
Abstract
While non-pharmacological interventions could positively impact mood and behaviors of nursing-home residents who are living with dementia, some facilities are more willing to adopt such interventions than others. This study investigated the characteristics of Medicaid-funded nursing facilities that were associated with their willingness to implement a non-pharmacological intervention, personalized music. Using the publicly-available dataset (aka LTCfocus) from Brown University, this study examined characteristics of nursing homes in Virginia that have implemented or are in the process of implementing a personalized music intervention (n = 59) and that have decided not to implement it (n = 216). The findings indicate that nursing facilities with a higher proportion of long-term residents are more likely to implement the intervention. The findings can inform future research recruitment strategies. In addition, a greater understanding of the use of non-pharmacological interventions in relation to the characteristics of nursing facilities offers insight to policymakers and public health officials regarding resource allocations to facilities.
Introduction
Recruiting nursing facilities to participate in research is challenging even when research offers an easy to implement, non-pharmacological intervention (NPI) that could positively impact residents’ mood and behaviors. The use of NPIs has been encouraged as an alternative to antipsychotic medications to treat some challenging symptoms experienced by nursing facility residents living with dementia (Álvarez-Jiménez et al., 2008; Ihara et al., 2019). Some nursing facilities, however, are more willing to adopt new NPIs than others. This is an example of the phenomenon of self-selection bias in non-randomized studies which Larzelere et al. (2004) caution is the most critical threat to making valid causal inferences in intervention research. Bender et al. (2014) note that self-selection bias can cause a substantial difference in socioeconomic characteristics (e.g., age, income, or education) between participants and non-participants in NPIs. A well-conducted randomized design is expected to mitigate self-selection bias but is rarely used in intervention research for ethical or pragmatic reasons (Larzelere et al., 2004). More complications ensue when a research design involves two levels of analyses: nursing facilities and nursing facility residents (Bifulco, 2002). Although evaluators may design a study with nursing facility residents as the unit of analysis and randomly assign residents to the intervention and control groups within a facility, it may be impractical and unethical to recruit some nursing facilities as part of the control group without giving any treatment to their residents. Thus, the induction of self-selection bias in the multilevel research design of NPI studies is unavoidable and needs to be further examined (Kaur et al., 2020).
The personalized music intervention project utilizing the Music & Memory® program (Music & Memory, 2022) that is discussed as the NPI in this paper is an example of this two-level type of research design, which attempts to randomly select nursing facilities and randomly select resident participants within facilities. Self-selection bias may affect the facility’s willingness to participate in this type of research study. This paper investigates the characteristics of nursing facilities that are associated with staff willingness to implement the personalized music intervention for residents living with dementia and distinguishes between nursing facilities that opted for this music program NPI and those that decided not to participate in the intervention project.
NPIs as Culture Change
Nursing facilities are an essential component of contemporary long-term care systems. In the United States, the nursing facility industry includes more than 15,000 public (7%), nonprofit (28%), and for-profit (65%) organizations (Martin et al., 2021). The U.S. government spent $172.2 billion on public programs at nursing facilities and continuing care retirement communities in 2019 (Martin et al., 2021). Medicaid and Medicare programs are the major revenue source for those nursing facilities even though most nursing facilities are for-profit (Kaiser Family Foundation, 2017; Martin et al., 2021). Typically, Medicare covers short-term, post-acute care residents and Medicaid covers long-term residents (Grabowski & Mor, 2020). These public programs typically require the funded organizations to comply with complex regulatory and reimbursement regimes (e.g., licensure, certification, inspections or sanctions) which can inhibit the nursing facilities initial response to environmental change (Song et al., 2020). The long-term care industry is further constrained by issues including low wages, limited or no health benefits, heavy workloads, high turnover rates, and job dissatisfaction, leading to disparities in quality of care (Chisholm et al., 2018; Deutschman, 2005).
