
Abstract
The Resident VIEW is a measure of person-centered care (PCC) from residents’ perspectives and was previously studied in nursing homes. The current study presents descriptive data for the Resident VIEW in community-based care settings including assisted living, residential care (AL/RC), and adult foster homes (AFH). Using a two-stage sampling design, we recruited 31 AL/RC and 119 AFH in Oregon and completed face-to-face structured interviews with 227 and 195 residents, respectively. Residents provided ratings for both the importance of and their experience with 66 items that tapped into PCC practices in eight domains. Results are provided for each item, many of which are significantly associated with greater quality of life, better resident satisfaction, and fewer depressive symptoms, especially in the domains of personalized care and being treated like a person. Incongruence between importance and experience ratings indicate many residents experience unmet needs across multiple domains. The Resident VIEW performed well in different types of settings, providing an important tool for researchers and providers who wish to learn about the PCC experience from residents’ points of view.
Keywords
Introduction
Consumer voices in long-term care (LTC) are increasingly at the center of research and public policy discussions, with attention directed to seeking and affirming the voices of those living in these settings. Person-centered care (PCC) practices are central to these discussions. Although specific definitions vary, PCC includes understanding and organizing support around residents’ personal goals, values, and preferences; providing personalized care in accordance with the needs and wishes of the person; and supporting resident autonomy to the greatest extent possible. With PCC now commonly viewed as the standard of high-quality care (Caspar et al., 2019) and as LTC communities seek to meet evolving standards of practice, new measures are needed to support research and evaluation of PCC (Kane et al., 2003; Van Haitsma et al., 2012; White et al., 2019; Zimmerman et al., 2015).
This study describes characteristics of one measure of PCC, the Resident VIEW (Voicing Importance, Experience, Wellbeing) in community-based care (CBC) settings in Oregon. This is a companion to a previously published article reporting on the Resident VIEW in nursing homes (NH), which included various descriptive statistics and evidence of validity for the measure (White et al., 2019). In the current study, we have two aims in presenting similar research in CBC settings. The first is to determine if the Resident VIEW can be used in different types of LTC settings and the second is to provide an item bank that researchers and others can use to further knowledge about PCC across settings and consider for use in the United States and in cross-national research (Corazzini et al., 2019).
CBC settings were developed as alternatives to NH (Kane & Kane, 2015; Wilson, 2007) and emphasize social aspects of life. These settings increasingly serve residents who have ADL and IADL needs similar to NH. Hua (2021) reports that the proportion of AL residents with high levels of care needs increased 18% between 2007 and 2017, more than double the rate of increase in acuity in NH. This was especially true for residents with dual eligibility (Hua, 2021). Although NH residents require the highest levels of care, residential care communities increasingly serve residents who are frail. Nationally, 63.6% of AL residents require assistance with bathing and nearly half (48.2%) require assistance with dressing, compared with 96.7 and 92.7% respectively in NH (Harris-Kojetin et al., 2019).
Unlike NH that are governed by federal regulations, CBC settings are regulated by each state (Carder, 2017). All states have some version of AL, although regulations and resident characteristics vary (Carder et al., 2015). For example, states differ widely in regulations governing residency agreements, disclosure provisions, admission and retention policies, staff training, infection control policies, and medication management (Bucy et al., 2020; Carder et al., 2015). About 75% of states have some provision for small residential settings, which serve five or fewer residents (Carder et al., 2015).
Study Context: CBC Settings in Oregon
Because CBC settings vary widely across the United States, we describe these settings as they operate in Oregon. We focus on two basic types, assisted living and adult foster care. In Oregon, assisted living consists of two related regulatory designations, one called assisted living (AL) and the other residential care (RC). Each of these entities have elements in common with assisted living settings as they are defined in other states. Licensing requirements for AL and RC are similar in Oregon: Both must be staffed 24 hours a day; hire or contract with a registered nurse; provide daily meals and snacks; offer social and recreational activities; and evaluate, coordinate, and monitor health services (Carder, Tunalilar et al., 2018). They differ in building requirements which stipulate that AL must provide fully self-contained units (i.e., private apartments with separate living, sleeping, kitchen, bathroom, storage space) while RC are not required to meet those requirements. The Oregon Department of Human Services (ODHS) treats AL and RC the same with respect to operation, including licensing inspections, disclosure requirements, scope of care provided, medication management, admission policies, staffing, and more (Harris-Kojetin et al., 2019). Because of their similarities and Oregon regulatory policy, we grouped AL and RC together in our analysis. Most Oregon AL and RC have contracts with Medicaid. In 2017, 42% of Oregon AL/RC residents were Medicaid beneficiaries, compared to 19% nationwide (Carder, Tunalilar et al., 2018).
In contrast, AFH are small residential settings licensed to serve between one and five residents. They differ from AL/RC in that the owner-provider or manager lives on the premises and provides much of the hands-on care. AFH are staffed 24 hours, most often by the owner-provider, to respond to residents’ scheduled and unscheduled requests (Carder, Elliott et al., 2018). Services provided include meals, housekeeping, laundry, personal care assistance, medication management, monitoring health conditions, communication with health providers, and social and recreational activities. Approximately three-quarters are licensed for five residents and most employ at least one other caregiver in addition to the owner or manager (Carder, Elliott et al., 2018).
