
Abstract
Introduction
Nonagenarians comprise a significantly larger population than they did in the past (Zafrir et al., 2010). Aging itself is associated with deterioration in health status. Many geriatric conditions are independently associated with both short- and long-term mortality in older patients and acute hospitalization of the oldest adults even more so, especially in patients with severe comorbidities (Bien et al.’s, 2015; Matzen et al., 2012). Acute hospitalization can be a double-edged sword for this population, as it might be followed by progressive physical and functional decline and increased in-hospital and post-discharge mortality (Iwata et al., 2006; Ponzetto et al., 2003; Zafrir et al., 2010).
There are relatively few studies regarding risk factors for post-discharge mortality of older patients. From these few, it appears that the following factors are important predictors of mortality: older age, cognitive decline, impaired functional status, and number and type of diagnoses (Iwata et al., 2006; Ponzetto et al., 2003).
In oldest-old patients, acute medical conditions requiring emergent hospitalization is frequently followed by high rate of progressive physical decline and increased mortality after discharge. Patients ≥90 years old show poor survival prognosis in the short- and long-term survival after hospital discharge (Barba et al., 2011).
Prognostic information collected during hospitalization can help in identifying groups at high risk for poor outcomes, in whom targeted treatment interventions may be indicated (Iwata et al., 2006).
It is important to consider clinical and functional domains when assessing a prognosis in older patients as well as being aware of the complexity of predicting mortality in the older patients (Ponzetto et al., 2003).
Despite latest increase in medical research, the literature on determinants of survival of geriatric patients is very limited (Bień et al., 2015). To our knowledge, this is the first study to identify predictive factors for post-discharge mortality in the nonagenarian patients during a very long follow-up. If some risk factors, including clinical and functional parameters, are reduced during hospitalization following a proper treatment, it might extend time to death in the older patients. The aim of this study was to identify risk factors for post-discharge mortality in nonagenarian patients.
Methods
This is a retrospective study of patients discharged from acute geriatric ward. We retrospectively surveyed electronic hospital health records of 977 older patients, aged ≥90 years, admitted between January 2007 and December 2010 from the emergency room to the acute geriatrics ward at a large community-based general hospital. Eight hundred sixty-four patients survived and were discharged from the hospital. Out of them, we have followed 448 patients for the risk factors for mortality within 1 month, within 1 year after discharge and throughout 14 years.
The recorded data included (Tal, 2022) patient demographics (e.g., age, sex, hospitalization date, stay duration, readmissions number, and death), medical diagnoses, laboratory results, and medications. We retrieved the following medical data: admission diagnoses as well as comorbidities, including dementia, pneumonia, ischemic heart disease (IHD), congestive heart failure (CHF), cerebrovascular accident (CVA), chronic renal failure (CRF), chronic obstructive pulmonary disease (COPD), anemia, malignancy, and falls. The drug types we retrieved were: statins, calcium blockers, β-blockers, angiotensin-converting enzyme (ACE) inhibitors, anti-depressants, benzodiazepines, neuroleptics, aspirin, and diuretics. Data on functional and cognitive status were also recorded. For each patient, Charlson Co-morbidity Index (CCI) score and age-adjusted CCI (ACCI) score were calculated (Charlson et al., 1987; J. X. Lin et al., 2019). The ACCI is a simple scoring system further combining the two related factors of age and comorbidity. For age adjustment, 1 point is added for patients over 40 years for each additional 10 years of age (J. X. Lin et al., 2019). We compared the characteristics of the patients who survived with those who died within 1 month and 1 year after discharge from the hospital. The study was approved by the Institutional Ethics Committee of the Kaplan Medical Center, Rehovot, Israel.
Statistical analysis
The data were analyzed, using JMP Pro 16.0.0 (2021 SAS Institute Inc.). Data records were complete for all 448 patients with the exception of functional status, which was available for 299 patients only. In order to use all 448 patients for the multivariate analyses, functional status was imputed for the missing cases, based on nominal logistic regression, using all other available data as predictors. This method predicted functional status correctly for 92% of the patients with complete records.