Given the challenges that nursing facilities encounter, a fundamental cultural change that systematically addresses such constraints is likely needed to achieve sustained quality of care (Miller et al., 2018). The “culture change” movement is an effort to alleviate those constraints and improve both quality of care and quality of life (Koren, 2010). The movement seeks to fundamentally transform nursing facilities from institution-based organizations to person-centered homes and empower staff to enable inclusion and involvement of family and community (Koren, 2010). An ideal facility features the following characteristics: resident direction, homelike atmosphere, close relationships, staff empowerment, collaborative decision making, and quality-improvement processes (Koren, 2010). Of those characteristics, resident direction (encouraging residents to make their own choices), close relationships (among staff, family, residents, and community members) and homelike atmosphere (shifting from an institution-like environment to a home-like environment) are frequently studied by researchers (Shier et al., 2014). Several nursing facilities that incorporate systemic culture change include Green House, Wellspring, Planetree, and the Eden Alternative which have implemented NPI programs (Grabowski et al., 2014). Person-centered NPIs, including those involving music, sensory stimulation, simulated presence, validation therapies, and exercise, have been shown to effectively improve or maintain quality of living or reduce emotional or cognition disorders among nursing facility residents (Meyer & O’Keefe, 2020). Therefore, the implementation of NPIs is critically important for nursing facilities.
Determinants of Willingness to Implement NPIs
Prior studies indicate that nursing facilities with certain characteristics exhibit disproportional motivation to implement NPIs to facilitate organizational change. For example, not-for-profit, large, or faith-based nursing facilities are more likely to implement NPIs than for-profit and small nursing facilities (Grabowski et al., 2014). Nursing facilities with a special care unit (SCU) of some type, fewer Medicaid residents, or higher share of private-pay residents are also more willing to participate in mission-driven programs (Grabowski et al., 2014). Whereas, nursing facilities that serve predominantly Medicaid residents have limited resources such as fewer nurses, lower occupancy rates, and more health-related deficiencies (Álvarez-Jiménez et al., 2008), which limits their ability to participate in NPIs (Grabowski et al., 2014; Mor et al., 2004). At the state policy level, studies suggest that more generous policy-based incentives are associated with increased NPI implementation such as state reimbursement reform or pay-for-performance (Chisholm et al., 2018; Miller, Cohen, et al., 2014; Miller, Looze, et al., 2014). For example, nursing facilities in Kansas that participated in the first year of a Medicaid pay-for-performance program, PEAK 2.0, were not-for-profit, were part of continuing care retirement communities, and had higher occupancy rates and greater quality of care (Hermer et al., 2018).
In short, there is a gap in the literature establishing the specific nursing facility characteristic(s) that lead to or limit the adoption of NPIs, specifically a personalized music intervention. This present study aims to bridge the gap by examining characteristics of nursing facilities that are associated with their staff’s willingness to implement a personalized music intervention for residents living with dementia, and also to distinguish between nursing facilities that opted for the personalized music NPI and those that decided not to participate in the music project.
Methods
Sample
This study examines uptake of a personalized music intervention program by nursing facilities funded by Medicaid in Virginia. The personalized music intervention program aims to help participating residents customize their own music playlists, including favorite songs, artists, and music, and listen to the personalized music for 30 min at least twice a week for 4 weeks. Nursing facility recruitment for the program included random selection of 50% of Medicaid-funded facilities in Virginia. These facilities were invited to participate in an NPI program, but some declined to participate and others never responded to recruitment efforts. The recruitment strategy then shifted from complete randomization to an attempt to contact and recruit every Medicaid funded facility in Virginia. Those facilities that agreed to participate became part of the study, thus perpetuating self-selection bias.
The present paper compares characteristics of Medicaid-funded nursing facilities in Virginia where staff have implemented or are implementing a personalized music intervention (n = 59) to those where staff declined or showed no interest in such an intervention after we left recruitment messages or sent emails (n = 216). On average, the participating nursing facilities have 117 beds (SD = 50), and the non-participating nursing facilities have 112 beds (SD = 57), with no statistically significant difference between the two groups. The sample facilities are similar in size to the overall Virginia nursing facility profile (N = 275) with an average of 113 beds (SD = 56).