Method
Sample and Data Collection Procedures
Community-based care sample
We used a two-stage sampling design. First, a stratified random sample of Oregon CBC facilities was generated from a list of all licensed AL/RC (n = 535) and AFH (n = 1,483) as of November 2018. All samples were stratified by region to ensure statewide geographical representation. AL/RC samples were further stratified by type (AL or RC), profit status, and quality. Type of setting was included in the stratification to address differences in population needs that have been identified in previous research (Oregon Department of Human Services [ODHS], 2019). For example, RC residents tend to have more ADL needs than AL residents, though less than AFH or NH residents. Quality is proxied by those above and below the median number of survey deficiencies. AL/RC that were specifically licensed for memory care were not included because advanced dementia was a major reason for incomplete interviews in our previous research (White et al., 2019). We determined that restricting our sample to non-memory care designated settings increased our likelihood of complete interviews while still including individuals with dementia in our resident sample. Our goal was to recruit 39 AL/RC based on our expectation of an average of seven completed resident interviews in each community. Our sample design called for recruitment of 102 AFH where we anticipated two completed resident interviews from each home (Elliott et al., 2016). We were unable to stratify the AFH sample based on quality due both to differences in reporting about quality and the lack of comparable data at the county level. All AFH are considered to be for-profit.
We used multiple methods of outreach and contact in recruitment. ODHS sent multiple provider alerts to inform AL/RC administrators and AFH providers about the study. The project manager attended professional association meetings to introduce the study, answer questions, and met with AFH union leaders to enlist their support. All administrators and providers in the sample received a letter describing the project and informing them that they had been randomly selected to participate. The project manager made up to five follow-up phone calls and email contacts. Those who indicated an intention to participate at a future date or had asked to reschedule a visit received additional contact. Interviewers called and scheduled their own visits for AFH since one interviewer generally completed all interviews in those settings. The project manager coordinated AL/RC visits to ensure adequate numbers of interviewers based on the size and location of the community. Administrators received a one-page description in plain language to distribute to residents in advance of the visit. Sites were scheduled by region to maximize resources and efficiency regarding interviewer travel to less populated areas of the state.
Figure 1 summarizes the sampling and recruitment procedures and results. Of the 535 AL/RC, 117 were randomly selected into the sampling frame, with 31 AL/RC in the final sample largely meeting the stratification goals. Over half (56%) of AL/RC that were contacted did not respond and another 16% were unable to schedule interviews. Of the 1,483 licensed AFH, 809 were randomly selected into the sampling frame resulting in 119 AFH in the final sample. Many AFH providers declined to participate (27%), others had no residents who met criteria (18%), were no longer operating (14%), or were unable to schedule when interviewers were available (13%). The remainder were not contacted either because the stratification cell was complete or the data collection phase of the study ended.

Sampling procedure.
The second level of unit selection was residents (see Figure 1). At AL/RC settings, an interview team obtained a list of residents from the administrator or designee and with them determined who met criteria for the study. Residents were excluded if they had a legal guardian, were too ill (i.e., some residents on hospice), were nonverbal or unable to communicate, were non-English speaking, had been living less than a week in the setting, or had behavioral health issues that would result in substantial disruption or distress due to the interview. The most common reasons for exclusion were having a legal guardian (32%), being nonverbal or unable to communicate (24%), or poor physical or mental health (23%). As in the NH study, residents were not screened for cognitive impairment to assure that those with cognitive impairment who were able to complete the interview would have their voices heard (White et al., 2019). Face-to-face interviews were conducted during 2019 using a structured questionnaire (see supplemental materials, ResVIEW tool—CBC—v4 revised 4-19-19).
In AL/RC, all eligible residents were randomly divided between team members who then approached residents in the order listed. Upon meeting residents, interviewers introduced themselves and described the study. Interviewers were trained to gauge residents’ interest and ability to participate. If appropriate, they proceeded with the informed consent and began the interview. If, at any time during the interview, the interviewer observed that the resident was not able to track the questions or participate in a meaningful way, or if a resident indicated they were tired or wished to stop, the interviewer would conclude, thank the resident for their time, and leave. Interviewers were not able to meet all eligible residents. On the initial visit, well over half of AL/RC residents were not in their rooms. Another 10% were engaged in receiving care, sleeping or having visitors. When possible, a second visit was made if an interviewer had not been able to meet several eligible residents on the first visit. This occurred when we had team members available for a second visit and the additional visit could be arranged with the administrator. Overall, about one-quarter of AL/RC residents we contacted refused to participate, including a few who started the interview and asked to stop (about 3%). Interviewers initiated and then stopped interviews with 10% and 15% of residents in AL and RC respectively due to cognitive impairment demonstrated by lack of ability to track questions or respond to the questions.
In AFH settings, providers identified the number of residents who did and did not meet study criteria for participation. Visits were made only if the provider reported that at least one resident met inclusion criteria. Interviewers attempted to interview all eligible residents in the order assigned. As in AL/RC, interviewers introduced themselves to AFH residents, explained the study, and when residents agreed, initiated the informed consent process followed by the interview. Nearly 40% of AFH residents refused to participate. Interviews initiated with over one-third of the residents were not completed due to cognitive impairment. Unlike AL/RC residents, most AFH residents were present on the site, though about 10% were either sleeping, receiving care, or with visitors.