Univariate comparisons of survivors to non-survivors were performed by t-test for continuous variables and by chi-squared test for categorical variables. Variables, whose univariate significance was .10 or less, were considered as candidates for stepwise multiple logistic regression for 1 month and for 1 year mortality, using alpha = .10 for retention and alpha = .10 for removal.
Analysis of survival time within a 14-year period was performed by Cox proportional hazards regression, first for each potential factor (variable) separately. Variables, whose hazard ratio was significantly different from 1 at the 10% level, were considered for use in multiple Cox regression. From this full model, variables were removed one by one, according to their significance in the model until no improvement was seen in the Akaike Information Criterion (AIC). The final model included, as predictors, ACCI, fully dependent functional status, CHF, anemia and dementia as comorbidities, treatment with neuroleptics, low serum albumin, and elevated levels of urea, troponin I, and vitamin B12. Hazard ratios were calculated for each of these predictors after adjusting for all the other predictors in the model. Kaplan Meier survival curves were calculated for some factors of special interest after correcting for the remaining predictors in the Cox regression.
Results
Selected characteristics of 448 patients (58% females), stratified according to death within 1 month and within 1 year after discharge from hospital, are presented in Table 1. Their mean age was 93.1 ± 3.3 (90–114) years. Within 1 month and within 1 year after discharge, 11.16% and 37% of the patients, respectively, died. The most common admission diagnoses were: urinary tract infection (UTI), 19%; COPD exacerbation, 13%; and pneumonia, 9%. About 59% of the patients had low serum albumin. Sixty five percent of the patients consumed ≥5 drugs.
Univariate Analysis of Selected Patient Characteristics by Mortality Within 1 Month and Within 1 Year After Discharge (N = 448).

Note. CCI = Charlson Comorbidity Index; ACCI = age-adjusted Charlson Comorbidity Index; low vitamin B12 = <200 pmol/L; high vitamin B12 = >666 pmol/L; low albumin = <3.5; low cholesterol = <150 g/dL; high troponin I = >15.6 pg/mL.
Within 1 year after discharge, but not after 1 month, the number of comorbidities was significantly higher among the dead than among the survivals (6.44 vs. 5.78). Also, CCI and ACCI scores were significantly higher among the patients, who died within 1 year (3.81 vs. 2.98 and 8.81 vs. 7.94, respectively), but not within 1 month after discharge. A significantly higher percentage of patients presenting with anemia, dementia, and malignancy as comorbidity, died within 1 year after discharge (39.2% vs. 28.7 %; 58.4% vs. 33.3%; 31.9% vs. 22.0%, respectively). Mortality within 1 year was also significantly higher in patients treated with neuroleptic drugs (9.6% vs. 2.8%). A significantly higher proportion of patients with elevated sodium, died within 1 year (4.2% vs. 1.1%). Mortality within 1 month and 1 year was higher among patients with on-admission low albumin level, high levels of urea and high levels of troponin I (within 1 month: 78% vs. 56.3% and respectively; 84.0% vs. 65.3% respectively; 14.0% vs. 4.0%, respectively; and within 1 year: 69.9% vs. 52.1%, respectively; 78.9% vs. 60.6%, respectively; 7.8% vs. 3.5%, respectively). Mortality within 1 month and 1 year was higher for the combined data of dependent and frail functions (96.3% vs. 80.1% and 94.1% vs. 76.6%, respectively).
By multiple logistic regression analysis (Table 2), low albumin, high urea, and full dependence (in descending order of importance), were risk factors for mortality within 1 month and within 1 year after discharge from hospital. A lower number of hospitalizations during the last year, and high troponin I were specific risk factors for mortality within 1 month. ACCI score, neuroleptic drug treatments and frailty were specific risk factors for mortality within 1 year. The significant risk factors for post-discharge mortality, in the study, explain 15% of the variation in mortality within 1 month after discharge, and 12% of the variation in morality within 1 year after discharge.