Data
Data for facility characteristics were obtained from the Brown School of Public Health’s “Long-Term Care: Facts on Care in the U.S.” (aka LTCfocus) website (Brown University, n.d.). The latest version of the LTCfocus data is 2018. LTCfocus gathered data from a variety of primary and secondary sources, including the Minimum Data Set (MDS), the Online Survey Certification and Reporting (OSCAR) system, the Certification and Survey Provider Enhanced Reporting (CASPER) system, and state policy surveys. Only Medicare- and Medicaid-certified nursing facilities are included in the dataset. The dataset arranges variables across six categories: Acuity, Facility, Facility Identification, Quality, Residents, and Staffing. The variables selected for analysis are relevant to facility type (e.g., presence of Alzheimer’s disease special unit, whether or not facility is for-profit), facility staffing (e.g., licensed practical nurse hours per resident day, certified nursing assistant hours per resident day), quality (e.g., risk-adjusted successful discharge rates to community within 100 days, proportion of long-stay residents with daily pain), and residents (e.g., proportion of all admissions during the calendar year that were from the community). Table 1 summarizes the 26 variables used in this study.
Variable Definition.

All statistical analyses were performed using Stata/MP 14.0. Chi-Square Test of Independence were conducted for categorical variables and an independent samples t-test for continuous variables. The distributions of each variable of the Virginia nursing facility population, the participating nursing facilities, and the non-participating nursing facilities are available upon request.
Results
Comparison of Participants and Non-Participants
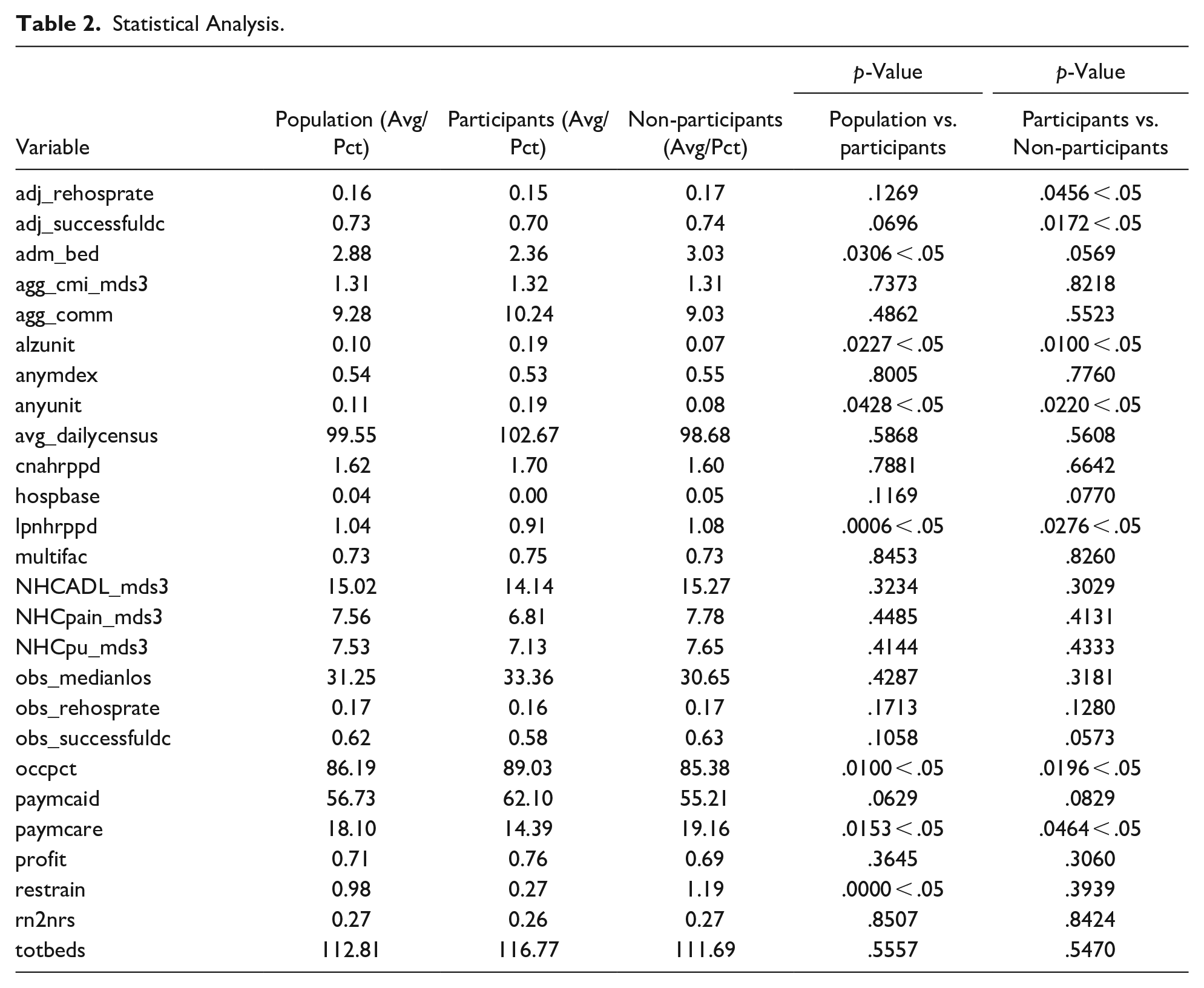
Comparisons of participating and non-participating nursing facilities showed statistically significant differences. Participating facilities are more likely to have lower rehospitalization rates within 30 days (adj_rehosprate) (p = .046), lower successful discharge rates to community within 100 days (adj_successfuldc) (p = .017), the presence of an Alzheimer’s disease special care unit (alzunit) (p = .010 < .05), the presence of a special care unit (anyunit) (p = .022), a lower number of licensed practical nurse (LPN) hours per resident day (lpnhrppd) (p = .028), a higher rate of occupied beds (occpct) (p = .020), and a lower proportion of facility residents whose primary support is Medicare (paymcare) (p = .046), as compared to non-participating nursing facilities (see Table 2). For the rest of the variables, statistical significance was not observed.
Statistical Analysis.
Sample Representativeness