At the end of interviews with residents in both AL/RC and AFH, a team member obtained resident information from the administrator or provider for those who had consented and participated in the study. This included move-in date, payment source, and date of birth. At each site, the team maintained a record of the number of residents on the census, number and reasons for exclusions, and the numbers of complete and incomplete interviews. Interviewers made detailed notes about each interview including their confidence in the data collected (see supplemental materials for interview rating form at the end of the ResVIEW tool). Twenty-five cases were removed from the AFH data set and 14 from the AL/RC data set before analysis, mostly because of incomplete interviews.
Measures
The Resident VIEW is a 66-item measure of PCC from the perspectives of residents and addresses eight domains reflecting the breadth of PCC (White et al., 2019). Six domains represent direct support to residents (meaningful activity, personalized care, knowing the person, autonomy and choice, treated like a person, relationships with staff) and two are related to the overall environment (physical environment, organizational environment). By definition, the PCC construct recognizes that what matters to residents varies by individual. Measurement of PCC practices, therefore, requires knowledge of both what is important to residents and how it matches their experiences of care. Accordingly, the Resident VIEW includes questions both about the importance of a particular item as well as residents’ experience with that item. Specific items that make up the Resident VIEW were developed through extensive literature review as well as cognitive interviews with those living in NH, AFH, and AL/RC in Oregon (White et al., 2016). Response categories for importance ratings were “not at all,” “somewhat,” and “very important.” Similarly, response categories for the experience ratings were “no,” “somewhat,” and “yes.” In addition to recording these responses, interviewers also noted comments residents made about specific items.
The Resident VIEW tested in NH originally contained 63 (White et al., 2019). Based on comments and interviewer observations in the NH study, 3 items were added for the CBC study. In the meaningful activity domain, we added an item about feeling useful. Second, we asked about choosing what to eat as part of the autonomy and choice domain. Before, we had asked only about choosing when to eat. Third, we asked residents about having a say in who helps them, a new item in the organizational environment domain. All items from the Resident VIEW NH study were retained.
The focus on multiple domains of PCC as well as asking about both importance and experience make the Resident VIEW unique among PCC tools, which may focus entirely or primarily on importance or experience. The Resident VIEW allows measuring the incongruence between how important each resident rates an item and whether their reported experience in that item aligns with their importance rating, a measure we call “unmet need.” Residents were assigned a value of 1 if they responded “very important” for the importance of an item but “no” or “some” for the corresponding experience with an item. Similarly, residents who responded “somewhat important” for the importance of an item and responded with a “no” response for their experience with that item were also assigned 1. All other residents received a value of 0 for this unmet need indicator, indicating that there was some correspondence between how much they valued an item and their experience with it. Supplemental Table 1 shows a matrix describing this variable. Unique aspects of the Resident VIEW are described in more detail by White et al. (2019).
As in the NH study, additional measures were included to gather evidence of validity for the Resident VIEW. PCC is thought to be associated with greater quality of life, which includes mood. Therefore, to assess criterion-related validity, we included the Quality of Life for Alzheimer’s Disease (QOL-AD; Logsdon et al., 2002) and the Patient Health Questionnaire (PHQ-9; Saliba et al., 2012). The QOL-AD was selected to accommodate participants with cognitive decline. PHQ-9 was selected as a measure of depressive symptoms. We expected that residents receiving PCC would have greater satisfaction with the setting. Four satisfaction items were included based on the work of Kane et al. (2007). The Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005) was used both to describe the sample and to determine at what level of cognitive functioning residents could successfully complete the Resident VIEW. The Katz Index of Independence in Activities of Daily Living (Hartigen, 2007) was included for descriptive purposes.
Analysis
To describe characteristics of residents in the final sample and the communities in which they lived, separately for AL/RC and AFH samples, we used means and percentages. We also compared means and percentages across the two settings for resident characteristics, indicators of resident well-being, and quality indicators. Finally, to examine the generalizability of the community sample, we compared the community characteristics of our sample with the known characteristics of AL/RC settings in Oregon in terms of average age, gender, non-Hispanic White, and Medicaid status.
We next calculated the percentage of distribution of responses to items that make up the Resident VIEW tool separately by domain and setting. This analysis allowed us to show resident preferences (i.e., importance) and experiences in each domain and in each setting. We next examined the congruence between what residents reported as important and what they experience using our indicator of unmet need (as described above) and the ρ statistic. The ρ statistic refers to Person’s correlation coefficient between responses to importance and experience questions for each item. We also calculated Cronbach’s α for each domain to measure within-domain agreement among items. Finally, to gather evidence of criterion-related validity for each item, we examined the mean differences in quality of life, depressive symptoms, and general satisfaction between those responded positively (“yes”) for that item and those who did not (“some” or “no”). Mean difference tests were based on ordinary least squares (OLS) linear regression results including an indicator for positive experience (0 = no or some; 1 = yes) and incorporating design weights.
