
Abstract
This study described clients’ experiences within adult day care (ADC) and its related impacts. A multisite case study was conducted with 26 older adults from six ADCs in Tokyo, with interviews and field observations conducted between November 2020 and July 2022. The transcribed interviews and field notes were analyzed qualitatively. Three categories pertaining to context (“guilt and resignation to the current living conditions,” “desire for social connection despite frustrating limitations,” and “supported life based on weekly ADC routine”) and four categories about the experiences within ADC (“savoring disability- and age-friendly conversations,” “feeling happy about something new and positive,” “challenges for changes in self-image,” and “discomfort with others and the waste of time”) were extracted. Clients’ increased vulnerability due to disabilities and COVID-19 affected their experiences. ADCs provide a safe place for interaction, and their use must be encouraged to develop a disability- and age-friendly society.
Introduction
The spread of COVID-19 restricted people’s daily activities, particularly those with disabilities. These include access to long-term care (LTC) services. Adult day care (ADC) is a generic term for older-adult care; it comprises building-based services that offer various programs and amenities to older people (Orellana et al., 2020). In Japan, ADC is an LTC service that provides nursing and social care to older people with disabilities (Naruse & Kobayashi, 2022). ADC was the most popular LTC service among Japanese people with disabilities (Ministry of Health, Labour and Welfare, 2018). The benefits include improved physical, mental, and social functioning, exposure to comprehensive care, improved well-being, and alleviation of family caregivers’ burden (Ellen et al., 2017; Fields et al., 2014; Orellana et al., 2020). Gaugler et al. (2021) warned about the possibility of COVID-19 inhibiting the use of ADC by older people. Indeed, the COVID-19 pandemic correlated with reduced use of home care services in Japan, especially ADC, estimated at a 9.1% reduction (Matsumoto et al., 2021). Gaugler et al. (2021) suggested that this was because of the absence of clear evidence regarding the effects of such services from a randomized control design experiment. Extant literature has revealed that it is difficult to measure service use benefits among ADC clients because of the heterogeneity of their needs (Baumgarten et al., 2002). It is necessary to enhance and confirm the significance of ADC in society when numerous older adults hope to live in their homes and access their services (Gaugler et al., 2021).
While ADC embodies diverse functions because clients require a wide range of service provisions (Naruse & Kobayashi, 2022; Orellana et al., 2020), fulfilling social interaction needs for older people with disabilities was the most common for 75% of ADC clients (Naruse & Yamamoto-Mitani, 2021). However, the effectiveness of ADC attendance was unclear because ADC clients can interact with others outside of ADC. One study found no significant differences between loneliness among older adults who participated in ADC and older adults who did not participate (Iecovich & Biderman, 2012). Ayalon (2020) focused on the kind of social ties of ADC clients and found that a large, egocentric network with meaningful individuals (including people outside the center) was associated with a greater sense of community belonging.
The COVID-19 pandemic has changed the lives of ADC clients. Older adults with disabilities are less able to engage in direct social interaction with others and are more dependent on ADC interactions (Naruse et al., 2022). This situation indicates both an opportunity for ADCs to demonstrate their effectiveness and an increased need to improve the quality of social interactions within ADCs. Future interventions to improve the ADC experience would require conceptual networks that indicate possible causality. A conceptual framework is an illustrated concept that depicts interrelationships in a field (Miles & Huberman, 1994a). It encourages researchers and practitioners to identify the most important phenomenon or meaningful relationships. One single-site case study showed that the experience of ADC during the COVID-19 situation had various aspects of human relationships and effects on the daily context of ADC use; clients communicate by sharing their experiences, ranging from light chats to serious counseling about their problems, and the effects of these conversations lingered on until the next day (Naruse et al., 2022).
The primary objective of this study was to describe clients’ experiences within ADC to substantiate the conceptual network that illustrates the meaning of such experiences within ADC. This study was a continuation of the single-site case study mentioned above (Naruse et al., 2022). Because case studies including cases from multiple ADC center settings would represent typical experiences of older adults in ADCs, the multisite case study was conducted on diverse ADC clients and agencies in some of Tokyo’s typical urban areas. A nationwide analysis of ADC could not be conducted due to the uncertainty surrounding the COVID-19 variants and different restrictions in each area based on policy. Consequently, Tokyo, which had specific conditions and higher social restrictions in Japan, was chosen as the research site. The authors, ADC staff, and public health nursing professionals reviewed the restrictions for the older population with disabilities. They concluded that it had not changed much in the last 3 years in Tokyo.
