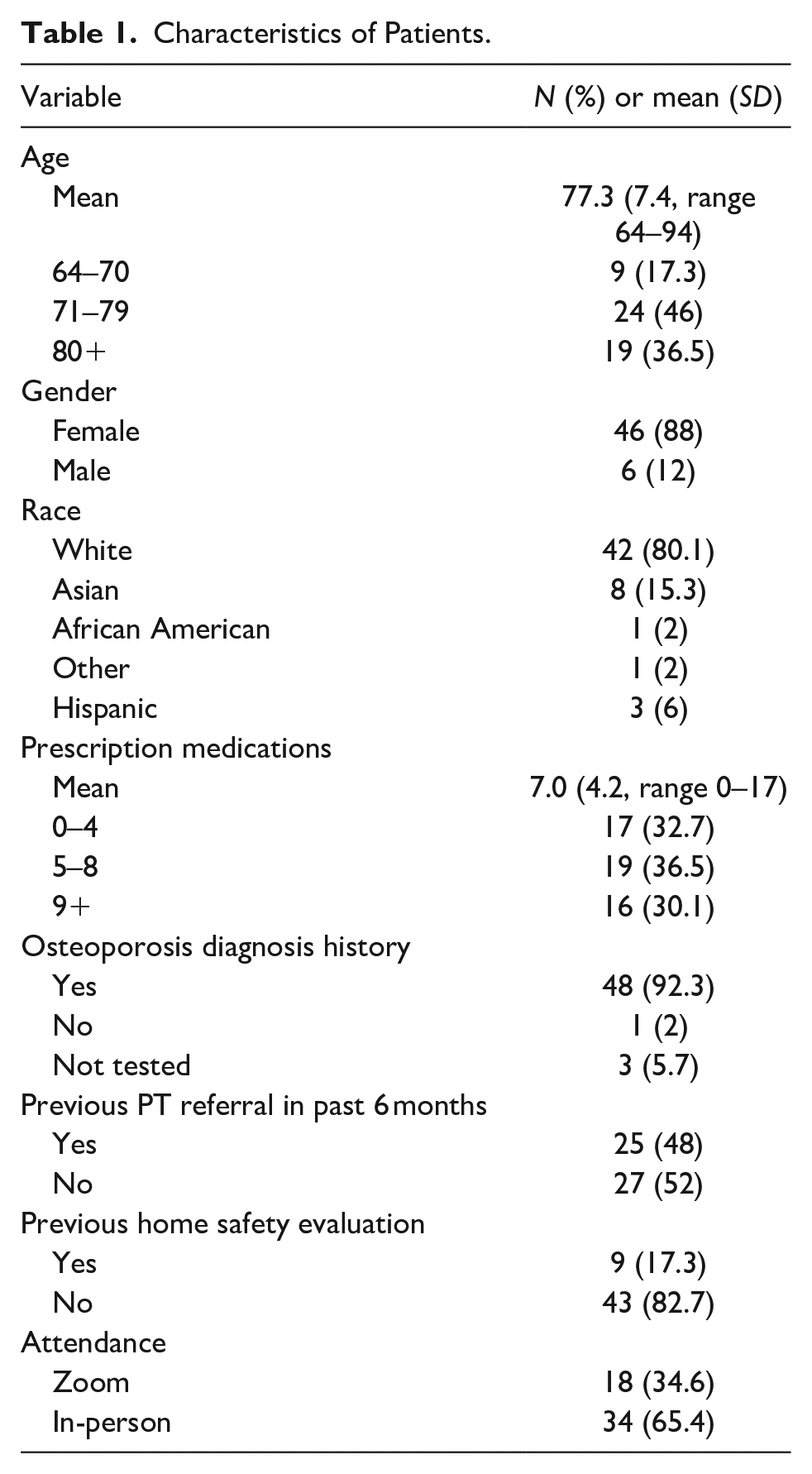
Between November 2021 and February 2023, we hosted 15 SMA Fall Prevention Clinic sessions, with 54 patients referred and scheduled. Of those scheduled, 52 (96%) completed the nurse pre-visit appointment and attended the SMA, for an average of 3.5 patients per SMA appointment (range 2–5). Of the 52 patients seen in the SMA, 18 (34%) attended virtually, 46 (88%) were female, and the average age was 77 years (±6.7, range 64–94). The average number of prescription medications was seven (±4.2), and 41 (77%) had osteoporosis. In terms of patients’ physical activity, the most reported activity was walking (33%) with a group-based physical activity following in frequency, such as yoga or tai chi. Other common physical activities included gardening and attending individual physical therapy sessions (Tables 1 and 2).