Results
Table 1 shows community and resident characteristics in the analytic sample by setting. The CBC communities in the Resident VIEW sample were similar to a representative sample of Oregon AL/RC communities licensed in Oregon in terms of rurality, Medicaid contract, and non-profit status, though the Resident VIEW sample had slightly more licensed beds than the larger sample, with 60 and 51 beds respectively (White et al., 2021). The AFH sample was also similar to the larger population of AFH in Oregon, although more of the Resident VIEW sample came from the Portland Metropolitan area than from rural areas in central and southern Oregon (Carder, Elliott et al., 2018). With respect to the resident sample, the Resident VIEW AL/RC sample was more likely to be non-Hispanic White (97% compared to 90%), but was similar in terms of age, gender, and Medicaid status. In contrast, the Resident VIEW AFH sample was less likely to be female (57% compared to 62%), more likely to be receive Medicaid (69% compared to 57%), and be younger (mean age 71.7 years vs. 76.5 years) (Carder, Elliott et al., 2018; White et al., 2021).
Community and Resident Characteristics by Analytic Sample by Setting.
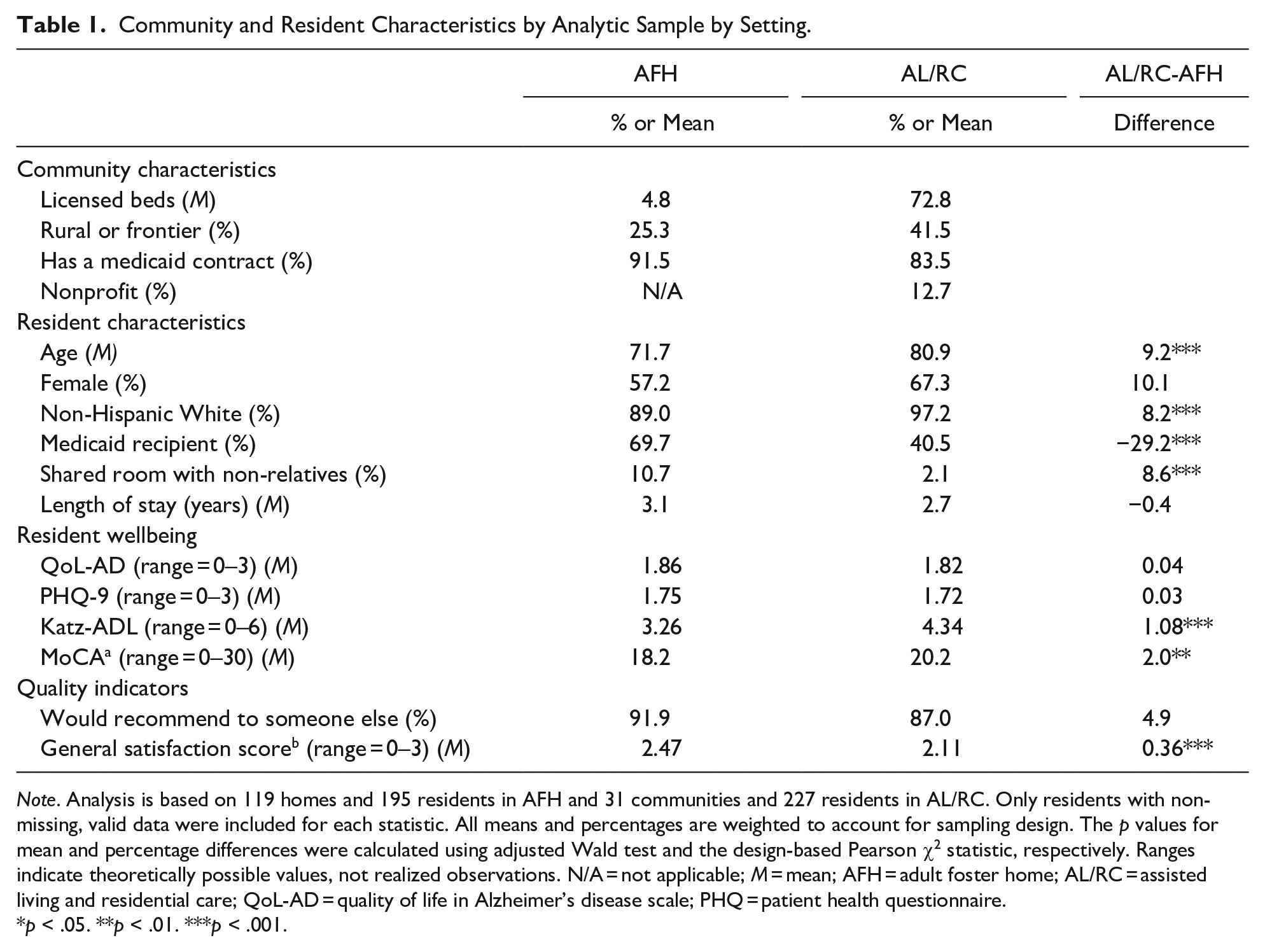
Note. Analysis is based on 119 homes and 195 residents in AFH and 31 communities and 227 residents in AL/RC. Only residents with non-missing, valid data were included for each statistic. All means and percentages are weighted to account for sampling design. The p values for mean and percentage differences were calculated using adjusted Wald test and the design-based Pearson χ2 statistic, respectively. Ranges indicate theoretically possible values, not realized observations. N/A = not applicable; M = mean; AFH = adult foster home; AL/RC = assisted living and residential care; QoL-AD = quality of life in Alzheimer’s disease scale; PHQ = patient health questionnaire.
p < .05. **p < .01. ***p < .001.
