
Abstract
Ageism has been recognized as a global problem leading to poorer health, isolation, and workplace discrimination toward people based on their age. Consequently, there are several tools that measure levels and types of ageism with a focus on the quantification of degrees and types of ageism. While such quantification is valuable, this paper describes the development of an inventory, created over four stages, designed to foster introspective and collaborative thinking about age-directed values. In Stage 1, 34 items were identified through a comprehensive literature review. In Stage 2, the items were evaluated and revised via a focus group discussion. In Stage 3, the revised ASI was administered to a representative U.S. sample (N = 513). Based on factor and conceptual analysis, a revised version was tested on a second sample (N = 507) (Stage 4) and again revised. The final ASI consists of 35 age-related statements: 22 psychometrically linked to one of four domains, six related to identity, and seven that, although not aligned with statistical results, are conceptually important. Rather than provide an ageism score, the ASI is a tool for introspection and reflection about individual values and judgements about age which can lead to customized strategies to address potential age biases.
Introduction
According to the World Health Organization (2021), “Age is one of the first things we notice about other people” (p. xv). Ageism, or the devaluation of someone based on perceptions of age (Butler, 1969; Gendron et al., 2015), contributes to poorer health outcomes (Chang et al., 2020; Hu et al., 2021), self-imposed isolation (Shiovitz-Ezra & Shemesh, 2018), and workplace discrimination toward people as they age (Gendron et al., 2015; Lipnic, 2018; Malinen & Johnston, 2013). Because of the negative and pervasive consequences of ageism, there has been increased interest in tools to identity types and levels of ageism with the goal of creating appropriate educational interventions. Although several ageism measurement tools exist (See Ayalon et al., 2019 for a systematic review of ageism scales), many have been criticized for being limited in the dimensions of ageism they address (e.g., internalized beliefs, stereotypes, prejudices), lacking psychometric properties, and assumptions that the person completing the scale is “not old” (e.g., college students, medical students) (Allen et al., 2022; Ayalon et al., 2019). In addition, although many of these tools produce an overall ageism score to indicate a person’s level of ageism, they do little to foster engagement in reassessing thinking about values and actions related to age and aging. This is especially important to consider as ageism is not limited to older people but can affect people at any age, such as when a younger person is assumed to lack experience or insight based on the appearance of their age. As researchers have argued, a more multidimensional approach to understanding and addressing ageism that goes beyond stereotypes and knowledge about facts on aging is needed (Ayalon et al., 2019; Gendron et al., 2018; Iversen et al., 2009).
To counter these limitations and add to opportunities to improve assessing and addressing ageism, we developed the AgeSmart Inventory© (ASI), a multifaceted tool to facilitate interactive dialogues about age. We note a common distinction between inventories and scales. Inventories typically refer to questionnaires whereby participants appraise their own results, as opposed to scales, whereby appraisal of results is determined by outside criteria (e.g., how many symptoms are indicated; Adkins & Fiske, 2022). Rather than serve as a standalone scale, which cannot account for the many ways that ageism is manifested, expressed, and perpetuated, especially across age groups, the ASI is an inventory that encourages people completing it to probe outward and inward behaviors, attitudes, and identity values. As such, the ASI is a vehicle to facilitate discussions about values and actions based on age rather than providing an overall ageism score as in a scale, or to test one’s knowledge about aging or ageism. The purpose of this paper, therefore, is to provide context for the ASI development, details of the validation and refinement processes, and suggestions for its use. We begin with a brief overview of existing ageism scales and their shortcomings. We then present the four-stage process of the ASI’s development, validation and refinement which ultimately used a nationally representative sample of 507 people, ranging in age from 18 to 94 years. Finally, we discuss how the ASI could be used to lead users to deeper introspection regarding decisions they make about their own and others’ aging.
