
Abstract
Delirium is a common, often preventable fluctuating state of cognition associated with increased morbidity and mortality. This report describes the implementation of an interprofessional consultative Delirium Team formed to improve the prevention, detection, and management of delirium in a community hospital. Team members consulted refered inpatients with delirium to establish a care plan and provide recommendations for pharmacological and non-pharmacological management. The team also offered delirium-related education to unit staff, patients, and caregivers. Consultations were initially completed by the team Nurse Practitioner or Occupational Therapist, and complex patients were discussed with the team Geriatrician and Psychiatrist at rounds to optimize specialist input. Of the 160 patients managed by the team over the 8-month study period, two-thirds of referred patients did not require specialist consultation for their delirium management. Strategies most often recommended by experts for managing delirium were related to medical management, social/cognitive engagement, and functional mobility. Two-thirds of all recommendations made by the team were implemented. Barriers and facilitators to implementation and improving unit staff adherence are further described. The consultative Delirium Team is a promising model that should be further explored for managing an aging population in a capacity-limited medical system.
Introduction
Delirium is an acute change in mental status characterized by fluctuation in attention, cognition, and consciousness. It is associated with an increased risk of mortality, functional decline, postoperative complications, and longer hospital stay among other morbidities (Rubin et al., 2018). The etiology of delirium is proposed to be a multifactorial interaction between predisposing characteristics such as older age, sensory impairment, and cognitive impairment, and precipitating factors such as active infection, certain medications, and hospitalization (Inouye et al., 2014; Rubin et al., 2018). Clinical presentation is heterogeneous but may include increased or decreased arousal, confusion, hallucinations, and challenging behavoiurs.
Delirium is diagnosed in 18% to 50% of patients upon admission and occurs in 11% to 82% throughout hospitalization. An estimated 30% to 40% of cases are preventable, highlighting the importance of delirium prevention initiatives targeting at-risk patients (Inouye et al., 2014; Rubin et al., 2018). Multicomponent strategies have been recommended to target precipitating risk factors such as sedative medication use, sensory impairment, orientation, hydration, nutrition, sleep, and bowel and bladder disturbances (Inouye et al., 2014; Monaghan et al., 2021). These strategies can be implemented through an interprofessional consultation team model. In this model, specialized teams composed of nursing, occupational therapy, physical therapy, geriatrics, and psychiatry consult inpatients at risk for delirium (Deschodt et al., 2016; Monaghan et al., 2021; Trogrlić et al., 2015). Team medical specialists support patient care through regular team case reviews, thus optimizing costs and increasing the number of inpatients benefiting from specialist services.
Research on interprofessional consultative models for delirium has found them to be well-suited for hospitals with limited resources or professional capacity. They are generally well-liked by patients, clinicians, nurse managers, and decision-makers (Trogrlić et al., 2015). There is, however, a paucity in detailed descriptions of these models, significant heterogeneity within their design, and little guidance on how to implement them (Monaghan et al., 2021).
This brief report provides a detailed description of an innovative consultative Delirium Team model, key consultation activities, and uptake of the team’s recommendations on engaged units. We have followed the Template for Intervention Description and Replication (TIDieR) checklist and Revised Standards for Quality Improvement Reporting Excellence (SQUIRE) reporting guidelines (Hoffmann et al., 2014).
Methods
Innovation: An Interprofessional Consultative Delirium Team Model. This study was approved by the local research ethics board.
Setting: The Delirium Team was formed as part of an organization-wide quality improvement project to improve the prevention, detection, and management of delirium. This project was implemented on adult inpatient units across a large community hospital situated in one of the most ethnocultural and racially diverse cities in Canada. Processes were linked with existing strategic initiatives and hospital services to build sustainable changes within clinical practice and create efficiencies in workflow.
Delirium Team: The team was designed to leverage interprofessional collaboration, and included 1 FTE Occupational Therapist, 1 FTE Nurse Practitioner, a Geriatrician, and Geriatric Psychiatrist. They were each compensated by stipend. An Occupational Therapist was selected based on their scope of practice, including assessment of function and cognition. A Nurse Practitioner was chosen for their autonomous diagnostic and prescriptive authority and emphasis on teaching and leadership domains.
