
Abstract
This prospective, quasi-experimental study aims to compare healthcare resource utilization (HCRU) and costs of a multi-component care approach for older people in a community setting (intervention group (IG)) with usual care in a matched control group (CG) during a 21-month observation period. The reablement-oriented intervention included a geriatric assessment, a case and network management and digital supporting tools. Regression models were applied to determine intervention effects regarding hospitalization, total hospital length of stay (LOS), number of physician consultations, and healthcare costs using claims data. 872 subjects were included in the IG and 1,768 in the CG. The analyses showed that the intervention did not affect hospitalization (OR = 1.153; 95% CI: 0.971–1.369, p = .105). However, participating in the IG lead to a small but significant increase of physician contacts by a factor of 1.078 (Exp(ß) = 1.078; 95% CI: 1.011–1.149; p = .022). A non-significant mean difference in costs of €1,183 (95% CI: €−261.6 to €2,627.6, p = .108) per participant was identified. Further research is needed to generate robust evidence on the optimal design of care approaches for older people and the health economic implications of such interventions to improve care and resource allocation decision-making.
Keywords
Introduction
Due to aging populations (OECD, 2019), healthcare systems must cope with various challenges, especially in terms of providing care for older people (Rechel et al., 2009, 2013). Studies reveal that age-related changes in functional status, frailty and multimorbidity are associated with higher healthcare resource utilization (HCRU) and costs (Bähler et al., 2015; Bock et al., 2016; Han et al., 2019). In order to address these challenges, preventing functional decline and long-term care dependency among seniors is particularly relevant from a health economic perspective (Bloom et al., 2014; Nishi et al., 2020; Rechel et al., 2009).
“Aging in place,” enabling older people to remain in their homes and communities and stay independent, autonomous, and socially integrated has been widely acknowledged as a promising approach for healthy aging (Wiles et al., 2012). Accordingly, health systems increasingly apply preventive, integrated care interventions. The interventions are based in primary care and target community-dwelling frail older people (Eklund & Wilhelmson, 2009; Looman et al., 2019). Moreover, the concept of “reablement” represents a related approach. Reablement is mainly implemented in home and community care settings (Cochrane et al., 2016; Doh et al., 2020) and “[. . .] aims to enhance an individual’s physical and/or other functioning, to increase or maintain their independence in meaningful activities of daily living at their place of residence and to reduce their need for long-term services” (Metzelthin et al., 2022). Evidence regarding positive effects of reablement-based interventions on health-related outcomes for seniors is inconsistent (Aspinal et al., 2016; Sims-Gould et al., 2017; Tessier et al., 2016). However, some studies have demonstrated changes in HCRU in terms of reduced utilization of emergency departments or unplanned hospital admissions resulting in cost savings (Lewin et al., 2013, 2014; Tinetti et al., 2012).
In recent years, analyses on the basis of statutory health insurance (SHI) claims data have become increasingly important in the context of health services research, as they reflect real-world healthcare provision and thus provide valuable information for decision-makers (Kreis et al., 2016). Due to their properties, they allow the examination of possible shifts in health care demand, for example, as a result of the introduction of new care approaches. While reablement-based interventions are already implemented in various countries (Clotworthy et al., 2021), they have not been implemented in the German healthcare system. Thus, evidence from Germany regarding (health economic) effects of reablement-based interventions preventing functional decline and care dependency for community-dwelling older people is lacking. Therefore, this analysis examines the effects of a complex intervention for older people regarding HCRU and total costs by using SHI claims data.