Background
Even before Robert Butler (1969) coined the term “ageism” in 1969 to describe “prejudice by one age group against another age group” (p. 243), there were instruments to assess misconceptions and attitudes about aging, each with shortcomings (Golde & Kogan, 1959; Tuckman & Lorge, 1952). One of the earliest, by Dinkel (1944), included 20 questions related to children’s attitudes toward caring for aging parents which was tested in a large sample of college and high school students. Later, Tuckman and Lorge (1952) developed an age-attitude questionnaire consisting of 137 yes/no questions spanning 13 categories: “physical, financial, conservatism, family, attitude toward the future, insecurity, mental deterioration, activities and interests, personality traits, best time of life, sex, cleanliness, and interference” (p. 337). Noting that items in Tuckman and Lorge’s work were not specific to older adults, Golde and Kogan (1959) created a 25-item sentence completion tool, tested in a group of 100 undergraduate students, to differentiate between attitudes toward people in general and toward older people specifically. Later, in an attempt to garner students’ interest in the topic of aging by showing them how many misconceptions they held (Palmore, 2005), Palmore’s (1977) “Facts on Aging” quiz included 25 true/false statements about aging.
Moving away from knowledge on aging, Fraboni et al.s’ (1990) “Scale of Ageism” used a four-point Likert scale to measure affective aspects of ageism (e.g., “I would prefer not to live with an old person”). More recent developments include Barker et al.’s (2007) Aging Perceptions Questionnaire (APQ), validated in a large sample (N = 2,033) of older adults (65–102 years of age). APQ questions center around eight subscales: identity, timeline (chronic), timeline (cyclical), consequences positive, consequences negative, control positive, control negative, and emotional representations. A sample question is “As I get older I continue to grow as a person.” Gendron et al.’s (2020) Relational Aging Anxiety, a refinement of the Aging Anxiety Scale (Lasher & Faulkender, 1993), addresses how personal identity, relational identity, and collective identity are understood and reinforced through interactions with self and others. Examples of statements include “I fear it will be very hard for me to find contentment in my older age” and “I will have plenty to occupy my time when I am older” (p. 292). However, one of the disadvantages of these and similar questions is the assumption that “older” is some undetermined time in the future, thereby overlooking ageism that one may experience in the present. In addition, many of the existing measures provide an ageism score that is not linked to clear action steps for addressing ageist views, attitudes, and behaviors. Consequently, to address the many shortcomings of existing ageism scales (validation testing primarily on younger people, assumptions that aging and being an older person are not immediately relevant to the respondents, focus on “facts” of aging), our goal was to create an inventory of statements—not a scale—of various dimensions and experiences of ageism (Adkins & Fiske, 2022). We describe the development and testing of the ASI in the following sections.
Data, Approach, and Corresponding Results by Stage
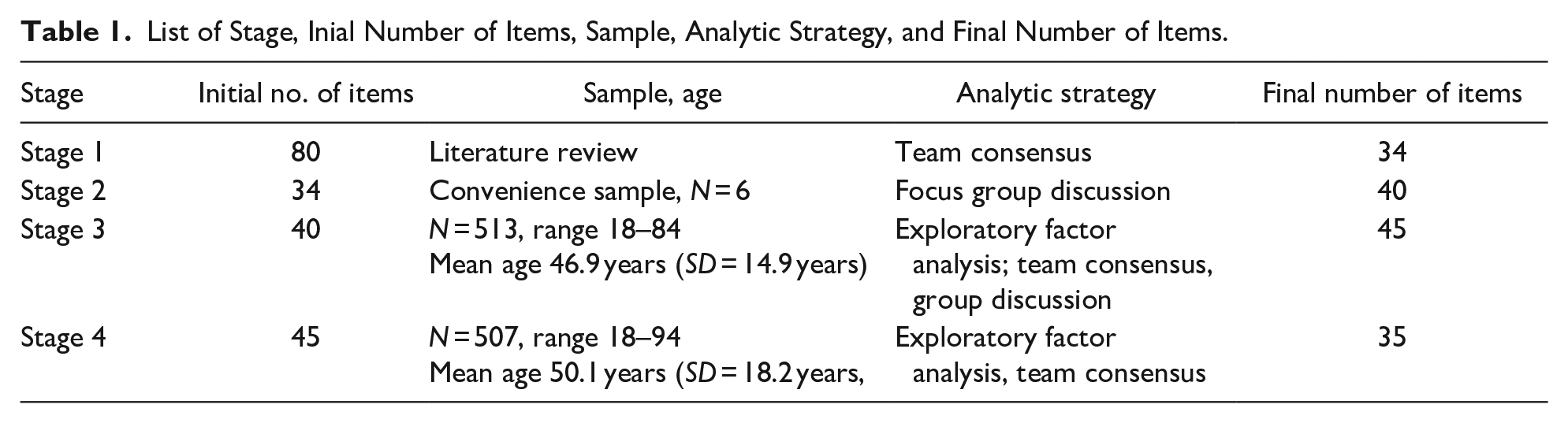
We developed the ASI over four stages described below. The multi-stage iterative process (see Table 1 and Figure 1) was approved by the aut!hors’ institutional review board. All participants provided electronic informed consent. Following is a description of the approach, relevant findings, and next steps for each stage.