We turn now to the cognitive and functional status of the Resident VIEW sample. Although AFH residents had lower MoCA scores (18.2) compared to their AL/RC counterparts (20.2), the mean scores in both groups were well below the cutoff of 26, which indicates that the Resident VIEW sample included a large proportion of people with mild and moderate levels of dementia (Julayanont & Nasreddine, 2017). AFH residents also had more dependency in ADLs compared to AL/RC residents, with Katz scores of 3.26 and 4.34 respectively. Residents across the two settings were similar in terms of self-reported well-being as measured by QoL-AD and PHQ-9 (Table 1).
Tables 2 and 3 provide the distribution of importance and experience ratings of AFH and AL/RC residents respectively for all 66 items by domain as well as Cronbach’s α coefficients for each domain. In AFH, Cronbach’s α coefficients were relatively high for six of the eight domains which focused on services and support. An exception was for the experience with autonomy/choice domain, which was .71, but is still within acceptable parameters for research purposes (Nunnally & Bernstein, 1994). Cronbach’s α coefficients for AL/RC residents were somewhat lower for these six domains, ranging from .68 for the experience with autonomy/choice domain to .84 for importance of the relationship domain. Lower α coefficients in AL/RC may reflect greater heterogeneity among residents in these settings with respect to functional status and engagement in the community. The two environmental scales had lower overall reliability coefficients with a low of .54 for importance of the physical environment domain for AL/RC residents to a high of .77 for the importance of the organizational domain for AFH residents, suggesting that the items in these domains work less well together, though somewhat better in AFH settings.
Distribution of Adult Foster Home Resident View Items.
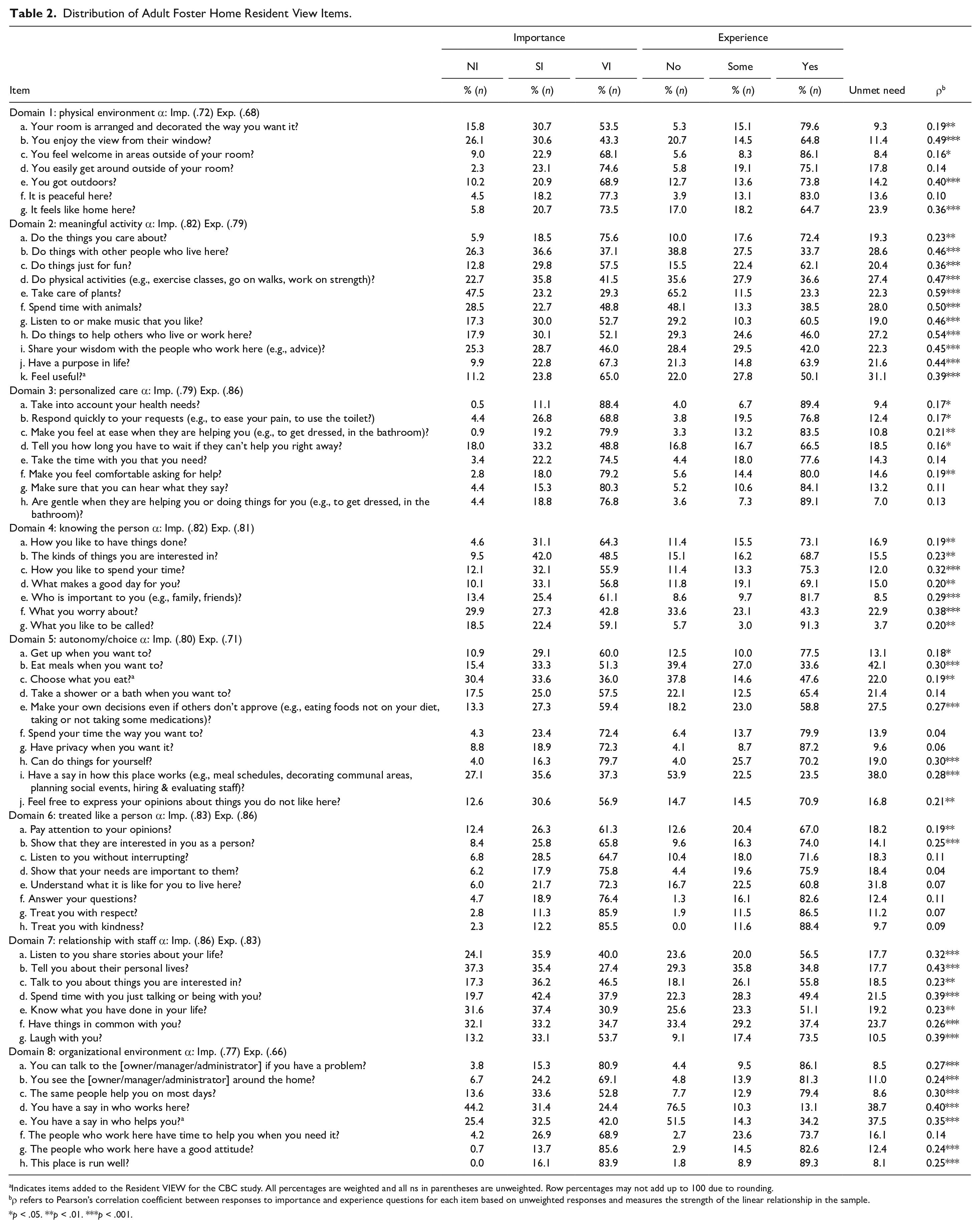
Indicates items added to the Resident VIEW for the CBC study. All percentages are weighted and all ns in parentheses are unweighted. Row percentages may not add up to 100 due to rounding.
