
Abstract
Keywords
The Hispanic population in the United States (US) continues to grow. The Pew Research Center estimates that by 2050, 128 million Hispanics will be living in the US, and Hispanics of Mexican origin account for 62% of the Hispanic population (Noe-Bustamante et al., 2019; Passel & Cohn, 2008). Hispanics in general have lower income, and worse educational and occupational opportunities than Non-Hispanic Whites (NHWs) (Gallo et al., 2009). Education and income are social determinants of health behaviors and outcomes (Langellier et al., 2020). In a systematic review and metanalysis, Khaing et al. (2017) found that groups with low education and income are at higher risk of coronary heart disease, cardiovascular events, strokes, and cardiovascular deaths when compared with groups with high education and income.
For more than a century, cardiovascular disease (CVD) has been the leading cause of death in the US (Mozaffarian et al., 2015). CVD risk is determined by non-modifiable and modifiable risk factors. The most studied modifiable risk factors are hypertension, dyslipidemia, diabetes, obesity, and smoking (Balfour et al., 2016). The Hispanic Community Health Study/Study of Latinos (HCHS/SOL) has reported that the prevalence of hypertension is 2% to 3% lower in Mexican Americans (MAs) when compared to NHWs, while the prevalence of dyslipidemia and diabetes is higher in MAs (Daviglus et al., 2014). The American Lung Association analyzed data from the 2015 National Health Interview survey and found that 10.1% of MAs were current smokers compared to 16.6% of NHWs (American Lung Association, n.d.). Using data from the National Health and Nutrition Examination Surveys, Fryar et al. (2018) reported that MAs have a higher mean waist circumference than NHW.
Research suggests that the presence of cardiovascular risk factors (CVRF) has negative effects on cognition. Hypertension increases the risk of vascular cognitive impairment and Alzheimer’s disease, and typically affects executive function, motor speed, and attention domains (Iadecola & Gottesman, 2019). Higher neurodegeneration present in diabetics have been associated with lower performance in memory and executive function tests (Frison et al., 2021). Central obesity, quantified by waist circumference, has been also associated with cognitive impairment and dementia (Tang et al., 2021), and impaired performance in various domains including episodic memory, executive function, decision making, and verbal learning (Dye et al., 2017). Another common CVRF, dyslipidemia, has also been associated with decline in memory and visual perceptual/constructional tests (Przybycien-Gaweda et al., 2020). Compared to non-smokers, individuals who are smokers have poorer performance on processing speed, attention, memory, and executive functions (Nadar et al., 2021).
Despite having higher rates of poverty, less education, and less access to health care services, Hispanics have lower mortality rates than NHWs, a phenomenon documented in the literature as the Hispanic or Latino mortality paradox (Abraido-Lanza et al., 2020). Since Markide and Coreil (1986) published the first article suggesting the existence of the Hispanic paradox, a plethora of research have been done trying to elucidate this epidemiological phenomenon, targeting may areas like cardiovascular disease (Khan et al., 2022), kidney disease (Desai et al., 2019), and cancer (Ruiz et al., 2013). There is a lack of research on the resilience of Mexican Americans to the physical effects of CVRF applied to age related cognitive decline. The goal of the present study is to compared the impact of cardiovascular risk factors on cognitive decline in cognitively normal NHWs and MAs older adults, and to evaluate if Mexican American ethnicity may be protective of cognition. We predicted that the presence of CVRF would be associated with poorer neuropsychological test scores in both ethnic groups, but the impact of CVRF will be greater in NHWs.
Methods
Settings and Study Design
We conducted a cross-sectional analysis of data from the Health and Aging Brain Study: Health Disparities (HABS-HD). The HABS-HD study methodology, including recruitment, inclusion and exclusion criteria, interview and functional exam, cognitive assessment, informant interview, imaging, and blood collection have been described in detail elsewhere (O’Bryant et al., 2021). In summary, the HABS-HD, is an ongoing longitudinal study of cognitive aging among MAs at the University of North Texas Health Science Center that has been recruiting participants since 2017. The HABS-HD study uses a community participatory research approach and recruitment methodology. Recruitment consists of community recruiters, community presentations, flyers/brochures, social media, and door-to-door recruitment. Subjects included in the study had an age of 50 and above, and a self-reported ethnicity of MA or NHW. Because of their potential impact on cognition, the next conditions are considered exclusion criteria for the HABS-HD study: type 1 diabetes, cancer diagnosis, chemotherapy, or radiotherapy in the last 12 months, severe mental illness, traumatic brain injury with loss of conscience in the last 12 months, active infection, alcohol/substance abuse, and other severe illness such as end stage renal failure or chronic heart failure.