Methods
Study Design
The analysis is based on a prospective, quasi-experimental study that was conducted in the district of Hamburg-Eimsbuettel (Hasemann et al., 2022). The study was initiated by German SHI companies (Techniker Krankenkasse, Barmer, DAK Gesundheit, Knappschaft) and started in 2017 in cooperation with the Center for Geriatrics and Gerontology (Albertinen Haus, Hamburg), Bielefeld University (Department of Health Economics and Health Management), Johanniter-Unfall-Hilfe e.V. (Regional Association Hamburg), CIBEK technology + trading GmbH, NXI GmbH & Co. KG, and VDI/VDE Innovation + Technik GmbH. SHI companies provided pseudonymized claims data covering the 21-month observation period and the year prior to inclusion. We compared participants of the intervention group (IG) with a matched control group (CG), who received usual care. The recruitment process was administered by the SHI-companies, who contacted eligible participants by letter. While participants for the IG were recruited in the pilot region, potential controls (CG) were contacted in urban areas that were comparable to the pilot region in terms of socio-demographic and infrastructural aspects. Participants were eligible if they gave written informed consent, were ≥70 years and had an increased risk for loss of independence measured by the LUCAS functional ability index (LUCAS-FI). Accordingly, participants classified as postROBUST, preFRAIL, and FRAIL (Dapp et al., 2014) were considered. Exclusion criteria were having a long-term care grade ≥4, living in a long-term care facility and not having fluent German language skills. After recruitment, control subjects were assigned to each intervention participant via exact matching based on the following criteria: LUCAS-FI/long-term care grade, year of birth, gender, marital status, number of people living in the household. To improve the precision of estimations, the IG to CG matching ratio was chosen to be 1:2 (Austin, 2010). The study protocol followed the ethical principles of the Helsinki declaration and was approved by the Ethics Commission of the General Medical Council Hamburg (PV548).
Intervention
The intervention was inspired by the concept of reablement (Metzelthin et al., 2022) and combined elements of health and social care by building a community-based network to assist and support older people and their relatives in their homes. More specifically, an initial comprehensive geriatric assessment was conducted to identify each IG participant’s resources and risks regarding medical conditions, social aspects and physical performance. Based on this assessment, an individual support plan was developed by experts in case conferences. Intervention services further included case management consultations, expert-moderated group consultations and a network management to promote and mediate local offers in the field of health and exercise. Additionally, a digital supporting tool for personal assistance was provided. Details on the intervention are presented in the Supplemental Material (Table 1).
Outcome Measures
When analyzing HCRU, we focused on inpatient services operationalized by having at least one hospitalization, total length of stay (LOS), and outpatient services that were operationalized by the number of physician consultations per participant. We adopted a payers’ (SHI) perspective (Institute for Quality and Efficiency in Health Care, 2020) when calculating total costs, which included the following services: inpatient care, outpatient care, rehabilitative care, pharmaceuticals, therapeutic devices, non-physician specialist services (e.g., physical therapy), nursing (home) care, and patient transport services. For drug utilization, Defined Daily Doses (DDD) were analyzed by using the WidO-database (AOK Research Institute, 2021).
Statistical Analysis
Baseline characteristics of the study population and outcomes variables after 21 months were analyzed using descriptive statistics. Baseline differences between IG and CG were examined using chi-square tests and t-tests. The relationships between outcome variables and relevant covariates were investigated using various regression analyses, in which the study group variable indicated the intervention effect. We used a logistic regression model to analyze effects on hospitalization (dichotomous variable). To investigate effects on the total hospital LOS per hospitalized participant, a generalized additive model (GAM) was used. Due to the skewness of the variable, a gamma distribution was applied. For the number of outpatient physician consultations, we applied a GAM using a zero inflated negative binomial distribution. We used a linear regression model to identify possible intervention effects on total health care costs. Theoretical considerations informed the composition of the initial models. Potentially relevant predictor variables were age, gender, previous year’s Charlson Comorbidity Index (CCI) Score, number of hospitalizations, total hospital LOS, number of outpatient physician consultations, total health care costs, length of study observation, death, and using a digital device (intervention component). Since the majority of IG participants was recruited within the second half of 2018, which caused their observation period (21 months) to overlap with the COVID-19 pandemic, the time of enrollment within the recruitment period was also taken into account by means of a cluster variable. CCI Scores were based on main and additional ICD 10-diagnoses documented in outpatient and inpatient settings (Charlson et al., 1987; Quan et al., 2011). Additionally, since baseline functional status was documented by LUCAS-FI (participants without initial need for long-term care) and long-term care grade, splitting the sample into two subgroups, the variables were combined into one predictor variable. This variable divides the sample into four categories which include LUCAS-FI stages postROBUST (1), preFRAIL (2), and FRAIL (3) (Dapp et al., 2014) as well as long-term care grade 1 to 3 (4). Backward selection based on the Akaike Information Criterion (AIC) (Fahrmeir et al., 2013) was applied to receive the final regression term. When necessary, the regression term was supplemented by the study group variable in order to quantify intervention effects. Model fit and reliability of the results were assessed by diagnostic plots (e.g., residual, qq, and worm plot), density curves, receiver operating characteristics (ROC) curves, and the area under the curve (AUC). Hosmer et al. (2013) refer to an AUC of 50% to 70% as poor, 70% to 80% as acceptable, 80% to 90% as excellent, and ≥90% as outstanding discrimination. Statistical analysis was performed using the open-source R software (version 4.1.0) (R Core Team, 2020) with a significance level of 5%.