ρ refers to Pearson’s correlation coefficient between responses to importance and experience questions for each item based on unweighted responses and measures the strength of the linear relationship in the sample.
p < .05. **p < .01. ***p < .001.
Distribution of Assisted Living/Residential Care Resident View Items.

Indicates items added to the Resident VIEW for the CBC study. All percentages are weighted and all ns in parentheses are unweighted. Row percentages may not add up to 100 due to rounding.
ρ refers to Pearson’s correlation coefficient between responses to importance and experience questions for each item based on unweighted responses and measures the strength of the linear relationship in the sample.
p < .05. **p < .01. ***p < .001.
Ratings of importance varied across and within domains. Using the cut-off point of 75%, we found that AFH and AL/RC residents rated 15 items and 20 items as very important (VI), respectively. In both settings, personalized care domain items followed by treated like a person items were most likely to have VI ratings, although other domains also were represented in these most important items (five domains in AFH; six in AL/RC). The five top-rated items for importance were the same in both settings and covered three domains: “taking into account your health needs” (personalized care), “treating you with respect” (treated like a person), “staff having the right attitude” (organizational environment), “being treated with kindness” (treated like a person), and “the place being run well” (organizational environment). We also observed congruence in these settings between ratings of VI and experience. In AFH, 80.2% to 89.4% of residents reported they experienced the top five rated VI items, with even greater percentages of AL/RC residents experiencing top-rated items (range 86.5– 92.7%).
Fewer residents ranked items as not important (NI), although at least 25% AFH and AL/RC residents rated 13 and 9 items this way, respectively. Four of the top five items rated as NI included “going outdoors when you want to” (meaningful activity), “having a say in how the place works” (organizational environment), “staff telling you about their personal lives” (relationships), and “staff knowing what you have done in your life” (knowing the person). In their five top-rated NI items, AFH residents also rated “staff having things in common with you” (relationships), while AL/RC residents gave this rating to the setting being peaceful (physical environment). In AFH, the items most frequently rated NI included 4 meaningful activity items, 3 relationship items, 2 items each from organizational and autonomy/choice domains, and 1 item each from the physical environment and knowing the person domains. Items most frequently rated as NI by AL/RC residents came from four domains: relationships (3 items), meaningful activities (3 items), organizational environment (2 items), and 1 item in the knowing the person domain.
The correlation coefficients (ρ) between experience and importance ratings for many items were strong, indicating there is substantial overlap between what most residents rate as important and what they report receiving. For example, for both AFH and AL/RC residents, correlations were high for several meaningful activity items such as taking care of plants, doing physical activity, spending time with animals, listening to or making music, and spending time with other residents. Other items with strong correlations included enjoying the view from their windows (physical environment) and having staff who knew the resident’s worries (knowing the person). Note that VI ratings were assigned by less than half of the residents for most of these items.
We examined incongruence between what individual residents rated as important and what they reported experiencing. We found that 25% or more of AFH residents experienced unmet needs for 11 items, including choosing what they ate, having a say in who worked at the AFH, having a say in how the AFH worked, and having a say in who helped them. AL/RC residents experienced even greater unmet needs, with 26 items meeting the threshold of 25% or more of residents having unmet need in areas that were important to them. The prevalence of unmet need for these items ranged from 27.2% (“help others”) to 42.1% (“choose when you eat”) for AFH residents, and from 25.1% (“people have time to help you when you need it”) to 58.2% (“have a say in how this place works”) for AL/RC residents. Two of the new items added to the CBC survey were among those with the greatest unmet need for both AFH and AL/RC residents: feeling useful and being able to choose who provided help to them. Choosing what to eat was an area of unmet need for 31.1% of AL/RC residents and for more than one in five AFH residents, although it did not meet our cut-off thresholds for the AFH sample. Other items with the high levels of unmet need included having a say in how the place worked, staff understanding what it was like for the resident to live there, having a say in who worked there, and staff telling residents how long they have to wait if staff can’t help residents right away.
Although correlations between ratings of importance and experience were substantial, many residents had unmet need, often in areas that had been rated NI for the majority of residents. For example, residents in both samples reported substantial unmet need for helping others who lived or worked in the setting, yet only about half of residents rated this as very important.
To examine criterion-related validity separately for each item, we turn now to Table 4, which shows the mean differences in depressive symptoms (PHQ-9), quality of life (QoL-AD), and general satisfaction, comparing those reported receiving an item (“Yes”) and their resident counterparts (“some” or “no”). Among AFH residents, there were statistically significant (p < .05) mean differences between the two groups for most items in terms of quality of life (57 out of 66 items), depressive symptoms (34 out of 66 items), and general satisfaction (63 out of 66 items). Similarly, among AL/RC residents, there were statistically significant (p < .05) mean differences between the two groups for most items in terms of quality of life (58 out of 66 items), depressive symptoms (39 out of 66 items), and general satisfaction (52 out of 66 items).