Table 2 (population vs. participants) illustrates that, compared to the general Virginia nursing facility population, participating nursing facilities are underrepresented in admission rates (adm_bed) (population = 2.88 vs. participating nursing facilities = 2.36, p = .030), licensed practical nurse (LPN) hours per resident day (lpnhrppd) (p = .000), proportion of facility residents whose primary support is Medicare (paymcare) (p = .015), and proportion of facility residents who were restrained (restrain) (p = .000). The participating nursing facilities are over-represented in having an Alzheimer’s disease special care unit (alzunit) (p = .022), having any special care unit (anyunit) (p = .043), and occupied beds rates (occpct) (p = .010). For the rest of the variables, statistical significance was not observed.
Discussion
A personalized music intervention can promote nursing facilities’ culture change as it is a person-centered NPI that is expected to reduce the effects of emotional or cognition disorders among nursing facility residents and improve the quality of their lives (Meyer & O’Keefe, 2020). Being able to identify which facilities are more likely to be willing to or reluctant to adopt such an NPI would help strategize an approach to encourage them to implement NPIs. The study examined the characteristics of nursing facilities that are associated with staff willingness to use the personalized music intervention for residents living with dementia.
The findings indicate that facility staff willingness to implement a personalized music intervention is less about facility staffing and more about the facility itself and the quality of that facility. The only significant staffing variable shown in the study was the number of LPN hours per resident, per day (lpnhrppd). The facilities willing to implement the personalized music intervention program had fewer LPN hours per resident, per day in comparison both to facilities that declined the music intervention program and the general Virginia nursing facility population, though there was not a difference between Certified Nursing Assistant (CNA) hours per resident, per day. These results are aligned with results from Deutschman (2005) and Chisholm et al. (2018) in that the constraints of Medicaid and Medicare programs within facilities can result in heavy workloads for staff. Similarly, our findings indicate that the facilities participating in the music study had lower rates of residents who are supported by Medicare (paymcare) in comparison to both non-participating facilities and the general Virginia nursing facility population, which indicates that facilities that were more open to adopt NPIs have more long-term residents. There was not a significant difference between groups in Medicaid resident rates (paymcaid).