After signing a written informed consent, HABS-HD participants undergo a clinical interview, neuropsychological assessment, functional examination, MRI of the head, and blood draw for clinical and biomarker analysis. An informant interview is conducted to assess functional level. Cognitive diagnoses are assigned using an algorithm (decision tree) that is verified at consensus review. Unimpaired Cognition (UC) = no cognitive complaints, CDR sum of boxes score of 0 and cognitive test scores broadly within normal limits (i.e., performance no more than 1.5 standard deviations below the mean of the normative range on any test).
All HABS-HD data is available to the scientific community through the UNTHSC Institute for Translational Research (ITR) website at https://apps.unthsc.edu/itr/.
Study population
From March 2017 until June 2020, 1,705 subjects were enrolled in the study baseline visit. In order to analyze the relationship of cardiovascular risk factors (CVRF) and cognition within a cognitively normal sample of NHW and MA elders, we excluded 260 participants with a diagnosis of MCI, and 116 participants with a dementia diagnosis. Of the remaining 1,329 subjects, 34 did not have all the variables of interest and were excluded from the analysis. The final sample was composed of 1,295 cognitively normal subjects (663 NHWs and 632 MAs).
Predicting variables
Hypertension was classified via self-reported medical history, use of blood pressure-lowering drugs, and/or average of two blood pressure measurements >140/90 mm Hg. Self-reported medical diagnosis, current use of insulin or oral hypoglycemic agents, and/or HbA1c >6.5% were used to diagnose diabetes. Participants with a medical diagnosis of high cholesterol and/or triglycerides, use of cholesterol-lowering drugs, total cholesterol >200 mg/dL, or triglycerides >150 mg/dL were diagnosed as having dyslipidemia. The category of “another cardiovascular disease” was ascertained with self-reported past history of coronary heart disease, heart failure, cardiomyopathy, atrial fibrillation, and heart valve replacement. Participants were considered current smokers if they were using cigarettes at the time of interview, ever smokers were the participants that used cigarettes at any point in their lives before the interview. To measure waist circumference, an indicator of central obesity, we located the upper hip bone and the top of the right iliac crest, and we placed a measuring tape in a horizontal plane around the abdomen at the level of the iliac crest.
Cognitive function
The Mini-Mental State Examination (MMSE) was used to assess global cognition (Gluhm et al., 2013). The Trail Making Test Part B, was used as measure of executive function (Linas-Regla et al., 2016). The Spanish English Verbal Learning Test (SEVLT) evaluated immediate and delayed memory (Gonzalez et al., 2022). The Digit-Symbol Substitution Test (DSST) ascertained processing speed (Amaresha et al., 2014).
Covariates
Demographic information including age, gender, and total years of education as reported during the interview were covariates. Plasma samples were assayed for the presence of apolipoprotein E4 allele (APOE4).
Statistical analysis
Baseline demographic data were analyzed using chi-squared tests for categorical variables, and t tests for continuous variables. Multivariate logistic regression was utilized to assess the relationship of CVRF and depression to neuropsychological test scores. Hypertension, diabetes, dyslipidemia, another cardiovascular disease, smoke current, and smoke ever were entered in the models as categorical variables (0 = absent, 1 = present). Abdominal circumference was measured in inches. MMSE raw scores were used for analyses; for Trails B, SEVLT, and DS, raw scores were transformed to z-scores to facilitate effect size comparisons. In Trails B, higher scores indicate worse performance, so we inverted the z-score before analyses. After this transformation, for all neuropsychological tests, a higher z-score indicated better performance. We conducted a multiple linear regression to analyze the association of cardiovascular risk factors with test performance, using each test score as a separate outcome. Age, sex, years of education, and APOE4 positivity were entered as covariates in the models. Statistical significance was set to p ≤ .05. All data were analyzed using SPSS version 28 for Windows (SPSS INC., Chicago, IL).
Results
Table 1 presents the prevalence rates for categorical variables, and mean and standard deviation for continuous variables of interest.
Baseline Characteristics.

Continuous variables reported as mean and standard deviation.
Categorical variables reported as number and percentage. p Values: chi square for categorical variables, and t tests for continuous variables.
Demographic characteristics
The total sample included 1,295 cognitively normal participants with a mean age of 66.06 (8.51); 663 participants (51.2%) were NHW and 632 (48.8%) were MA. Sixty four percent of the total sample were female. MAs were significantly (p < .001) younger (63.08 [7.67] vs. 68.9 [8.29]), less educated (9.84 [4.47] vs. 15.6 [2.57]) and have a higher number of females in their cohort (69.5% vs. 58.1%) when compared to NHWs.