Referral system: As part of the larger project, nursing staff on engaged units were trained to screen adult inpatients for delirium every 12 hr with the Confusion Assessment Method (CAM), a well-validated instrument for identifying delirium (Helfand et al., 2021; Wei et al., 2008). The results of the CAM screening were entered into the Hospital Information System (HIS), and a HIS referral list of all patients who received two positive CAM results in 48 hr was automatically generated and sent to the Delirium Team. The team would then contact the most responsible provider of each patient on the list to inquire whether a consultation was indicated. Referrals from the weekend would be followed up on Monday morning. In addition, phycisians could also do a direct referral by emailing the Delirium Team.
Activities
Consultation: After reviewing the patient’s medical record, the Occupational Therapist or Nurse Practitioner would complete an initial consultation and patient assessment. The Delirium Team would then collaborate with the patient’s most responsible provider and nursing to draft a care plan. Care plans included pharmacological management, laboratory investigations, and non-pharmacological strategies targeting evidence-based key domains. These domains included social and cognitive function (e.g., encouraging family visits, participating in unit-based group activities), functional mobility (e.g., sitting up in a chair for meals, working with physio/occupational therapy), bowel/bladder habits (e.g., identifying and managing constipation, urinary retention), nutrition/hydration status (e.g., establishing appropriate diet, access to feeding aids), and pain (e.g., medication optimization, physio/occupational therapy). When needed the Nurse Practitioner and/or Occupational Therapist could discuss cases with the team MD over the phone, without the need for the specialist to see the patient at bedside. Recommendations were then shared with the patient’s most responsible provider, nursing, and allied health staff on the unit to be implemented. At the end of the consultation, the Delirium Team would leave a tent card on the patient’s side table introducing the team and describing any recommendations that were made. This provided an easily accessible summary of the visit to the patient, their family, and health care providers.
Patient management: Patients were followed by the Delirium Team for a short period to ensure that delirium was well-managed and they were responding to interventions. All interventions were aligned with the Registered Nurses’ Association of Ontario Best Practice Guideline on the care of Delirium, Dementia, and Depression in Older Adults to ensure that they adhered to quality standards.
Systematic case reviews: Patients with complex conditions were presented to the entire team, including the geriatrician or geriatric psychiatrist, during systematic case reviews that were scheduled twice per week. Adjustments to the care plan were made and implemented collaboratively by the team.
Education: The Delirium Team provided education on delirium to patients, their families, and unit staff to support local capacity building. To educate families, the tent cards left in patients’ rooms contained information on both standardized and customized non-pharmacological strategies that could be easily implemented by family members. To support staff education, the Delirium Team frequently visited engaged units to provide education at huddles, and provided in-depth training to a designated “Delirium Champion” on each unit.
Data Collection and Analysis
Participants: Data from all patients (N = 160) consulted by the delirium team between October 2018 and May 2019 were included in the main description and analysis. A subset of participants (n = 45) composed of all patients consulted in October 2018 and April 2019 were selected for an in-depth sub-analysis examining medication changes, laboratory orders, diagnostic imaging requests, and implementation of recommendations. These timelines were selected to explore potential trends over time, ensure the program was sufficiently in steady state after implementation, the Delirium Team was staffed with both an Nurse Practitioner and Occupational Therapist, and data were consistently available. The Delirium Team serviced medicine, surgery, rehabilitation, and cardiology units throughout this period.
Data collection: Data were extracted from Delirium Team tracking documents and from patients’ electronic medical records by a trained chart abstracter.
Data analysis: Descriptive statistics were performed, and values are presented as means (SD) and medians (IQR) for continuous values and counts (%) for categorical variables.
Results
An analysis of the entire study population (N = 160) was completed to describe the demographics and referral characteristics of patients consulted by the Delirium Team over 8 months. Most were older adults, with a mean age of 82.5 (SD 10.6), and there were slightly more men (88) than women (72) included.
As mentioned previously, referrals to the team could be made automatically through the HIS after two positive CAM results, or directly from a physician. Of referrals received, 47.5% were made through the HIS, 35% came from the patient’s primary physician, and 15% were directly from a specialist. Half of the patients were seen by both an Nurse Practitioner and Occupational Therapist, and the remaining were seen by one of the two. On average, patients had 1.55 (SD 1.3) follow-ups after initial consultation from the Delirium Team, and this did not differ between referral sources. Lastly, 38% of patients were brought to team rounds by the Nurse Practitioner or Occupational Therapist to obtain specialist input on management from the team geriatrician or psychiatrist. About 62% of patients were managed without specialist input.