List of Stage, Inial Number of Items, Sample, Analytic Strategy, and Final Number of Items.

Flowchart of the four ASI development stages.
Stage 1
Approach
To identify important domains and potential questions related to attitudes about age across various age ranges, we conducted a comprehensive literature review of journal articles, books and book chapters, and similar inventories or assessments within gerontology and in other disciplines (e.g., Ambivalent Ageism Scale (Cary et al., 2016), the Ambivalent Sexism Inventory (Glick & Fiske, 2018), Discrimination and the Implicit Association Test (Rudman & Ashmore, 2007). We searched broadly using terms such as “implicit bias,” “racism,” “sexism,” “ageism,” and gleaned reference lists for additional sources. We compiled a list of sample questions and question types (e.g., scenarios, Likert-scale agreement/disagreement) from various approaches to see how a particular bias was being addressed (e.g., “A good woman should be set on a pedestal” (Ambivalent Sexism Inventory; Glick & Fiske, 2018). We also searched for patterns in types of discriminatory practices being addressed.
Findings
The research team, composed of two senior gerontology faculty members and three doctoral students, identified three categories/typologies of biases, attitudes, or discriminatory practices: (1) internal (self-directed) and external (“other”-directed); (2) implicit (implied or indirectly expressed) and explicit (clearly or directly expressed), (3) positive (when seemingly kind assumptions are made about one group that are not made about another such as being articulate or being attractive), and negative (when negative attributes are applied to one group but not another). Another category, knowledge or factual information about a particular group, was also identified in several bias assessments. These four categories provided a framework for our next steps.
Next Steps
Using findings from the literature review, we created a list of 80 potential age-based statements based on existing measures of ageism and non-ageism scales and which corresponded to one of the four categories identified in our literature review. For example, original statements included “If you live long enough, you will get dementia” (factual information); “I am afraid my life will have no meaning when I am old” (internal); “Most older people have no interest in learning new things” (external), and “The older you get, the crankier you become” (explicit). Research team members then rated each statement (keep, revise, delete) based on wording, relevance to values, or judgements related to age. Each item and its rating were discussed by the research team. Using group consensus, items that received low ratings or were deemed repetitive were either removed or revised. The final inventory at Stage 1 consisted of 34 statements, scored on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree.”
Stage 2
Approach
In this stage, we administered our 34-item ASI to a convenience sample (N = 6) of people with gerontology training: two graduate students, one faculty member, and three researchers, all of whom agreed to participate in a 90-min focus group discussion (Nyumba et al., 2018). Unlike a focus group, which involves notetaking and structured analysis, a focus group discussion is meant to foster group discussion and consensus within the discussion period on a given topic. In selecting our sample, gerontology training was important since we were interested in learning from their expert perceptions about potential omissions, oversights, or other needed changes. Thirty minutes before the focus group discussion convened via Zoom, participants were sent a link to the ASI and asked to note their reactions to each question. We opened the focus group discussion by asking participants for their “gut” reaction to the statements to obtain information on wording, content, and face validity.
Findings
Several people noted inconsistencies in statement types: some were factual and not appropriate for the Likert-scale response, while others were based on perceptions and attitudes. Another person stated that some of the items provided “really great starting points for really interesting discussions,” especially statements that included phrases such as “in my opinion,” since they were internal judgements and perceptions rather than based on formal knowledge. At the end of the focus group discussion, the facilitator read back the two major consensus points from the discussion: First, include more “I” statements, and second, rephrase factual items to better align with the response agreement categories.
Next Steps
Based on the discussion, the inventory was again revised to include more items that were internal-perception/opinion-focused (e.g., “I think,” “In my experience”). We also removed factual items based on knowledge of aging in favor of statements that were more thought- provoking and better suited to start conversations, as per the focus group discussion participant’s observation. This resulted in a 40-item revised ASI.