Risk Factors for Mortality Within 1 Month and 1 Year After Discharge, by Multiple Logistic Regression Analysis.
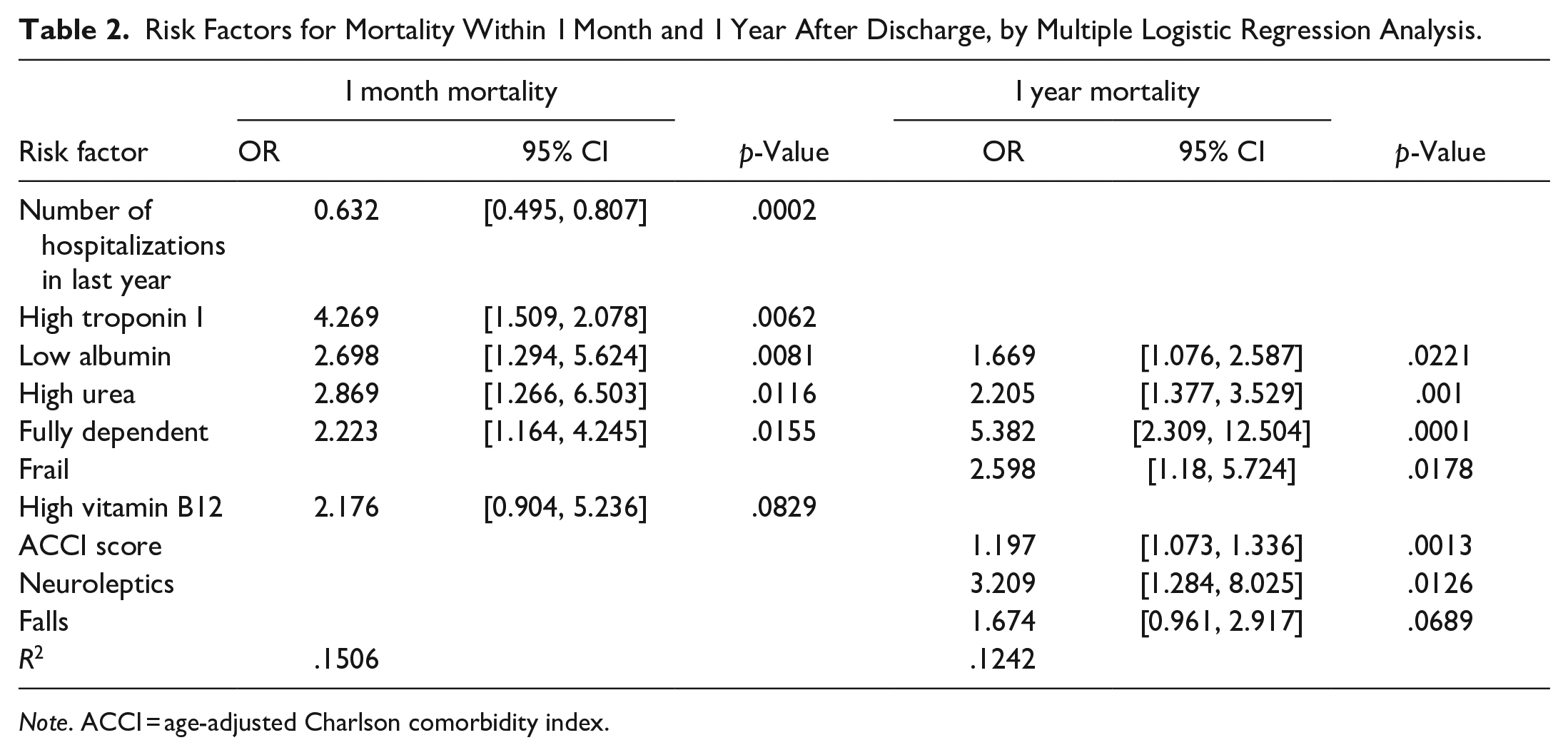
Note. ACCI = age-adjusted Charlson comorbidity index.