Results
After exact matching (1:2), 902 participants were included in the IG and 1,804 in the CG. Dropouts after matching in the IG (3.22%) and CG (0.39%) led to a study sample of 2,670 participants. Due to missing data or loss to follow-up, this health economic analysis involved a reduced sample of 872 (IG) and 1,768 (CG) participants (Figure 1).

Flowchart of participants.
In both groups, mean age was 80 years. 67.78% (IG) and 64.59% (CG) were female. The majority of the sample was deemed “frail” (IG: 42.09%, CG: 41.46%), followed by “postROBUST” (IG: 36.93%, CG: 38.52%), and “preFRAIL” (IG: 11.70%, CG: 12.67%), as classified by the LUCAS-FI. Less than 10% of both groups were classified to long-term care grade 1 to 3 (IG: 9.29%, CG: 7.35%). No statistically significant group differences at baseline were observed (Table 1).
Baseline Characteristics.

SD = standard deviation.
t-Test applied for continuous and Chi²-test applied for categorical variables, significance level (p < .05).
Healthcare resource utilization
During the 21-month study period, 57.68% (IG) and 52.77% (CG) were hospitalized, indicating statistical significance (p = .019). Among those, the average number of hospitalizations (mean ± SD) differed only slightly between IG (2.30 ± 1.79) and CG (2.33 ± 1.86). Mean total hospital LOS per participant was 21.66 ± 29.22 (IG) and 22.16 ± 36.49 (CG). Neither outcome measure was statistically significant (Supplemental Material: Table 2).
The regression model on having at least one hospitalization indicated that the intervention had no statistically significant impact (OR = 1.153; 95% CI: 0.971–1.369, p = .105). Significant predictors for hospitalizations were female gender, having a long-term care grade at baseline, the number of hospitalizations in the previous year, the number of outpatient physician consultations in the previous year and the length of study observation (Supplemental Material: Table 3). Whereas the binned residual plot showed no definite pattern, the ROC and the AUC of 0.66 demonstrated, that the model provided only weak discrimination of the values (Supplemental Material: Figures 1 and 2).
According to the GAM, total LOS among hospitalized IG participants was reduced by a factor of 0.754 (95% CI: 0.591–0.963) compared to hospitalized CG participants (Supplemental Material: Table 4). This effect was statistically significant (p = .023). The GAM further indicated that higher total hospital LOS is associated with LUCAS-FI categories and having a long-term care grade at baseline, CCI Score, and total hospital LOS in the year before enrollment. Lower total LOS was associated with the length of study observation. The residual plot of the regression model showed an undesirable pattern. Moreover, according to the density curves, the fitted values did not adequately represent the distribution of the observed values (Supplemental Material: Figures 3–6).
Participants in the IG had an average of 48.40 ± 24.51 physician consultations (CG: 47.87 ± 29.19, difference not statistically significant; Supplemental Material: Table 2). The regression model showed a significant intervention effect (Exp(β) = 1.078; 95% CI: 1.011–1.149, p = .022), indicating that the number of physician consultations was significantly higher (7.8%) in the IG compared to the CG. Relevant predictors of physician contacts were higher CCI Score and higher number of physician contacts in the previous year. Higher age was associated with a small decrease in outpatient physician consultations (Table 2). The residual plots indicated acceptable model estimation and the density curves demonstrated that the fitted values adequately covered the center of the empirical values (Supplemental Material: Figures 7–10).
GAM on Number of Outpatient Physician Consultations.