Differences in Averages of Measures of Quality of Life (QoL-AD), Depressive Symptoms (PHQ-9), and General Satisfaction by Reported Experience.

Note. All means are weighted. N-S = no (not at all) or some receipt. Difference tests are based on ordinary least squares (OLS) linear regression results incorporating design weights.
These items were added to the original Resident VIEW measure.
p < .05. **p < .01. ***p < .001.
Discussion
Overall, the evidence of validity presented here for the Resident VIEW in AL/RC and AFH settings is promising. We have demonstrated that multiple items of the Resident VIEW work well across different types of LTC: in NH, AL/RC, and AFH. We would expect some variation in responses when residents live in different types of settings. For example, residents in different settings may have different priorities and preferences for care and have different needs and expectations for support. We did find variation in specific responses. At the same time, however, we found expected patterns of association, as measured by mean differences, between responses to Resident VIEW items and multiple outcome measures, which is evidence of criterion-related validity. These findings indicate that the Resident VIEW can be used meaningfully across different types of LTC settings, especially when those settings are clearly defined.
As with the NH study (White et al., 2019), these results show that PCC practices of greatest importance to CBC residents have to do with personalized care and being treated like a person. As care needs and acuity increase, PCC practices exemplified in these domains likely become increasingly important to residents’ quality of life. In all settings, residents who experienced the PCC practices reflected in these domains, reported positive, and significant associations with important resident outcomes: higher quality of life, fewer depressive symptoms, and greater satisfaction with the settings. Although many of the items contained within other domains were not significantly associated with lower levels of depressive symptoms, many items were positively and significantly associated with higher quality of life and greater satisfaction. This finding suggests that multiple domains of PCC are important for resident well-being, supporting the value of defining PCC broadly.
PCC practices rated as the least important by most residents are of great interest. Across three settings (including the NH study), items comprising the relationships with staff domain generally had higher ratings of not important (NI) than in other domains. Although some residents express personal preferences to keep their lives private and not engage with staff, other residents appear to adjust their ratings of importance based on their perceptions of what is possible (White et al., 2021). For example, some commented that staff do not have time to listen to their stories and that it is unreasonable for residents to expect them to do so. Consistent with cognitive dissonance, residents may decide that such conversations are not important to them. In the AL/RC samples, ratings of NI were higher for the knowing the person domain relative to both AFH and NH residents. This likely reflects the differences in reliance on staff for daily support found in these settings. In spite of relatively low ratings of importance and experiences in these domains, however, when residents who experience relationships with staff and feel that they are known, they have higher quality of life and greater satisfaction with the setting than those without these experiences. Further research is needed to understand items in these domains in relation to PCC principles and the context of care. In addition to ratings of importance, we observed other differences in resident responses between the CBC settings that warrant further exploration. Overall, AFH residents had more positive relationships with staff, fewer unmet needs, higher levels of satisfaction with their setting, more positive relationships with staff, and higher levels of quality of life. AL/RC residents were more likely to report unmet need, particularly with items in the organizational environment domain and knowing the person domains. Additional research is needed to determine the sources of these differences in perspectives about PCC. Some of these differences may be related to setting size and resident needs for support. Because AFH settings have five or fewer residents, a very small staff, and residents with greater ADL needs, AFH residents and staff spend a lot of time together and seem to know each other well. In contrast, AL/RC residents mostly live in private apartments in a setting with many more residents and staff who do traditional shift work. If AL/RC residents have few ADL and IADL needs, they may feel somewhat isolated from administration and staff and perhaps other residents. Differences also may be associated with self-selection by residents into various types of settings. They also may be a result of our sampling process, where many eligible residents were not on site for interviews in AL/RC and we experienced greater refusal rates in AFH, potentially biasing both samples.
Asking residents about both the importance of items and their experience in receiving support related to those items, allowed us to assess areas of unmet need based on individual preferences. Capturing unmet needs is especially important for adhering to PCC principles since it recognizes that residents have a wide range of individual needs and preferences. Our findings reinforce the call to personalize support in response to these differences. Areas of highest unmet need were frequently for items that had only moderate ratings of importance, such as having a say in who helped residents or feeling useful (both settings), or spending time with animals (AFH), and choosing what to eat and having the place feel like home (AL/RC). From an organizational perspective, it might be unreasonable to expect residents to have a say in who works in the setting, especially in these days of staff shortages. Indeed, many residents’ comments acknowledged staffing issues. Others expressed no desire to be involved in such organizational decisions. Yet unmet need was high for those residents who found this level of involvement to be important. The culture change movement has long advocated for residents to have a greater voice in shaping their environment. In person-centered settings, this may mean honoring resident preferences for who helps them and making resident councils more effective and responsive to residents in shaping their environment.
This study has several limitations. First, the cross-sectional design does not allow us to capture residents’ views over time or determine causation. Future research with the Resident VIEW should include a longitudinal design that tracks preferences from the time residents move into the setting and over time. Second, this study is limited to Oregon. The Resident VIEW should be tested in other states with different regulatory rules. At the same time, AL/RC and AFH in Oregon are very different types of CBC settings. Results suggest that this measure may be useful beyond Oregon in exploring PCC in different models of care.