Method
Design
This qualitative study was based on Yin’s (2009) case study method In the case study method, questions such as “why” and “how” are presented; these are useful for studying current phenomena and multiple cases. Yin defined the case study research method as an inquiry that deals with a technically distinctive situation. In such a situation, several variables from multiple sources of evidence converge in a triangulating fashion. The case study method benefits from the prior development of theoretical propositions that guide data collection and analysis.
Multiple case analyses within each case and across cases can substantiate contrasting or similar results from postulated hypotheses. Thus, the multisite case study was adopted to extend the results’ generalizability to a wider base of clients and agencies.
Participants
Six ADC agencies were recruited through snowball sampling (Goodman, 1961). The inclusion criteria for an agency were as follows: (1) ADC agency working in accordance with the Japanese long-term care insurance system and (2) ADC agency located within a densely inhabited district (designated urban areas based on statistical data; Geospatial Information Authority of Japan, 2015). ADC agencies that were asked to shut down by the public health sector due to significant clustering were excluded from the sample.
The interviewees comprised long-term clients of ADC. The following inclusion criteria were employed: (1) older adults who could participate in individual interviews in Japanese with the researcher, (2) older adults with the same difficulty with activities of daily living (level 1 or 2 according to the Japanese LTC insurance certification; Naruse & Masayuki, 2022), (3) older adults who did not face acute symptoms of disabilities, and (4) older adults willing to meet the researcher, irrespective of the COVID-19 pandemic. The first four interviews were conducted with female participants in a large agency. The data indicated the gender of the older adult and the ADC size that the participant used, which would contribute to their experience. The subsequent case study involved interviews with male participants in a small ADC. Sequential selection was developed based on consequent questions. Recruitment was discontinued because new codes were no longer being extracted.
The researcher contacted the agency administrator directly, presented a written explanation of the study’s purpose and content, and obtained their consent in written form. In response to the researcher’s request, the administrator selected candidates for interviews and arranged the date, time, and location for their introduction to the researcher. Upon introduction, the researcher gave the candidates a written explanation of the study’s purpose and content. An interview survey was conducted after obtaining their informed consent. The participating agency and participants were given 5,000-yen (approximately USD 40.0) and 1,000-yen (approximately USD 8.0) worth of library gift cards, respectively. This study was approved by the Ethics Committee of the Graduate School of Medicine and Faculty of Medicine at the University of Tokyo (Issue No. 2019037NI).
Data Collection
Before conducting the interview, a face sheet was used to enquire about the participants’ age, current use of ADC, and history of using ADC. Subsequently, a semi-structured individual interview was conducted using an interview guide. Each interview lasted approximately 60 minutes. Since the interviews were conducted slowly to ensure participants’ comfort, they were conducted twice (if possible), with an interval of at least 1 week.
The following questions were included in the interview guide: (1) how the interviewee spent their day at the day-care center; (2) what they thought of the others (users and staff) at the center; (3) what kind of relationships they had with the others.
The data were collected from October 2020 to August 2022. The interviews were recorded, and transcripts were verbatim for analysis. The interviewees’ tone of voice and facial expressions were also referenced as data. Two researchers were present during the interviews. The first author conducted the interview and the second one observed the first, ensured proper ventilation, set up panels for infection control, and monitored the participants’ physical condition. To ensure the quality of the interview data, we employed the following strategies. Interviews were conducted in a room where privacy is protected. After informing them that they would not be seen by anyone other than the researcher, the audio was recorded and transcribed verbatim. Interviews were conducted according to an interview guide. When possible, we interviewed twice in order to get them to reveal their true feelings about their interactions with others. Prior to the interviews, we arranged a casual chat time with the participants to make them feeling safe and comfortable. Soon after each interview, the voice data were reviewed for recording error check.