Sub-Analysis Patient Characteristics
Table 1 describes the demographic and referral characteristics of 45 patients selected for further analysis. Demographics were similar to the comprehensive analysis. Recommendations were most often related to social/cognitive engagement (100.0%), medical management (86.7%), and functional mobility (88.9%).
Sub-Analysis Patient Characteristics, Consultation Recommendations and Implementation of Recommendations; n = 45.
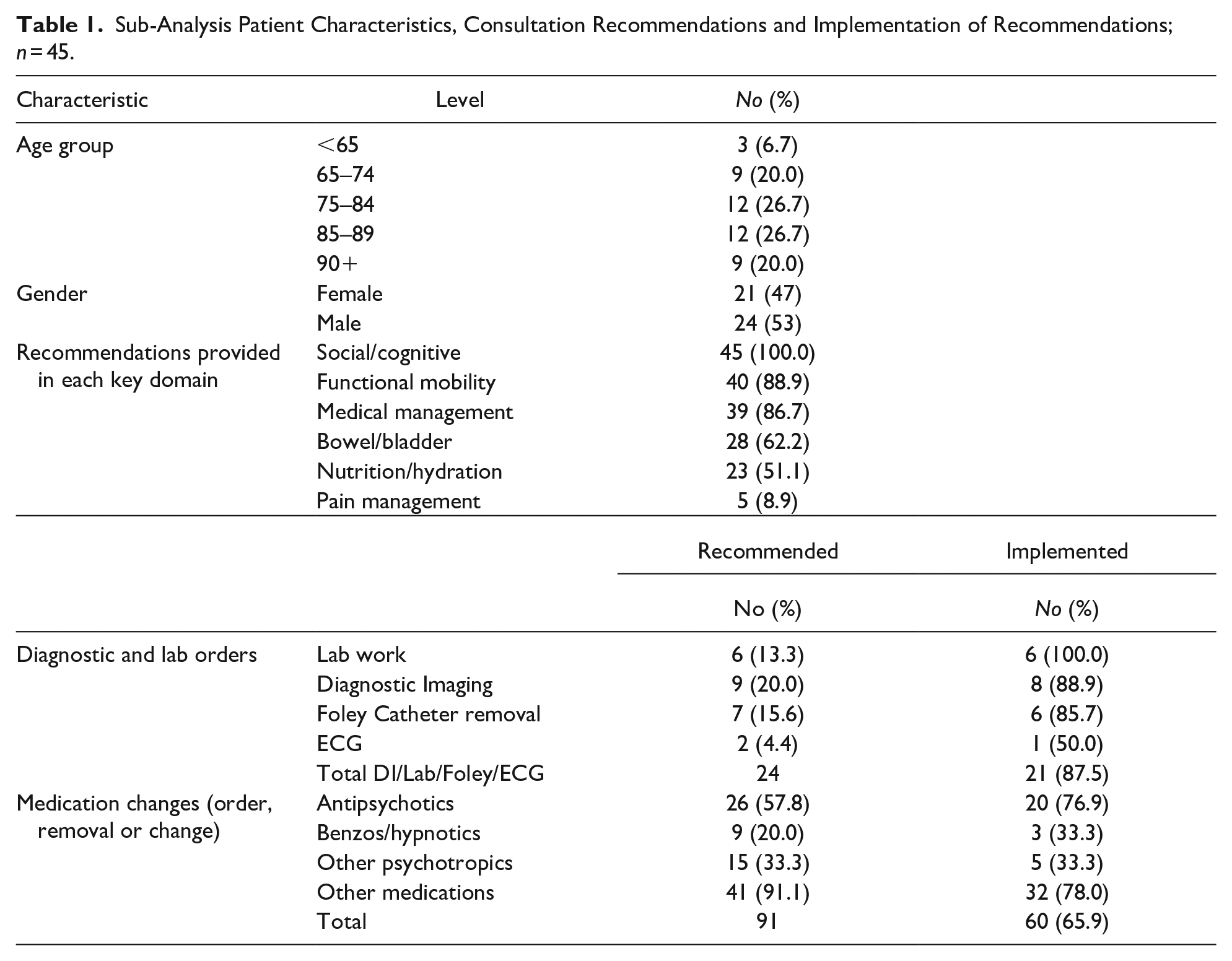
The most frequently ordered labs or diagnostic tests were bladder scans and diagnostic imaging. Overall, 65.9% of recommendations were implemented; diagnostics and labs were most frequently implented (90.3%) while ECGs were least frequently implemented (50%). Additionaly, there was notable variation in implementation by drug class.