Stage 3
Approach
We tested the 40-item revised ASI in a U.S. representative sample of 513 people aged 18 or older using Qualtrics™, an electronic survey tool and market research service. Qualtrics™ recruited participants from various sources, including website intercept recruitment, permission-based networks, and social media based on our criteria. Table 2 provides a percentage breakdown by age category, self-reported race/ethnicity, and self-reported gender. (See Supplemental Table 1 for numbers of participants for each demographic classification.)
Frequency, Percent, and Cumulative Percent by Stage for Age, Race/Ethnicity and Gender.

Findings
We conducted four exploratory factor analyses: one with eigenvalues set to ≥1.0 that constrained nothing and used the default rotation method, one that constrained the components to 8 and used rotation to maximize variation across them, one that limited factors to 5 and used varimax rotation, and the last one which forced only 4 factors using varimax. In all four models, the majority of variables loaded on the first factor, explaining most of the variation in the data before varimax rotation. The four-factor model identified items that conceptually were related. After studying and discussing individual items based on these groupings, we identified labels related to thematic content of the items within the four factors. Factor 1, age distancing, was comprised of items that supported separating people within workspaces and communities based on age. The second, claiming a non-ageist identity, included positive statements about aging, such as “Older people deserve our admiration.” The third, classic ageist stereotypes, included stereotypes such as “You can’t teach an old dog new tricks.” The fourth, fears/internalized life issues, related to questions such as fears about losing a job because of one’s age.
Next Steps
In reviewing our Stage 3 results, we discussed and conceptually re-evaluated some of our statements, regardless of whether they fit into the model. For example, the statement, “When I get old, I would rather live with my adult children than live alone” did load into factor 3, classic ageist stereotypes. Upon further review, we realized that the statement addressed living arrangement preferences, not behaviors or attitudes based on age. The statement was also confusing in that more than one concept was introduced: cohabitation with children (a person may not have children) and views about living alone. The statement was removed along with eight other items that may have loaded highly onto one of the factors but that were problematic in wording or did not fit the conceptualization. Other statements were either added (N = 9) or revised (N = 8) to address missing content. This interplay between empirical results and conceptualization of findings was a hallmark of this study. As Anastasi (1992) has pointed out, factor analysis is a means of organizing data into categories but not a means of identifying “fixed, universal behavior” (p. 614). After the third revision, the ASI had a total of 45 items. We also note that we presented Stage 3 findings at a workshop in conjunction with a national conference on aging. Prior to the presentation, we invited participants to complete the ASI and participate in an informal, unstructured discussion about their reactions. Much like our focus discussion group in Stage 2, participants commented that the “I” statements were particularly revealing to themselves. One person noted, for example, that although they responded “strongly disagree” to the statement, “I think that people should dress their age,” since they felt that people should wear whatever they wanted at any age, this person also said they “strongly agreed” with the statement, “I often ask myself whether my clothes are appropriate for my age.” In the discussion, the person said that the latter question really made them aware of their internal attitudes about age in a way that questions about other people’s age had not. This discussion helped to confirm our assumptions about the ASI, that it could be a useful tool in uncovering and examining one’s own beliefs while also making others aware of the persistence of age biases.
Stage 4
Approach
In this stage, our goal was to solidify what patterns had emerged from the factor analysis and iterative team consensus in Stage 3 using a new sample. We tested the 45-item revised ASI in a U.S. representative sample of 507 people, age 18 or older, using Qualtrics™ services as described in Stage 3. Table 2 provides a percentage breakdown by age category, self-reported race/ethnicity, and self-reported gender for Stage 3 and 4 (See Supplemental Table 2 for numbers of participants for each demographic classification.)
As in Stage 3, results from the analysis guided further discussion on factors and items (See Table 3.). In this iteration, we changed one of our factor labels—fears/internalized life issues to “language and ageism” based on items, all three items of which addressed words used to describe aging such as “old,” “senior,” and “elderly.”
Stage 4 Factor Loading, Variance, and Cronbach’s Alpha Values for 24 Items.