Besides the interviews, the first and second authors observed the day care rooms of each participating agency for an hour with the administrator’s permission. The purpose was to observe the participants and the people around them. However, they were careful not to record personal information other than those associated with the study participants. The observations were recorded as field notes and used for analysis. Observers stayed at ADCs and participated in ADC practices, taking a few unstructured notes. Observers noted participants’ behavior as they interacted with other people. Furthermore, ADC staff were interviewed about the participants’ usual behavior and how they distinguished between clients. All comments were included in the field notes.
Each older adult was considered one unit for data collection and analysis. We interviewed and observed the participants’ experiences within the ADC at the time of the interview and did not include longitudinal changes within the research period.
Data Analysis
The first author conducted the analysis, while the other authors reviewed the analytical process and results. Analysis was continued from the pre-data collection, single-site case study (Naruse et al., 2022), and the preliminary result from the first four cases was published.
First, each participant’s summary was compiled. It included information regarding past experiences within ADC and the participant’s context regarding ADC use. Then, multiple summaries were classified by examining their similarities and differences. Codes were created based on the client’s context for ADC use and experience of social interaction within ADC. These codes were integrated into each participant’s summary to reflect their unique context. Further, categories and subcategories were created for each case. An integrated version of the subcategories and categories was generated. The second and third authors confirmed the first author’s analytical process.
After the codes were developed, they were integrated into the conceptually clustered matrix for each case (Miles & Huberman, 1994b) to illustrate the relationship between ADC use and the experience of social interaction within ADC. A conceptually clustered matrix has rows and columns arranged to assimilate items that “belong together.” After producing a conceptually clustered matrix for all the cases, all the rows were combined into one table, and similar rows were merged. The merged rows were categorized to represent their causal relationship to ADC reactors. The illustration and abstraction encouraged researchers and practitioners to determine the most important phenomena and meaningful relationships in ADC intervention.
The researchers intended to conduct a peer review to get feedback from all the participants. However, it could not be achieved for all the participants due to the re-emergence of the COVID-19 pandemic in July 2022. Four agency administrators were contacted for peer review.
The Model of Social Interaction (SI model; Doble & Magill-Evans, 1992) was used throughout the analysis to develop the analytical framework. The model was developed to explain client’s social interaction and guide occupational therapist’s assessment and intervention process. Data collection and analysis were based on the model’s elements. Data that did not correspond with the elements of the SI model were excluded.
Results
Description of Participants and ADC Agencies
Twenty-six older people with disabilities from six agencies participated in this study. Table 1 presents the demographic information of participants and agencies. All ADC agencies were located in urban areas with easily accessible public transportation services, mobile phones, and Wi-Fi services.
Description of Participants and Adult Day Care Agencies.

Note. Re = rehabilitation; Ns = nursing; Mt = mealtime; Bt = bathing; Bp = bus pick up.
Reflects the average number of clients per day.
Reflects the number of independent rooms within the adult day care center.
Reflects the presence of care provision within the adult day care center by a check mark.
Reflects the years of ages.
Reflects the years of length of the adult day care center visit.
Reflects the number of visits per week.
Reflects the hours of length of stay at the adult day care center per day.
Contexts of and Experience Within the ADC
Analysis of the interviews and field notes identified and organized seven themes under two major categories. The first category reflected the perceived context of daily living with the routine use of ADC, while the second category reflected experiences within ADC use. Themes under the former were affected by the latter.
Contexts
Table 2 presents the three themes under the category of contexts.
Context of Adult Day Care Users.