CCI = Charlson Comorbidity Index; CI = confidence interval.
= previous year.
Statistical significance (p < .05).
Health care costs
Average health care service utilization rates and incurred costs per participant for the IG and CG after 21 months are shown in Table 3. Significant differences occurred in non-physician specialist care services and attributable costs. Additionally, costs of outpatient care were significantly higher in the IG and costs of rehabilitative care were significantly lower in the IG. Overall, the mean total health care costs (including intervention costs) were €16,561.80 ± €21,313.94 for participants in the IG and €14,747.77 ± €24,586.94 for participants in the CG, indicating no statistically significant group difference (p = .051).
HCRU and Costs per Participant and Service of IG and CG after 21 months.
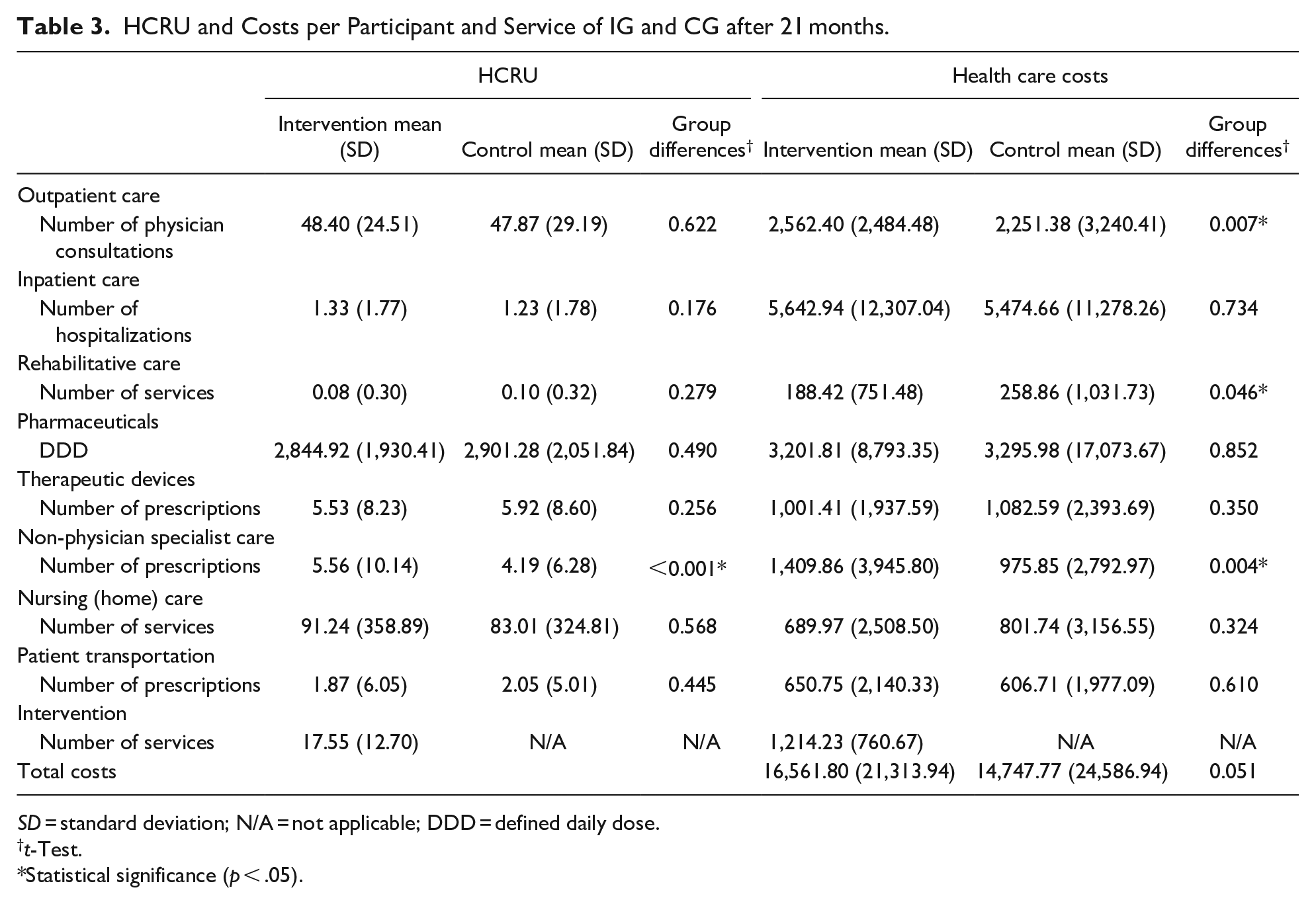
SD = standard deviation; N/A = not applicable; DDD = defined daily dose.
t-Test.