Other significant variables describing the facility itself indicated that facilities that implemented our music program had fewer average admissions (adm_bed) compared to the total Virginia facilities (with this effect trending in significance in comparison to facilities declining to participate in our music program). Our participating facilities also had more Alzheimer’s disease SCUs (alzunit) and SCUs in general (anyunit) in comparison to both non-participating facilities and Virginia facilities overall. Findings from Grabowski et al. (2014) were similar to our findings in that facilities having some type of SCU are more willing to participate in voluntary programs. Lastly, our music program facilities had higher occupancy rates in comparison to both non-participating facilities and Virginia facilities overall. While this finding might appear counterintuitive, higher occupancy rates generally indicate that a facility has greater resources and higher quality of care (Grabowski et al., 2014; Hermer et al., 2018; Mor et al., 2004).
Regarding the quality-related variables, our participating facilities had lower rehospitalization rates (adj_rehosprate), and lower successful discharge rates meaning more long-term stays (adj_successfuldc) in comparison to non-participating facilities, with the latter variable only trending in significance in comparison to Virginia nursing facilities. Our facilities had lower restraint rates (restrain) in comparison to Virginia facilities overall. Interest in the intervention among staff at a facility with a lower restraint rate might be associated with a culture of respecting residents’ autonomy and dignity, which is consistent with the personalized music intervention’s goal of person-centered care. Overall, it is important to note that our music program did not cause a change in these facility qualities. Rather, these qualities provided a facility environment that was more conducive to adding our music program.
The presence of an Alzheimer’s disease unit, lower LPN staffing, and higher bed occupancy rates suggest a busy work environment. In such settings, a personalized music intervention might be perceived as a useful tool to adopt given its wide and effective use among people with dementia and its reported efficacy in improving residents’ mood and behaviors. Because Medicare does not cover long-term care stays, having fewer Medicare-supported residents may be associated with having more residents with chronic conditions who are more likely to benefit from this type of intervention. Medicare residents are often in the facility for rehabilitation purposes and facility staff may not see them as the best candidates for a personalized music intervention. While these findings shed light on the characteristics of nursing facilities most likely to participate in a specific NPI, a music program, these findings can also inform future recruitment efforts to reach facilities that were not previously interested in NPIs. One important detail to consider, however, is that resource limitations encountered by these facilities remain a core obstacle to the addition of NPIs.
There are policy implications associated with this study. Previous studies show that more resources in the form of generous policy-based incentives are associated with increased NPI implementation (Chisholm et al., 2018; Miller, Cohen, et al., 2014; Miller, Looze, et al., 2014). If a substantial reason why some facilities avoid NPIs is related to complex regulatory and reimbursement regimes of federal and state-wide public programs at their facility, then an important future direction would be to communicate the numerous findings regarding the efficacy and benefits of NPIs to state and federal lawmakers and/or public health officials, with the goal of building funding for NPI adoption into these public programs. Doing so would create an atmosphere where facilities may feel more comfortable adjusting their facility environment for NPIs, without the threat of regulatory sanctions. While facility staff may be intrinsically interested in NPIs, the lack of comfort at the organizational-level within facilities is not conducive to staff motivations and interest in NPI implementation.
There are a few limitations that should be noted. First, this study focused on nursing facilities in Virginia. Although there are federal nursing home regulations, there may be variations in rules, incentives, and waivers across states, thus requiring caution when applying the study findings to nursing facilities outside Virginia. Second, the findings are based on nursing facilities responses to our recruitment for a specific NPI, a personalized music intervention. Their responses might have been different for different types of NPIs.
Footnotes
Authors Note
This manuscript will not be submitted, in part or entirety, elsewhere for publication before the decision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data used for this study came from two sources: the LTCfocus data (publicly available nursing facility characteristics) and the administrative recruitment record for our larger intervention research, which was supported by the Virginia Department of Medical Assistance Services (Contract #10055).
Ethical Approval
This study was approved by George Mason University IRB (reference number: 1360973-16).