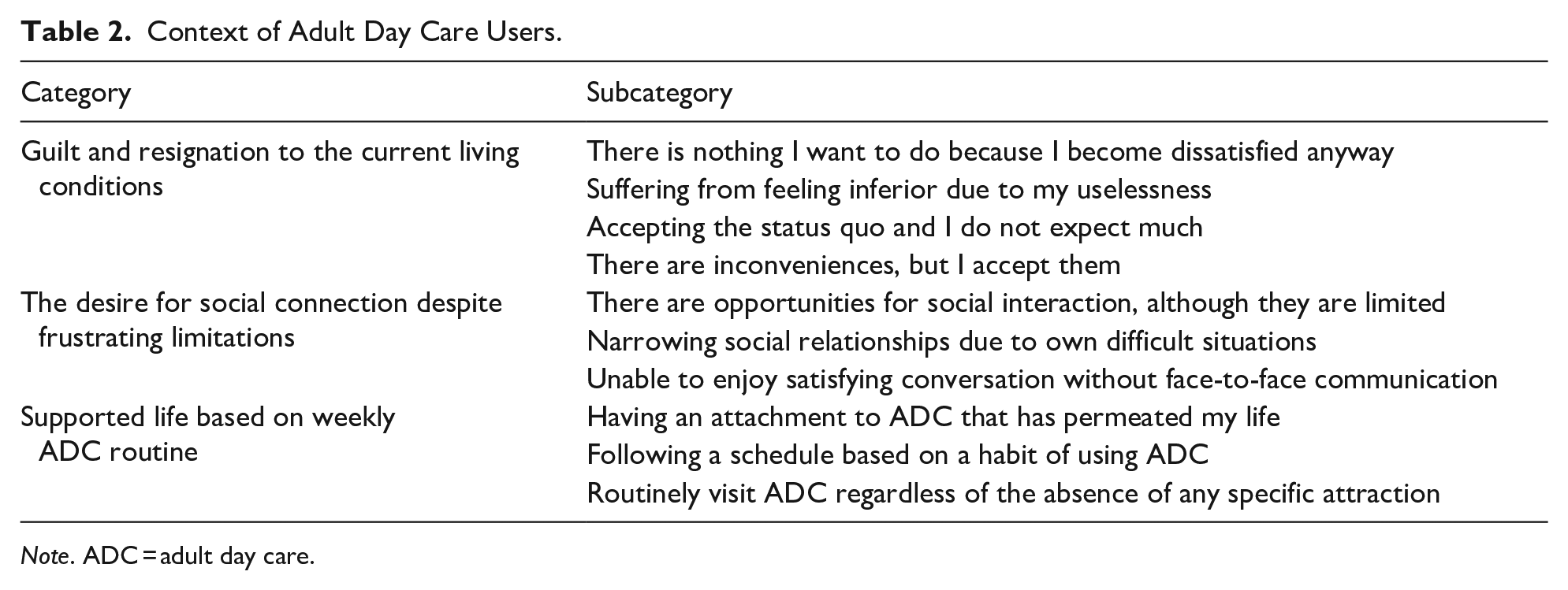
Note. ADC = adult day care.
Guilt and Resignation to the Current Living Conditions
Participants experienced feelings of guilt and resignation from their current living conditions, where they received good social welfare and LTC services. They experienced two ambivalent feelings; satisfaction and dissatisfaction.
The Desire for Social Connection Despite Frustrating Limitations
Participants expressed their desire to connect with other people through face-to-face communication. Some participants had some opportunities remaining for social interaction but they were limited. Their world had been narrowing, but they could not be satisfied with their social interaction using information communication technologies (ICTs).
Supported Life Based on Weekly ADC Routine
Participants explained ADC as an essential resource of their life and fundamental weekly routine. Some participants felt attached to ADC, experiencing pleasure in coming for the routine, but some considered it as a job task and recognized ADC as their work site.
Experience Within ADC
The four themes under the category of experience within ADC are presented in Table 3.
Experience Within Adult Day Care.

Savoring Disability- and Age-friendly Conversations
Participants experienced joyful interactions with other clients and staff in ADCs. Moreover, they behaved politely to avoid trouble. ADC environment was accessible and feasible for older people with disabilities to stay and communicate with others. Some participants explained that ADC has a disability- and age-friendly environment.
Feeling Happy About Something New and Positive
Participants experienced some new things in ADCs and sometimes incorporated them into their daily lives. ADC environment with supportive professional staff and other older adults promoted new encounters that included new hobbies, new friends, and new interests. Encountering something new created new hope and enjoyment for participants, removing their attitude of hopelessness and “guilt and resignation to unfavorable living conditions.”