Statistical significance (p < .05).
The linear regression model (controlled for several confounding factors) showed that participating in the intervention had no significant impact on total health care costs (Table 4). For the IG, mean difference in total costs of €1,183 (95% CI: € −261.6 to €2,627.6, p = .108) per participant were identified. Statistically relevant predictor variables were gender, LUCAS-FI or long-term care grade at baseline, CCI Score, death, length of study observation, and total costs in the previous year. Density curves of the underlying data and the model estimates showed that the model can adequately capture the data (Supplemental Material: Figure 11).
Linear Regression Model Estimates for Total Health Care Costs.
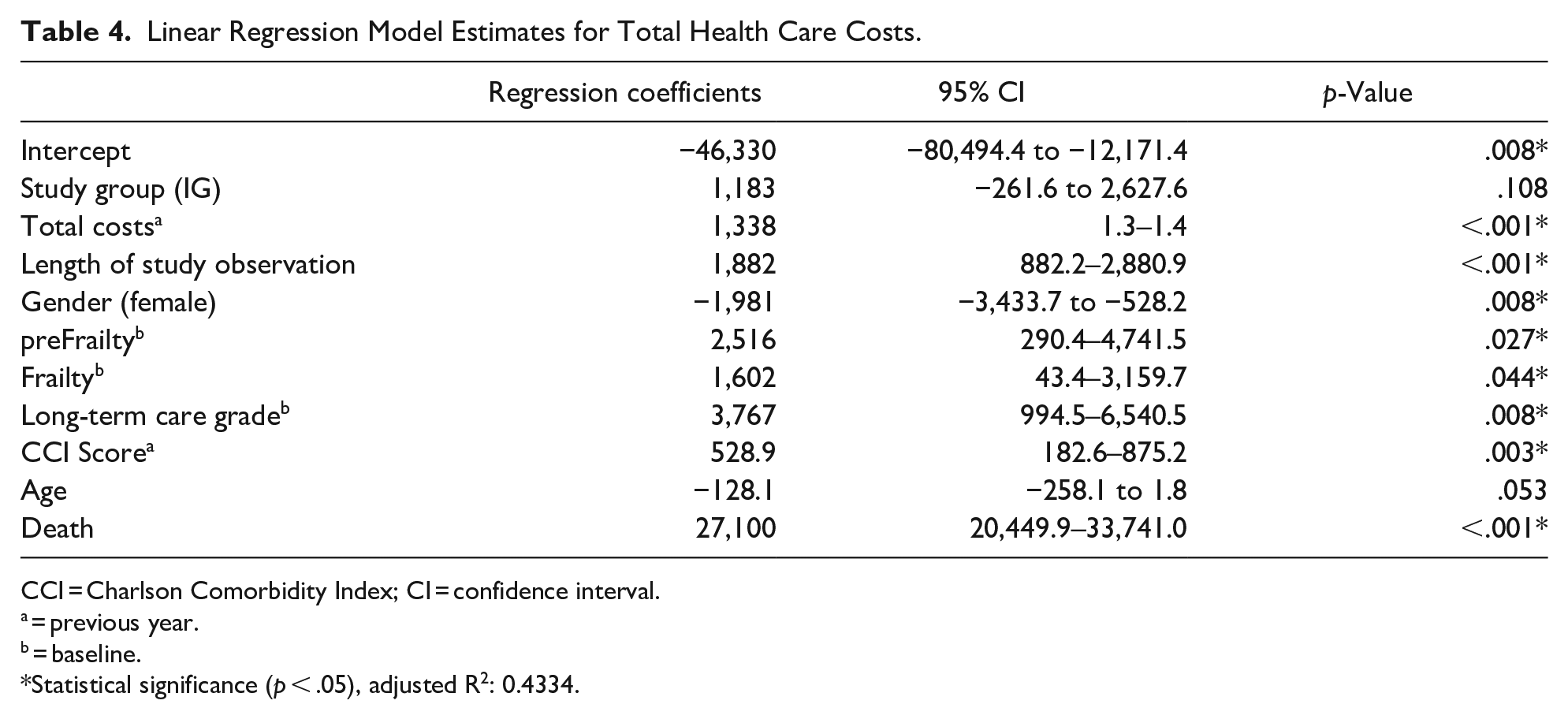
CCI = Charlson Comorbidity Index; CI = confidence interval.