Cardiovascular risk factors
When compared to NHWs, MAs had a higher prevalence of hypertension (64.9% vs. 58.1% [p = .001]), diabetes mellitus (34.7% vs. 11.5% [p < .0001]), and current smoking (7.4% vs. 3.6% [p = .002]). MAs also had a higher abdominal circumference mean (40.11 [5.41] vs. 39.25 [5.95]) when compared to NHW. The prevalence of another CVD (10.1% vs. 5.5% [p = .002]) and APOE4 positivity (27.7% vs. 17.2% [<.0001]), were higher in NHWs. The prevalence of dyslipidemia and ever smoking were not different between groups.
Neuropsychological tests
NHWs had higher scores in the MMSE (29.2 [1.01] vs. 27.4 [2.58]; p < .0001), and Trails B (0.27 [0.62] vs. 0.18 [0.86]; p = .003) when compared to MAs. There was no difference among MAs and NHWs in SEVLT nor DSST.
Multiple linear regression
Tables 2 and 3 show the multivariate linear regression models using CVRF as predictors of test scores in NHWs and MAs, respectively. After controlling for age, education, sex, and APOE4 status, in NHWs, other CVD predicted Trails B (B = −0.22 [B = −0.39 to −0.06]; p = .007), and DSST scores (B = −0.31 [−0.53 to 0.08]; p = .007); abdominal circumference predicted MMSE (B = −0.03 [−0.05 to −0.01]; p = 0.006), SEVLT immediate (B = −0.06 [−0.07 to −0.04]; p = .000), SEVLT delayed (B = −0.05 [−0.07 to −0.03]; p = .000), and DSST scores (B = −0.02 [−0.04 to 0.00]; p = .01); current smoking predicted MMSE (B = −0.47 [−0.88 to −0.07], p = .02) scores. In MAs, abdominal circumference and ever smoking predicted SEVLT immediate scores (B = −0.03 [−0.05 to −0.00]; p = .01, and B = −0.17 [−0.31 to −0.03]; p = .0) respectively. Hypertension, dyslipidemia, and diabetes did not predict cognitive test scores in either group. Contrary to our hypothesis, CVRF were more detrimental in cognition in NHWs that in MAs.
Logistic Regression. CVRF as Predictors of Tests Scores in NHW (n = 663).

p ≤ .05 after adjusting for age, education, sex, and APOE4 status.
Logistic Regression. CVRF as Predictors of Tests Scores in MA (n = 632).
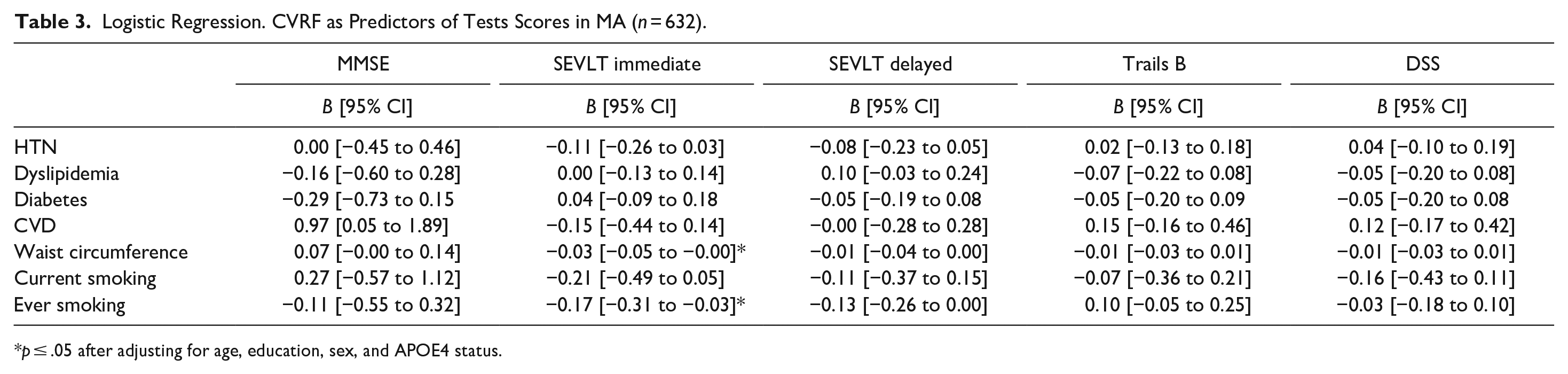
p ≤ .05 after adjusting for age, education, sex, and APOE4 status.