Challenges for Changes in Self-image
Participants had encountered confusion caused by their changed self-image. An administrated environment with excessive support, childish activities, and being surrounded by functionally inferior people hurt participants’ pride; however, they understood that it was reasonable for their remaining function and safety. One participant (ID03) said that when staff members provide excessive support for tasks that she can complete by herself, it hurts her pride, as if they think she is incapable of doing them. She wanted to be as independent as possible. Another participant (ID04) experienced anxiety. She explained that ADC resembled a childish school setting and that it was difficult to accept the fact that other people seemed to enjoy it.
Then they needed to change their independent self-image into a dependent one, which brought negative feelings for themselves. Participants tried to act like better people to avoid being their inferior selves in the group. This included the presentation of humility through self-pity, taking a dominant position. These challenges for changes in self-image moderated or improved the participants’ anxiety or fear from “guilt and resignation to current living conditions.” One widower (ID21), who did not express loneliness or interest in conversing with others, frequently noted that he felt sorry about being useless and wasting the ADC nursing staff’s time. The researchers observed that, instead of chatting with other participants, he engaged in serious conversations about his disease with staff members as ones would with longtime friends. Another participant (ID01) frequently expressed her feelings of uselessness in the interviews as well as in the ADC friend group. Other people listened silently and then gave her encouragement. According to the researchers, she seemed like a tragic heroine on a stage who achieved satisfaction at the end of her performance.
Discomfort With Others and the Waste of Time
Some participants experienced feeling dissatisfied with being together with others in the ADC environment. Some participants mentioned that they left their previous ADC agencies because of dissatisfaction with those agencies. This delayed attachment to the ADCs and the feeling of a “supported life based on weekly ADC routine.”
Discussion
The three pressures of aging, disability, and COVID-19 rapidly narrowed the scope of the world where ADC clients spent their daily lives. Making and maintaining a network is a notable contribution of ADC (Aday et al., 2006; Orellana et al., 2020). Clients found it easier to talk to other clients in ADC because they shared similar memories. Such interactions occurred like “peer-assisted learning”—without professionals to help clarify life’s problems and identify solutions through conversations (Topping & Ehly, 1998). Contrarily, male clients preferred interacting with staff members to ensure secrecy. This could have been caused by ingrained masculinity; the traditional Japanese gender-role division of labor prohibits men from showing weakness or expressing their feelings (Ito, 1996). Such a support network increases the likelihood of activity participation (Aday et al., 2006), contributing to the perception of well-being (Dabelko-Schoeny & King, 2010). In times of limited outdoor social interaction, for example, COVID-19 lockdowns, adequate social interaction in the ADC may predict better client well-being. Surrounded and supported by people, the environment also encouraged them to find new hobbies to enjoy. Hobbies are associated with improved health (Arslantaş et al., 2015; Johnson et al., 2017; Kobayashi et al., 2021). As participants were resigned to having hobbies, the ADC environment may have the ability to help them find hobbies that fit their disabilities or find new interests. Encountering new networks and hobbies enables older adults to look at the world more positively.
Staying at ADC centers also causes social comparison with other old people and then it contributed to updating self-image. It was sometimes distressing for participants to be treated the same way as older people with disabilities equal to or more severe than their own. Social comparisons have also been observed among residents of nursing homes in the UK (Paddock et al., 2018). When their self-image was shaken, the elderly took various measures, but they all attempted to safely renew their self-image by using the group nature of ADC. It included self-pity, that is an emotional response we sometimes experience (Kahn, 1965). Instead of accepting that they were older adults with disabilities, they were trying to gain a more favorable position within that group.
The enjoyment of social interaction, the acquisition of hobbies, and the safe renewal of self-image motivate people to use ADC. This would motivate the next visit, a cycle that contributes to a life with ADC as a routine with good long-term outcomes. Methods to encourage successful experiences that motivate users need to be developed. We can expect to improve the resolution of the causal model of ADCs and contribute to visualizing the value of ADC services by clarifying the contribution of such successful experiences to users’ health status.
Simultaneously, an unpleasant experience within the ADC may reduce the willingness to use the ADC. It is considered necessary to ensure successful experiences and reduce unpleasant experiences. This study describes uncomfortable experiences as not feeling a sense of meaningfulness and having troubles with others. A future study focusing on people leaving the center and describing unpleasant experiences would help in creating a plan.