By Cox unadjusted and adjusted regression analysis, some risk factors predicting survival over a period of 14-year follow-up after discharge from the hospital, are shown in Table 3. In an unadjusted analysis, post-discharge mortality hazard ratio was increased for a longer hospital length of stay, higher number of comorbidities, higher CCI and ACCI scores, dependent and frail functional status, the comorbidities CVA, CRF, CHF, IHD, anemia and dementia, neuroleptic drug treatments, low hemoglobin and low albumin, and high urea, creatinine, troponin I, and vitamin B12. After adjustment for other predictors in the Cox analysis, the risk factors, which were still associated with higher hazard ratio for post-discharge mortality, were ACCI, poor functional status, the comorbidities anemia and dementia, neuroleptic drug treatments, low albumin, high urea, and high vitamin B12. By Kaplan Meier analysis, the impact of functional status, high urea, low albumin, and high vitamin B12 on post-discharge mortality, is illustrated in Figure 1(a–d).
Fourteen-Year Survival by Cox Proportional Hazards Regression.

Note. CCI = Charlson Comorbidity Index; ACCI = age-adjusted Charlson Comorbidity Index; high vitamin B12 = >666 pmol/L; low albumin = <3.5 g/dl; low cholesterol = <150 g/dL; high troponin I = >15.6 pg/mL; low hemoglobin = <13.5 g/dL; high creatinine = >1.17 mg/dl; high urea = >43 mg/dl.

Kaplan Meier cumulative 14 year survival curve: (a) by functional status, (b) by urea, (c) by albumin, and (d) by vitamin B12.
Discussion
Very few studies have evaluated predictors of mortality in nonagenarian patients in internal and geriatric departments (Bień et al., 2015; Conde-Martel et al., 2012. Saint Jean et al., 1993; Sonnenblick et al., 2007; Zafrir et al., 2010). Prognosis of oldest-old patients may be poor after they are discharged from hospital, especially in those with severe comorbidity (Matzen et al., 2012; Oeyen et al., 2017). Acute medical conditions, requiring emergent hospitalization, is frequently followed by high rate of progressive physical decline and increased mortality after discharge (Iwata et al., 2006).
Like in the Spanish study of community dwelling nonagenarians (Formiga et al., 2007, in this study, there was no difference between genders in post-discharge mortality. In some other studies (Matzen et al., 2012; Walter et al., 2001), mortality was greater in men, maybe because in those studies patients were younger.
It is important to consider clinical and functional domains, when assessing a prognosis in older patients as well as being aware of the complexity of predicting mortality in the older patients (Ponzetto et al., 2003). The CCI is the most widely used method for predicting patient mortality based on comorbidity data (Needham et al., 2005). ACCI in this study, was a significant independent predictor of mortality within 1 year and of long-term survival, similarly to the J. X. Lin et al.’s (2019) finding. In some other studies, higher comorbidity score was significantly associated with lower long-term survival (Conde-Martel et al., 2012; Iwata et al., 2006; Matzen et al., 2012; Zekry et al., 2011).
In a few studies in nonagenarian patients, hypoalbuminemia and functional loss were factors associated with mortality within 1 year and with long-term survival after hospitalization due to acute medical illnesses (Conde-Martel et al., 2012; Matzen et al., 2012). In this study, low albumin, high urea, and dependency were independent risk factors for mortality within 1 month and 1 year after discharge. Mortality risk within 1 year after discharge was lower in patients with a higher level of albumin, correspondingly to some studies (Abd-Elraheem et al., 2019; Conde-Martel et al., 2012; Zafrir et al., 2010).