Third, our samples may not be as representative as we had hoped. As noted, our response rates were relatively low. In AL/RC, we were not able to contact most residents who were eligible for interviews because they were not on site or were engaged in other activities. Those we did interview may have been different than those we did not. Refusal rates were higher in AFH, which may also have resulted in a nonrepresentative sample. Our sample may have been cognitively and physically healthier than the general CBC population. As anticipated by design, several interviews could not be conducted due to cognitive impairment. At the same, however our final sample included many residents with cognitive impairment and physical frailties who could and did complete the interview successfully. Residents in our sample may have preferences for one type of setting over another. Alternatively, choices of settings may be limited in some regions of the state, especially in rural and frontier counties where a community may have only one type of CBC setting available to them. Furthermore, without knowledge about quality in AFH settings, we do not know whether the AFH providers who agreed to participate provided a different quality of care than those who did not. It may be that the greater satisfaction expressed by residents in these settings reflect this bias. Finally, data collection for this study concluded just before the COVID-19 pandemic. Resident care preferences may have been altered by pandemic experiences. This is an open question for future studies.
This study has important strengths. We were able to complete extensive interviews with 422 residents living in 119 AFH and 31 AL/RC. Although the resident sample was not fully randomized, the order of recruiting residents on site was randomly assigned. Our attempt to interview all eligible residents whenever possible across multiple settings resulted in a resident sample that is largely generalizable to the population of AL/RC and AFH residents in Oregon. We examined elements of PCC from the perspective of residents that included both their ratings of importance and experience. Coupled with our NH study with 258 residents in 32 settings (White et al., 2019), these studies are among the largest cross-setting data sets examining residents’ preferences and experiences in residential long-term care.
This study also contributes to the goal of providing a bank of items that researchers and others can use to further knowledge about PCC practices across settings and to consider in cross-national research. Such research will contribute further information about the utility of items in research. We note that use of these items separately will not constitute use of the Resident VIEW, though researchers are welcome to incorporate the full measure in their research.
Validation of any measure is a long-term process requiring additional research by multiple research teams (Pedhazur & Schmelkin, 1991, citing Borhnstedt & Borgatta, 1981). Questions emerging from this study suggest areas for additional research. The next step for our team will be further refinement of the measure by closer examination of items within the context of each domain with the goal of producing a short-form of the Resident VIEW. As suggested by response rates, use of the full measure was burdensome to some residents. To create a short form we will conduct further analysis using appropriate tests to identify those items that best represent the PCC domains, address issues of unmet need, and are associated with outcome measures. Further research will be necessary to finalize and test the short form.
Additionally, the Resident VIEW should be examined over time, not just to examine stability of importance ratings, but also to examine changes in experience and unmet need. Such research would help identify areas of unmet need over time and identify organizational or personal factors associated with it. Longitudinal data might help answer the question of whether and when some people might lower ratings of importance to align with their experiences as we suggested might have occurred for low importance ratings for “knowing the person” and “relationships with staff.”
The Resident VIEW can be used to compare different types of settings to determine the extent to which contextual factors (e.g., size, staff resources, geographic location, setting type, leadership skills) predict residents’ perspectives of PCC. In addition to examining the Resident VIEW as a predictor of outcomes related to psychological well-being, additional research could examine the association of the Resident VIEW with health outcomes such as functional status and morbidity.
Finally, the Resident VIEW could be tested in assisted living settings that focus specifically on serving older adults living with dementia. Although residents with significant cognitive impairment successfully participated in our study, we do not know if the Resident VIEW, even a shortened form, could be used extensively in settings specifically designed for those with dementia.
Conclusion
We presented initial analysis of data collected to validate the Resident VIEW in CBC residential settings. Findings from this study, coupled with our prior NH study, indicate that most items of the Resident VIEW have salience for residents across these types of settings. Findings also support inclusion of eight domains, emphasizing the multidimensional aspect of PCC. In addition, we found that the Resident VIEW can be used successfully with many residents who have mild to moderate levels of cognitive impairment. Evidence suggests that the three new items are useful additions to the Resident VIEW. These findings should inform researchers and providers who wish to learn about the PCC experience from residents’ point of view.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214221139367 – Supplemental material for The Resident VIEW in Community-Based Care Residential Settings
Supplemental material, sj-docx-1-ggm-10.1177_23337214221139367 for The Resident VIEW in Community-Based Care Residential Settings by Diana L. White, Ozcan Tunalilar, Serena Hasworth and Jaclyn Winfree in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-2-ggm-10.1177_23337214221139367 – Supplemental material for The Resident VIEW in Community-Based Care Residential Settings
Supplemental material, sj-docx-2-ggm-10.1177_23337214221139367 for The Resident VIEW in Community-Based Care Residential Settings by Diana L. White, Ozcan Tunalilar, Serena Hasworth and Jaclyn Winfree in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We thank our team of interviewers for their contribution to the completion of the validation study. We also thank the assisted living, residential care, and adult foster homes who welcomed and accommodated this research effort. We especially express our gratitude to the residents who participated in our study. We learn from them and they continue to inspire and motivate us to do this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support to conduct the research was provided by the Quality Care Fund through the Oregon Department of Human Services (IAA #158501). Support for analysis and presentation of these findings was made possible by a grant from The Patrick and Catherine Weldon Donaghue Medical Research Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.