Discussion
The Delirium Team supported care for older, medically complex patients by providing bedside patient consultation, recommendations for delirium management, and ongoing education to unit staff. Having an interprofessional team of delirium experts champion the intervention allowed for a more welcomed, sustained change in practice than hospital policy alone. Delirium is a highly preventable condition that often goes unrecognized. Prolonged episodes are associated with an increased length of stay, risk of admission to long-term care, morbidity, and mortality (Mccusker et al., 2003). Through this model, unit staff implemented strategies to prevent delirium where possible in at-risk patients and identify the condition early in its course.
Recommendations made by the Delirium Team for clinical management of delirium were most often related to social/cognitive engagement, functional mobility, and medical management. This highlights the value of the interprofessional structure, as the Nurse Practitioner was responsible for most medical management and the Occupational Therapist was responsible for functional mobility. Two-thirds of patients consulted by the Delirium Team were effectively managed without escalation to team-wide case review for physician input. These cases were managed, resolved, and discharged from the Delirium Team service exclusively by the Nurse Practitioner and Occupational Therapist, while more medically complex cases were brought to the geriatrician and psychiatrist. This model makes efficient use of specialists’ time.
A large proportion of referrals were made directly, which may indicate that hospital staff recognize the availability and utility of the consultative team. However, it could also indicate that the automatic alert generated after two positive CAM screens within 48 hr is not optimal given the fluctuating, acute onset of delirium. This may have been exacerbated during weekends when the Delirium Team was not available. In such instances, other services may have been contacted and specialist consultations may have occurred. An aim of the Delirium Team model was to mitigate the need for specialist consultation, however 15% of referrals came directly from specialists. The model may benefit from 7 day/week Delirium Team availability and a real-time referral system to allow for more timely and seamless consultations.
Recommendations made by the Delirium Team were usually implemented, however there is room for improvement. Adherence to recommendations is a frequently described barrier to intervention implementation and efficacy, and previous studies have found that 20% to 30% of treatment recommendations were not followed (Deschodt et al., 2012; Marcantonio et al., 2001). The impact of the Delirium Team could be enhanced by ensuring that a larger portion of recommendations, particularly medication changes, are implemented. This could be addressed through strategies such as ongoing education to frontline staff and physicians, building geriatric processes of care into routine care, and collaborating with specialties familiar with the unique needs of older adults (Monaghan et al., 2021).
For data collection, a Delirium Team-specific form was created in patients’ Electronic Medical Records and training was provided on how to complete them. Despite this, some information was tracked outside of the Electronic Medical Record, resulting in inconsistencies in data collection and incomplete datasets. This was likely exacerbated by clinical staff turnover. High turnover has previously been identified as a barrier to team-based delirium interventions, and future work should investigate how to build interprofessional team structures that encourage retention of team members and facilitate intervention longevity.
Conclusion
The interprofessional consultative delirium team was found to be an important component of a hospital-wide program to improve the prevention, detection, and management of delirium. In our hospital setting, two-thirds of consulted patients were successfully managed by the Nurse Practitioner and Occupational Therapist without physician specialist input, demonstrating the cost-effectiveness of the model. Older adults with complex health statuses benefit from the vigorous, interdisciplinary, and expert support. The Delirium Team model is a promising approach to patient care, particularly within a capacity-limited medical system managing an aging population.
Footnotes
Acknowledgements
The authors would like to acknowledge all present and past members of the MPA Adults and Seniors Inpatient working group, and the Delirium Team and MPA project management. In particular the contributions of Mareena Mathew, Toni Ivison, Monica Lau, Sara Banbury, Drs Don Head, Vesna Page, Margeret Grant, Nourhan Mohamed, Diana Nicolici, Meredith MacNaughton, Gillian Steeve, and Greg Brandsma.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Medical Psychiatry Alliance, a collaborative health partnership of the University of Toronto, the Centre for Addiction and Mental Health, the Hospital for Sick Children, Trillium Health Partners, the Ontario Ministry of Health and Long-Term Care, and an anonymous donor.