= previous year.
= baseline.
Statistical significance (p < .05), adjusted R2: 0.4334.
Discussion
In this analysis, we aimed to evaluate the impact of a multi-component community-based intervention based on the reablement concept (Aspinal et al., 2016; Doh et al., 2020) for older people at risk of functional decline and long-term care dependency on HCRU and costs using SHI claims data. Regarding hospital admissions and total hospital LOS, the results suggest mixed intervention effects. However, the quality of the regression models related to hospitalization and total hospital LOS is limited. Therefore, we are unable to conclude whether the intervention leads to a change of inpatient services. In terms of outpatient services, our results reveal that IG participants had slightly higher utilization of physician consultations, which may result from improved care-coordination due to the comprehensive case management approach. However, effect size was small. With regard to total costs, no significant group differences were observed. Thus, we cannot confirm that participating in the multi-component intervention leads to a substantial change in HCRU or cost savings, as previously shown (Aspinal et al., 2016; Kjerstad & Tuntland, 2016; Lewin et al., 2013, 2014; Tinetti et al., 2012). However, the analysis does not reveal significant additional costs of the intervention. The main strengths of our study result from addressing research gaps, using promising data and methodological approaches. Thus, it provides first evidence regarding HCRU and cost effects of a community-based care intervention from a German (SHI) perspective using a comprehensive data set. By using matching and regression analyses and including potential confounder variables, a substantial effort was made to ensure comparability of the study groups.
Comparing these results to the current literature is difficult due to the heterogeneity of interventions, and outcomes investigated. Furthermore, due to different populations and settings studied, data are derived from heterogenous samples (Looman et al., 2019). Nevertheless, our findings are consistent with the inconclusive body of evidence regarding reablement-based interventions (Aspinal et al., 2016), as well as integrated and coordinated care interventions for frail older people (Eklund & Wilhelmson, 2009; Looman et al., 2019). Some studies suggest that integrated interventions can decrease HCRU and thereby reduce costs (Eklund & Wilhelmson, 2009). However, several studies also demonstrated effects in favor of the CG or were not able to show group differences (Eklund & Wilhelmson, 2009).
Particularly within the field of geriatrics, evaluating the effectiveness of complex interventions can be quite challenging (Faes et al., 2010). Thus, as proposed by the Medical Research Council framework (Craig et al., 2008) and underlined by Looman et al. (2019), research should focus more on processes and questions concerning why and how intervention components work or do not work properly. Most likely, the design and effectiveness of future complex interventions will benefit from this. Moreover, researchers should take into account that complex geriatric interventions are sometimes not delivered or adhered to as intended (Metzelthin et al., 2013; Muntinga et al., 2015; Stijnen et al., 2014).