Discussion
This study investigated the effect of cardiovascular risk factors on cognition among MAs compared to NHWs. After adjusting for age, education, sex, and APOE4 status, our results indicated that in NHWs, other CVD (coronary heart disease, heart failure, cardiomyopathy, atrial fibrillation, and heart valve replacement) predicted Trails B and DSST scores. Abdominal circumference predicted MMSE, DSST, and both memory tests scores. MMSE scores were also predicted by current smoking. In MAs, only SEVLT immediate scores were predicted by abdominal circumference and ever smoking variables. As we predicted, CVRF were more detrimental in cognition in NHWs than in MAs. This may be explained by Mexican American ethnicity may be protective of cognition as part of epidemiological phenomenon commonly known as the Latino or Hispanic Health paradox. Some researchers reported that the advantages of the Hispanic paradox are “inconsistent and equivocal.” Teruya et al. (2013), while others, like Weden et al. (2017) concluded that foreign born MAs have half the odds of cognitive decline than their NHWs and US born MAs counterparts. The Hispanic paradox is descriptive rather than explanatory hence determination of cause requires further research.
Hypertension is a well-known risk factor for cognitive decline and dementia (Mahinrad et al., 2021). Unlike previous research (Forte et al., 2020; Walker et al., 2017), hypertension did not impact any cognitive domain in our cohort. A possible explanation for this inconsistency may be the age of hypertension initiation and hypertension duration. Also, it has been suggested that the correlation between hypertension and cognition is age dependent (Wei et al., 2018), considering the relatively low mean age of our cohort, we may have captured them at a time where cognitive performance was not yet affected.
Diabetes has been shown to be a risk factor for cognitive decline in NHWs samples (Dove et al., 2021; Frison et al., 2021), and diverse Hispanic cohorts (Elfassy et al., 2019; Gonzalez et al., 2020). The duration of diabetes and the glycemic control, which we did not account for, modulate the impact on cognition. These factors may partially explain our results.
A diagnosis of dyslipidemia did not predict cognitive test scores in our cohort. Research on the lipid-cognition association has shown mixed results. Elevated total cholesterol and triglycerides have been associated with greater decline on multiple cognitive domains (Power et al., 2018) and increased risk of dementia (Anstey et al., 2017). Similar to our results, Wendell et al. (2014) and Peters et al. (2021) reported no significant associations between total cholesterol and cognitive decline.
These differences in findings may be also explained in part by differences in methodology and study design, including mean age of participants, different cognitive assessment used, different CVRFs diagnosis criteria, use of composite scores, and different co-variates. Further research on the association of long-term hypertension, diabetes, and dyslipidemia and cognitive decline is warrant.
Our study has several limitations. First, the cross-sectional design precludes any type of casual inference. Long term follow up of the cohort will allow us to examine the relationship of CVRF and cognition through time. Second, the self-reported information, specifically for other CVD, may be affected by access to health care, which may be lower in minority populations. Third, we did not analyze the potential effects that age of diagnosis and treatment status of CVRF may have in cognition. Lastly, the analyzed data were from a MA cohort, which may limit generalizability of our findings to other Hispanic groups.
This study has several strengths like having a well-characterized cognitive normal community based-sample, and the use of neuropsychological tests that have been normed for a Mexican American population. Another strength is the administration of the interview and cognitive tests in Spanish which probably gives a more accurate measurement of cognitive status.
In conclusion, the present study provides a distinctive view of the effects of CVRF on cognition among MAs and NHWs. We examined the effect of hypertension, diabetes, dyslipidemia, abdominal circumference, smoking, and other cardiovascular disease in a sample of older MAs and NHWs. We found that cardiovascular disease, abdominal circumference, and smoking negatively impacted global cognition, executive function, and processing speed in NHW. In MA, only memory was affected by abdominal circumference and smoking. We argue that the notion of a Hispanic health paradox for cognition may be the explanation for our results. Further research of the underlying causes of these differences are warranted. Future research should include cultural factors such as family values and collectivism that are common to Mexican American. Measures of brain structure should also be considered since the impact of cardiovascular risk factors on cognition is likely related to brain changes in structure and function. Finally, future research needs to take in account the cumulative burden of cardiovascular risk factor in cognition. The necessary next step is to include other Hispanic groups to understand if these patterns apply to them, and to elucidate the factors contributing to cognitive impairment among genetically, culturally, and ethnically diverse Hispanics. Considering that many of these conditions are modifiable, these data may help to create intervention to target at-risk groups and to improve healthy brain aging in Mexican American and other ethnic groups.
Footnotes
Acknowledgements
The consent is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The research team also thanks the local Fort Worth community and participants of the HABS-HD study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sid O’Bryant has multiple patents in neurodegenerative diseases and is the founding scientist for Cx Precision Medicine, Inc. Leigh Johnson owns an interest in Cx Precision Medicine, Inc. Raul Vintimilla, James Hall, and Thomas Nevin report no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers R01AG054073 and R01AG058533.
Ethical Approval
The HABS-HD study is conducted under the approval of the North Texas Regional IRB Board, 2016-128.