In the exploratory factor analysis for Stage 4, we first used Bartlett's Test of Sphericity and Kaiser-Meyer-Olkin (KMO) to ensure that the sample data were suitable for factor analysis. Next, all items were examined by the principal components factor method (Bryant & Yarnold, 1995) with varimax rotation, resulting in a more accurate and reproducible solution (Costello & Osborne, 2005). Non-cross-loading items with a loading value of .50 or higher were retained (Chen & Tsai, 2007). The factor analysis was conducted multiple times until the number of factors and eigenvalues were stable (i.e., no longer increasing or decreasing significantly) in the final model. A scree plot maps the improvement in the amount of variance that can be explained with the inclusion of each component (factor) in the model (Cattell, 1966). A scree plot (See Figure 2) was used to determine how many factors to retain for rotation. The sharp decline in eigen value improvement (the “elbow” of the curve) after the inclusion of a fourth component guided our decisions about the number of meaningful factors. For each latent factor extracted, Cronbach’s alpha of .70 was used to determine internal consistency and reliability (See Table 3). All analyses were performed using SPSS. Excluded items in the factor analysis were re-evaluated conceptually because this use of EFA is appropriate to explore a data set rather than testing an underlying theoretical framework (Costello & Osborne, 2005).

Scree plot of eigenvalues by number of principle components.
Findings
Results from Bartlett’s Test of Sphericity (Bartlett, 1950) (X2 = 3705.304, df = 276, p < .001) and the KMO (Kaiser, 1974) statistic (0.873) were well above the minimum standard for conducting a factor analysis suggested by Kline (1994). In addition, sampling adequacy measurements for each variable were within reasonable limits. Thus, factor analysis was appropriate for the data. Using the Kaiser criterion (eigenvalue >1) as well as visual inspection of the scree plot (Figure 1), the four factors identified corresponded with the 24 items included in Stage 4 and explained 50.64% of the variance.
In reviewing items that did load onto factors, we again used group consensus described in earlier stages to determine whether items were conceptually relevant despite being statistically appropriate. We agreed to remove two items from Factors 1 and 2, respectively, because of lack of conceptual relevance. For example, we deleted the statement “I think younger people should have their own dating site” since, in retrospect, we were unclear ourselves what view or attitude about age this was meant to address. When we examined items that failed to load onto any factor, we made an important discovery. After reviewing the 21 items that were not associated with a factor, we identified six as being the “I” statements related to internalized views about one’s own aging that we first mentioned in Stage 2. Conceptually, these items comprise what we have labeled the ASI Identity subscale; they all address an individual’s own aging-related identity and challenges. Following are the six ASI Identity scale items: “I worry about losing my job because I'm seen as old”; “I hide my age from others”; “I often ask myself whether my clothes are appropriate for my age”; “If people knew how old I really was, they would treat me differently”; “The older I get, the harder it is for me to learn new things”; and “I prefer friends who are my age.”
In addition, seven items failed to load strongly on a single factor but were viewed as conceptually relevant and important to generating internal and external dialogue about age judgements and actions via group consensus. Nine items were deleted due to lack of statistical and conceptual importance.
Next Steps
After again reviewing items both statistically and conceptually, our final ASI is composed of 35 items. Supplement Table 3 presents the factors and the items that comprise each one, as well as a measure of the internal consistency (Cronbach’s alpha) for each factor. All but one factor had good Cronbach’s alphas at or above .70. The fourth factor came close, and was considered to be conceptually meaningful, as the items all related to ageist language.
Discussion and Conclusion
Ageism is nuanced, multi-faceted, and consequential. Although there are numerous tools and assessments of ageism, we argue that we are currently less in need of an ageism score and more in need of a way to create positive change. One way that change can occur is through an inventory of items that is well suited to internal and collaborative discussions of age as a value that includes attitudinal, behavioral, and experiential dimensions. Unlike other tools and measures that provide an ageism score, the ASI is meant to provoke thinking about value judgements and actions related to age. As we have described, in the process of developing, testing, and refining the ASI, we were not interested in an overall score. Instead, we became interested in how items could elicit dialogue either internally or with others that might move the needle on unexamined forms and foundations of ageism, reflecting a shift away from quantifying ageism toward facilitating greater individual understanding of the many ways in which age is perceived and experienced, and how ageism can be unintentionally perpetuated.