Serum albumin plays a vital physiologic role in health maintenance for many organs. Hypoalbuminemia, in medical ward, usually reflects disease severity and has prognostic implications. Studies conducted within communities, hospitals, and long-term care institutions reveal a strong inverse correlation between serum albumin level and the risk of subsequent morbidity and mortality. Hypoalbuminemia might also be a marker of an acute condition (Sullivan, 2001), and an indicator of poor nutritional status, both of which might contribute to negative prognosis (Corona et al., 2017; Sullivan, 2001). Therefore, hypoalbuminemia should not go unnoticed (Cabrerizo et al., 2015).
The combination of acute and chronic diseases in the aging individual often results in disabilities and limitations in activities of daily living (Matzen et al., 2012). Patients, with functional decline, are at risk for adverse health outcomes, such as institutionalization and death (Buurman et al., 2012; Matzen et al., 2012). Functional limitations are associated with mortality in patients with hip fractures, pulmonary infection, and acute disease (Matzen et al., 2012). It should be kept in mind that the patients in the present study were discharged from acute geriatric ward. In this study, functional status, diagnosed at admission, was an independent risk factor for short- and long-term mortality, correspondingly to other studies (Buurman et al.,2012; Incalzi et al., 1992; Conde-Martel et al., 2012; Matzen et al., 2012; Minicuci et al., 2003; Narain et al., 1988; Walter et al., 2001; Zafrir et al., 2010), and in contradiction to Iwata et al.’s (2006) finding. In an Italian study, those patients, who were severely/totally dependent at admission, were 2.8 times more likely to die within 1 year after discharge (Minicuci et al., 2003). Consistently with other studies, functional status in the present study, adds important information about risk for 1-year mortality, beyond that provided by medical diagnoses or physiologic measures. This is probably because functional status reflects the severity and end-result of many different illnesses and psychosocial factors (Walter et al., 2001). Preventing functional decline, during and after hospitalization, is therefore, an increasingly important health-care focus in older hospital patients (Buurman et al., 2012).
Serum high urea, in this study, was an independent risk factor for post-discharge mortality. The association between urea and mortality may be explained by the direct negative effects of renal dysfunction on multiple organ systems or may reflect generalized decreased tissue perfusion (Ponzetto et al., 2003). On-admission raised serum urea appears to be an independent variable for predicting mortality, and it has been shown to correlate with mortality in acute stroke, pneumonia, and gastrointestinal hemorrhage (Lewis et al., 2006).
In community nonagenarians, relationships between functional independence and cognitive function, and extended lifespan have been recently found. In Pancani et al.’s (2022) study, impaired cognitive function and loss of functional independence were the stronger predictors of mortality. Some studies have suggested that dementia adversely influences clinical outcomes in patients hospitalized for acute diseases (Guijarro et al., 2010; Sampson, et al., 2009). In Narain et al.’s (1988) study, dementia was associated with mortality within 6 months after discharge from hospital, and in some other studies, within 1 year after discharge (Incalzi et al., 1992; Zafrir et al., 2010). However, in the present study, similarly to some other study findings (Shami et al., 2019; Walter et al., 2001; Zekry et al., 2011), dementia was not associated with mortality within 1 month and within 1 year. Nonetheless, a follow up for a longer period showed that dementia had a significant impact on the survival, presumably hinting that dementia might be found a risk factor for mortality in the long run follow-up, a period which could catch some more demented patients.