From a health systems perspective, it should be emphasized that despite high expectations and widespread interest in preventive, integrated care services for seniors, these services have not been conclusively proven to be (cost-)effective (Looman et al., 2019). Hence, it is still uncertain whether reablement and other types of complex interventions can reduce long-term care need and which economic implications result (Aspinal et al., 2016; Looman et al., 2019). Facing the initial rationale for integrated care, also driven by a need for cost containment, one cannot conclude that this approach necessarily leads to cost savings (Nolte & Pitchforth, 2014). Consequently, in order to extend the current limited evidence on innovative care approaches, full health economic evaluations, namely the comparative analysis of alternative courses of action in terms of both their costs and consequences, for example, cost-effectiveness or cost-utility analyses (Drummond et al., 2015), should be highly prioritized (Rocks et al., 2020). Methodological challenges, including those arising from the complex nature of the interventions themselves (Tsiachristas et al., 2016) and the paucity of high-quality studies highlight existing research gaps. Future economic evaluations should have longer time horizons to ensure that possible intervention effects can be observed and thereby generate robust evidence on long-term cost implications and cost-effectiveness (Bulamu et al., 2018). Decision analytic modeling may thus be helpful to extrapolate costs and effects beyond study follow-up (Rocks et al., 2020). Additionally, subgroup-analyses are recommended to better target interventions and resources (Faria et al., 2016). In this analysis, a full economic evaluation of the intervention was not conducted, since the intervention was not shown to be effective in terms of the primary outcome (Hasemann et al., 2022). Notwithstanding, from a health economic viewpoint, analyzing the effects of a multi-component community-based care approach on HCRU and costs by using SHI claims data is of high importance to understand direct implications for actual care delivery resulting from such interventions. In conclusion, the evaluation of complex and integrated care interventions in terms of health economic effects remains crucial to properly addressing the increasing demands of aging populations while ensuring future financial sustainability of health systems (Rocks et al., 2020).
Our findings are not without limitations. Generally, claims data are not primarily collected for research, but for billing and reimbursement purposes, and thus entail some weaknesses (Kreis et al., 2016). These include dependence on the coding behavior of health care providers. In addition, potentially relevant diagnoses of the insured are only documented if an outpatient or inpatient service was used. Due to the data source, our perspective is restricted to the payers’ perspective. Thus, we did not consider any indirect costs (e.g., productivity losses due to informal care) (Alwin et al., 2021). Further limitations refer to the model estimations. Especially analyses of hospitalization and total LOS show limitations, so that no conclusions should be drawn from it. With the selection of suitable control regions, matching, and the consideration of potential confounding variables in regression analyses, numerous methods were used to ensure the structural comparability of the study groups. Nevertheless, it should be noted that confounding factors not reflected in the data as well as a potential selection bias may have influenced the results. Accordingly, the percentage of woman in this sample (65.6%) was slightly higher in comparison to the German population of the same age (57.5%) (Federal Statistical Office, 2021) which might be due to stronger health awareness and willingness to participate within the female population (Robert Koch-Institut, 2020). Additionally, the observational period of 21 months may be too short to capture long-term changes in HCRU. Finally, it has to be considered that initial power calculation was not based on the outcomes analyzed in this study.
Conclusion
Participating in a multi-component community-based care approach for older people did not lead to a substantial shift in HCRU and costs. These findings are in line with the current state of research yielding ambiguous results of community-based geriatric interventions. More research is needed to better understand how care approaches for older people should be designed in order to improve their effectiveness and to gain more insights into the health economic implications of such interventions. This may contribute to maintain health systems’ financial affordability.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214221140222 – Supplemental material for Health economic perspective on a community-based intervention for older people at risk of care dependency – results of a prospective quasi-experimental study
Supplemental material, sj-docx-1-ggm-10.1177_23337214221140222 for Health economic perspective on a community-based intervention for older people at risk of care dependency – results of a prospective quasi-experimental study by David Lampe, Lena Hasemann, Thomas Nebling, Ulrich Thiem and Wolfgang Greiner in Gerontology and Geriatric Medicine
Footnotes
Authors’Contributions
TN, WG, and UT contributed to the study conception, design and implementation, and provided comments/revisions to the manuscript. LH and DL contributed to the conceptualization and execution of the analyses. DL drafted the manuscript. LH, TN, UT, and WG read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by innovation funds of the Federal Joint Committee (G-BA) (No. 01NVF16017).
Ethics Approval and Consent to Participate
The study protocol followed the ethical principles of the Helsinki declaration and was approved by Ethics Commission of the General Medical Council Hamburg (PV548). Written informed consent was obtained from all participants.
Study Registration
The study was registered at the German Clinical Trials Register (DRKS00027866).
Data Availability Statement
The datasets analyzed during the current study are not publicly available due to project specific agreements of data protection. On reasonable request, possibilities of data access for external researchers have to be proved. Requests can be made to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.