Characteristics of Patients.
Screening Characteristics.

Nurse Visit Assessment
The average Staying Independent Brochure Score was 4.9 (±3.4, range 0–12). Functional assessments showed an average TUG of 11.4 (±6.3) seconds, with 34 (65%) of patients having scores less than 12 s. The average 30-second chair rise was 12.7 (±5.2) stands, and 42 (81%) patients had normal age and gender adjusted 30-second chair rises. On Snellen visual acuity testing, seven (13%) were found to have corrected scores 20/60 or greater, and 12 patients (23%) were found to have abnormal orthostatic vital signs.
Age was not significantly associated with the number of prescription medications, the average SI brochure score, the modality of attendance (virtual or in-person), the TUG time, 30-s chair raises, or having abnormal TUG or 30-s chair rise times (results not shown). Associations between objective measures of fall risk and clinically collected data are reported in Table 3. No single question or marker was associated with each clinically collected measure or marker of fall risk; however the total SI Brochure score was statistically associated with having a TUG and 30 second chair rise scores predictive of fall risk (p < .001 for both). Additionally, select high yield questions such as subjective unsteadiness was associated with TUG and 30 s chair rise scores predictive of fall risk (p < .001) as well has having orthostatic vitals (p < .01). Polypharmacy and self-reported strength were statistically associated with predictive risk based on the TUG and 30 s chair rises (p < .05 for all measures).
Associations Between Screening Questions and Objective Fall Risk Measures.
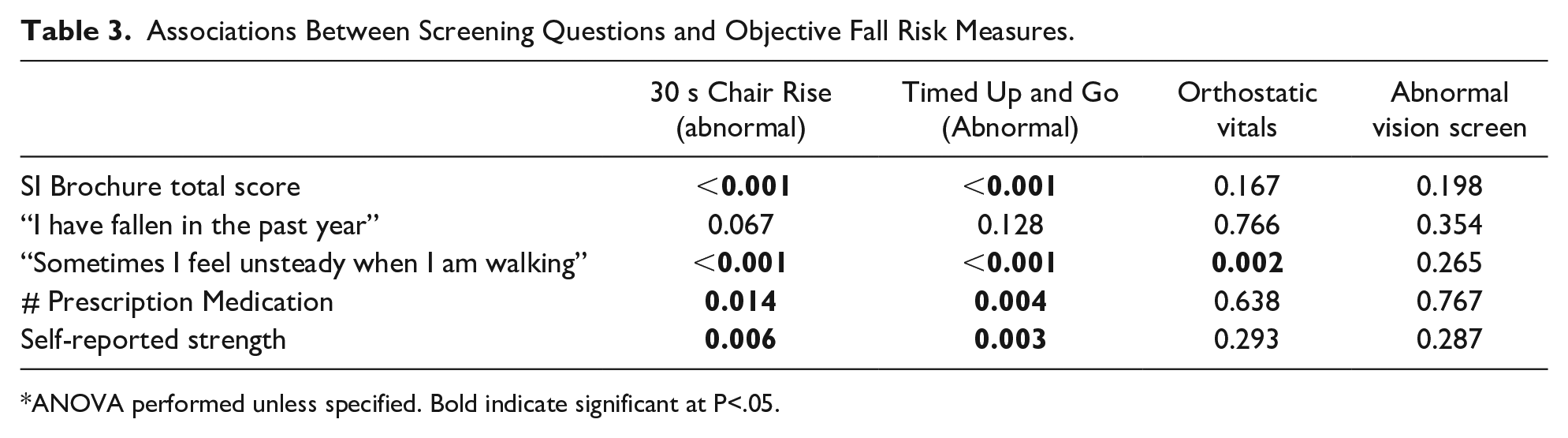
ANOVA performed unless specified. Bold indicate significant at P<.05.