Anemia is a common problem in hospitalized older patients, and is recognized as a risk factor for a significant number of adverse outcomes, such as mortality, falls, cognitive impairment, and decreased physical performance. Data on the effect of anemia on mortality after discharge are limited (Joosten et al.’s, 2016) In the present study, anemia was not a risk factor for mortality within 1 year, as opposed to Joosten et al.’s (2016) finding. However, like in Bien et al.’s (2015) study, anemia decreased survival. In Fabjan et al.’s (2019) study, anemia at admission was associated with long-term mortality in patients suffering from acute ischemic stroke. In another study, anemia at admission was not significantly associated with mortality in patients discharged after acute coronary syndromes, but was associated with decreased survival for patients who had consistent anemia or new-onset anemia at discharge (Fabjan et al., 2019). The substantially greater effect of anemia at discharge on mortality suggests that this is a much more important determinant of outcome than the presence of anemia at admission (Vaglio et al., 2005), and emphasizes the importance of correcting hemoglobin level during hospitalization.
Neuroleptics, also known as antipsychotic medications, are used to treat and manage symptoms of many psychiatric disorders (Ameer & Saadabadi, 2022). In the present study, no drugs were found to be independent risk factors for mortality within 1 year after discharge. However, by Cox Regression analysis, neuroleptics use predicted a lower survival within 14 years. Studies on the effect of different types of antipsychotics (conventional and atypical) on death risk in demented patients have inconsistent results (Zhai et al., 2016). In Mooney et al.’s (2005) study, patients discharged with antipsychotics were 1.6 times more likely to die within 1 year after discharge than those not discharged on antipsychotics. A meta-analysis of 15 randomized placebo-controlled trials indicated an increased risk for deaths in patients with dementia receiving atypical antipsychotic drugs (Zhai et al., 2016). A meta-analysis of 17 randomized trials in 2,387 patients, with dementia or at risk of delirium, did not confirm that conventional antipsychotics have a higher mortality rate than placebo (Hulshof et al., 2015).
There are several likely mechanisms by which antipsychotics may increase the risk of death. Antipsychotics may prolong the QT interval, predisposing patients to arrhythmias and sudden cardiac death. Additionally, sedation and accelerated cognitive decline, caused by antipsychotics, may increase the risk of aspiration and choking, especially in patients with dementia (Gurevich et al., 2012).
High vitamin B12 level, in the present study, was marginally significant predictor of mortality within 1 month and within 1 year. However, it was a significant predictor of long- term survival. In many studies, performed on the aged, the focus is usually on detecting vitamin B12 deficiency (Dali-Youcef & Andrès 2009). In contrast, little is known about the meaning of high vitamin B12 levels. High vitamin B12 levels, as a predictor of increased mortality in malignancies and liver disease, have been already documented (Arendt et al., 2013; C. Y. Lin et al., 2010). In several studies, high vitamin B12 levels, in older patients without malignancy, were associated with higher mortality (Flores-Guerrero et al., 2020; Salles et al., 2005, 2008; Shahar et al., 2001; Tal et al., 2010; Wolffenbuttel et al., 2020; Zeitlin et al., 1997). Serum vitamin B12 concentrations can increase as a result of acute and chronic illness. Several hypotheses have been postulated regarding the mechanism behind vitamin B12 increase, including an increased release of cellular cobalamin, for example, in liver disorders during hepatic cytolysis, or a reduction of cobalamin clearance by a damaged liver (Wolffenbuttel et al., 2020).
Our study has all the disadvantages of a retrospective observational study. We must point out that we have contributed to the medical knowledge regarding nonagenarian population, whose proportion in the geriatric population is recently significantly increasing. Our study strength lies in being the first study to identify predictive factors for post-discharge mortality in the nonagenarian patients during a very long follow-up of 14 years.
Conclusion
The medical staff in the geriatric departments should strive to correct maximum risk factors, like low albumin and anemia as well as prevent unnecessary neuroleptics use and improve functional parameters. Optimal treatment of the condition due to which the patient has been hospitalized and of the medical complications that occurred during hospitalization, while preventing functional decline, might secure longer post-discharge survival.
Footnotes
Acknowledgements
I would like to thank Felicia Stern, PhD, RD for her assistance in the preparation and editing of this manuscript.
Author Contribution
I am the only author.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.