Implications for Practice and Research
There are two implications for developing better interventions within ADCs. First is the early adaptation of information and communication technology (ICT). Online virtual chatting could be an unfamiliar and difficult form of communication for older adults because of its delayed eye contact (Jokinen et al., 2010) and difficulty knowing who should speak next and when (Boland et al., 2022). Practice using ICT tools in ADC settings is expected to provide older adults with greater skills and confidence (McMurchie et al., 2013) and enable them to communicate using ICT in the face of decreasing social interactions.
The second implication regards the ADC users updating their preferred self-image. Differences in individuals’ self-evaluation of their self-image reflect differences in the mindsets of different cultures. In the West, the motivation to enhance and maintain one’s self-esteem is predominant, whereas in East Asian countries including Japan, the motivation to recognize one’s own inferior attributes and improve them through effort prevails (Heine et al., 2001). The Japanese older adult participants used the ADC group atmosphere to accept their new self-image while experiencing confusion because of the gap between their desired self-image and the real service delivery environment. If we can understand how older adults achieve and adjust to a positive self-image, we may be able to visualize the potential contributions of ADC. Future research and comparisons from an international perspective could contribute to the recognition of older adults’ experiences within a Japanese cultural context, which will help improve the care of ADC users originating outside of Japan.
Limitations
There are several limitations of the study. In order to maintain a social distance during the COVID-19 pandemic, researchers could not sit near the participants. Instead, to monitor and manage the environment, two researchers stayed in an interview room. These conditions could make it difficult for the participating older adults to feel comfortable and safe in the interviews, and our results might not fully reflect their experiences. Additionally, the study only included 26 older adults with chronic partial difficulties with daily living from six ADCs located in urban areas in Japan. Because it was difficult to visit ADCs and conduct direct interviews and observations due to COVID-19, the participant ADCs were limited to those agencies that had existing positive relationships with the researchers. It is also possible that there were clients who feel positively about ADC and therefore would only speak highly of their experiences there. We believe that our results can contribute to the understanding of experiences among similar populations in urban areas; however, the findings cannot describe the experiences of ADC clients with more severe and/or acute disabilities, those living in rural areas or other countries, or those with negative feelings toward their ADC agencies. Further, family caregivers were not interviewed; thus, the analysis lacks the family perspective. Consequently, future research should examine causality by using case study that includes multiple sources of caregiving.
Conclusion
Although ADC clients were prone to pessimism with aging, disability, and the pandemic situation, ADCs provided resources to broaden their perspectives and to challenge updating their self-image. However, the ADC’s group nature was also utilized to prevent the negative feelings associated with renewal. Successful experiences encouraged the continued use of ADC and helped establish a daily schedule of spending time with support. Future work is needed to develop interventions that will achieve more successful experiences.
Footnotes
Author Contributions
Conceptualization, N.T.; methodology, N.T.; software, N.T.; validation, N.T., M.K., and K.J.; formal analysis, N.T. and H.M.; investigation, N.T.; resources, N.T.; data curation, N.T. and H.M.; writing—original draft preparation, N.T. and R.T.-I.; writing—review and editing, N.T.; visualization, N.T.; supervision, N.T.; project administration, N.T.; and funding acquisition, N.T. All authors have read and agreed to the version of the manuscript submitted for publication.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare no conflicts of interest. Mr Masakazu Hatsushi, the second author, is a staff member of the General Incorporated Association. He did not receive any payment from ADCs that related to conflicts of interest. Mr Masayuki Kobayashi and Junichi Kato, the fourth and fifth authors, are administrators of Long term care service agency that provided ADC service in Japan. They were employed by the agencies, but they did not receive any payment from ADCs that related to conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Japan Society for the Promotion of Science Grant-in-Aid for Scientific Research (B; Grant number: 20H04009).
Research Ethics and Research Participant Consent
Consent was confirmed in writing. The ADCs that participated in the interview survey were given 5,000-yen (about 35.5 USD), and the participants were given 1,000-yen (about 7.1 USD) worth of library cards. This study was approved by the Ethics Committee of the Graduate School of Medicine and Faculty of Medicine at the University of Tokyo (Issue No. 2019037NI)
Data Availability
Data from this study are available through reasonable request to the corresponding author.