Survey Experience
All participants were emailed 4 to 6 weeks after the SMA to provide an opportunity for feedback, and 12 of participants (23%) responded. The average System Usability Scale (SUS) score was 81.7, indicating excellent usability of this clinical model of screening and assessing for fall risk. Of the respondents, 5 of the 12 attended the clinic appointment in person, and seven by Zoom (average SUS scores 80.5 and 82.5, respectively). Nine additional questions included 7 Likert questions to understand user experience (1 = strongly disagree, 3 = neutral, 5 = strongly agree) and three scaled questions (0%–100%) to display behavioral change and assessment, although these questions were not filled out by all respondents as indicated in Table 4. Overall, users expressed appreciation of this clinic and feedback was supportive and suggested resources provided were overall useful (Table 4).
Survey Results from Patient Experience.

Discussion
In this evaluation of our Fall-Prevention SMA, we screened 52 older adults who were mostly non-Hispanic white women and found that this clinically integrated model was well accepted by patients. Here, the average Staying Independent Brochure score was 4.9, just above the CDC’s suggested cutoff of 4 to suggest elevated fall risk. Unsurprisingly therefore, the average TUG (11.4 s) and 30 s chair stand (12.7 165 stands/30 s) scores were close to thresholds indicative of risk of falling. We found that the Staying Independent Brochure Score was associated with objective markers of risk, as has been highlighted in other studies (Casey et al., 2017). Further, simply asking patients to self-report their strength on a 10-point scale also was significantly associated with having objective markers indicating elevated fall risk. This finding was interesting, yet unsurprising in that previous reports have also found those who fall more are likely to report fatigue (Blain et al., 2021) and having worsened validated measures of physical function (Hernandez et al., 2010). This is interesting and important, as perhaps it provides a useful clinical surrogate to help quickly stratify those most likely to benefit from more intensive screening and intervention.
Strengths of this program include the ability to integrate a clinically meaningful visit type with existing mechanisms already embedded within our healthcare system. We also utilized existing procedures, such as nurse visits, to collect relevant clinical data prior to the shared visit, allowing for some personalization in the visit in terms of addressing specific fall risk domains and providing appropriate corrective actions. Additionally, this clinic was fully available to all patients within the academic primary care network, versus selective recruitment. The accessibility increases the likelihood that this program could be adapted into other health systems. We also offered this visit both virtually and in-person, synchronously, to allow for more flexibility of patient needs. However, the providers anecdotally noted that when the visit was delivered entirely virtually or entirely in-person, the experience and the flow of the visit went more smoothly.
Limitations included a lack of complete electronic medical record integration, which would have allowed for a better understanding of process-level measures including the total number patients referred even if they did not schedule the nurse visit, and lack of systemic implementation, thereby clearly allowing a degree of selection bias. The vast majority of participants were female, and many were seen by specialists in an academic medical center, which may lessen generalizability. Our survey results (23% of respondents) were also likely adversely selected from those who were familiar with technology and found the appointment memorable enough to reply, which may bias the results—showcasing a trend for a higher response rate for those who attended by Zoom.
Additional work is warranted to further understand how clinical processes can integrate meaningful evidence-based, patient centered care. This is especially important as it relates to prevention in general, but more specifically with a focus on independence and function.
Conclusion
SMA are effective tools for clinically assessing fall risk in older adult patients and are well received by patients. This model of care delivery can augment usual primary and geriatric care by providing comprehensive fall assessment, screening, and medical recommendations to improve fall risk.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231186460 – Supplemental material for Shared-Medical Appointment for Screening and Risk Assessment for Fall Prevention
Supplemental material, sj-docx-1-ggm-10.1177_23337214231186460 for Shared-Medical Appointment for Screening and Risk Assessment for Fall Prevention by Ryan Moran, Michelle Ramirez, Gina Woods, Heather Hofflich, David Wing, MS and Jeanne Nichols in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Because this program was designed as a clinical assessment in a shared-medical appointment model, designed to include older adults, we initially designed the SMA to be performed entirely virtually after a one-on-one nurse visit. This was in part to mitigate the concerns of COVID-19, but also to improve user experience. However, after the first two months, because of patient interest and the opportunity to conduct the nurse assessment before the clinical assessment, we offered it in hybrid format within the conference room of the clinic, synchronously for those who opted to login digitally, or physically spaced for those who opted to attend in person. This project was reviewed by UCSD Risk Management and Billing and Compliance and approved as exempt for IRB review, by the UCSD Aligning and Coordinating Quality Improvement, Research, and Evaluation (ACQUIRE) Committee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.