During the four-stage process of developing the inventory, we uncovered several important ideas and dimensions of ageism that add to the robust agenda on this topic and pave the way for future research and action. A major contribution was the emergence of self-identity as an aging person as a cohesive concept. This element of ageism is complementary to yet different from internalized ageism and relational ageism. Internal ageism is typically described in terms of a person wanting to deny commonality with other people in their group (e.g., older adults) (Gendron et al., 2015) while relational ageism is described as self-identity as a schema based on our interactions with others (Gendron et al., 2020). What we address in the identity portion of the ASI is more concerned with how people may rethink everyday personal practices (e.g., wondering if they are dressing appropriately for their age) rather than comparing themselves with an “other.” In this way, we also address shortcomings in other aging tools that do not situate the respondent as an aging person, regardless of their chronological age. The ASI includes items that will allow further examination of this concept and how it relates to other dimensions of ageism. This juxtaposition of self-identity as an aging person with attitudes about others as aging adults needs further examination.
Another finding from our analysis underscores the importance of moving beyond statistical associations alone toward approaches that are statically informed yet theoretically and experientially driven (Anastasia, 1992). As we noted in several stages of our analyses, statements that did or did not fit into factorial loadings were not always conceptually meaningful. Nor did we eliminate statements because of their failure to fit within a model. By drawing on the reactions from focus group discussions and through an internal team review of each item, we carefully considered whether the statements appropriately addressed a domain related to age identity or if poor wording or conflated concepts made the statement confusing, something that the statistical data alone could not provide. This is important in studying complex topic such as ageism that has many causes, expressions, and effects that may differ depending on the age of the responder.
We do report limitations to the study. Both discussion groups were small and unstructured. A more structured “think aloud” approach to each of our statements, whereby participants are asked to read a statement and explain their thought process as they respond to the statement (Van Someren et al., 1994), would provide helpful information for each statement rather than general opinions about a few statements in particular. In addition, having formal and informal focus discussion groups composed of gerontology doctoral students, faculty, practitioners, and researchers, may have led to more ideologically driven responses and/or responses informed by the research literature. We also note that because we have nationally representative data from Stages 3 and 4, it would have been helpful to explore response patterns by age group. However, it was beyond the scope of this paper to do so.
Future research will address these issues and will continue to test and refine the conceptual and empirical strength of the inventory through confirmatory factor analysis (CFA). These analyses will address a limitation of the EFA used for this paper by providing inferential data to test the fit of the model to the data, and to test the invariance of the model across age, self-reported gender, and self-reported racial/ethnic groups.
Finally, the ASI is designed to generate action in the form of self-reflection, discussion, and collaborative exploration of what ageism looks like, where it comes from, and how it might be addressed. Given that ageism is such a complicated, multilayered phenomenon with many damaging effects for people as they age, our findings support the use of a tool that moves beyond an ageism score. Instead, the ASI challenges people to address their assumptions and judgements based on age. Consequently, the ASI is a tool that can be used in many educational and training sessions with people from various age groups to address ageism at is roots in values, beliefs and behaviors. The type of introspection that the ASI provides lends itself well to customized strategies to address age biases that go beyond improving knowledge about aging as a gauge to mark learning about ageism, which is often the case in existing ageism measure. We do not see the ASI being administered in a pre-/-post design to mark change, but instead as a baseline discovery for individuals or groups rather than a form of admonishment. For example, there can be rich discussion around items included in the domain claiming a non-ageist identity. Rather than potentially shaming someone who might think it is positive to compliment someone by telling them how “young” they look (2.2), the ASI provides an opening for considering the implications of doing so without judgement. Other items, such as in the identity scale portion, provide opportunities for people to think of ways that they perpetuate ageism within their own identities. Given that ageism is often missing from diversity, equity, and inclusion (DEI) efforts, tools such as the ASI can contribute to an important dimension of DEI. As such, development of appropriate educational tools is another important next step for the ASI.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231166215 – Supplemental material for The AgeSmart Inventory©: A Multifaceted Tool to Understand Age Bias
Supplemental material, sj-docx-1-ggm-10.1177_23337214231166215 for The AgeSmart Inventory©: A Multifaceted Tool to Understand Age Bias by Kate de Medeiros, Suzanne Kunkel and Lei Yu in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We would like to acknowledge and thank Alex D’Errico-Bronston and Amelia Pittman for their contributions to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received a seed grant from the Gerontological Society of America that provided partial support for the development of the initial AgeSmart Inventory©.
IRB Approval
IRB human subjects approval number: #03671e, Miami University Research Ethics and Integrity Program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.