
Abstract
Community building is necessary to help create a dementia-inclusive society. In this study, a one-of-a kind dementia education program based on mutual learning using instructional design was developed alongside community members and stakeholders. The purpose was to implement and evaluate this program and gain insight into dementia education for the community. A total of 118 individuals participated in the program; however, data of 80 participants (Male = 26, Female = 54), who completed a questionnaire before and after the program, were analyzed. The results showed a significant pre–post difference in mean total scores on the Attitudes Toward Dementia Scale (32.1 points pre-program vs. 33.7 points post-program). Nine necessary learning topics were identified. The program could successfully teach participants to take the perspectives of various other people, view dementia as something relevant to themselves, and think about specific ways of responding to people with dementia considering their feelings. This study recommends creating education programs using scenario stories that depict the desire of people with dementia to be a part of the community, using visual depictions to create a shared impression and facilitate mutual learning.
Introduction
Dementia is a global issue, with the number of people with dementia (PwD) projected to reach 82 million by 2030 and 152 million by 2050 (World Health Organization [WHO], 2021). In Japan, by 2025, roughly one in five people older than 65 years will have dementia (Ministry of Health Labour and Welfare [MHLW], 2017a). Therefore, under the New Orange Plan, the Japanese government is undertaking initiatives to create communities where people can continue living in a familiar environment even after developing dementia. The basis for these initiatives is an emphasis on the perspectives of PwD and their families (MHLW, 2017a).
In Japan, a survey on the actual image of dementia among people aged 18 years or older showed the following: people believed that those with dementia would burden their family members (73.5%), caused trouble to people around them (61.9%), forgot family and important memories (57.6%), and became unable to do things (56.4%); therefore, more than half of the people questioned had a negative perception of PwD (Cabinet Office, 2019). Dementia policy in Japan seeks to achieve an inclusive society in which community members and local organizations move beyond the relationship of “helper” and “helpee” to participate as personally affected individuals. People are connected with each other and resources seamlessly, leading to the creation of a lifestyle, reason for living, and community for each resident. Such a society would allow community members to continue living with hope even after developing dementia (MHLW, 2017b). On a global scale, the WHO (2021) has proposed the promotion of a dementia-inclusive society. An inclusive, dementia-friendly community is a similar concept, defined as a place where PwD are understood, respected, supported, and comfortable (Wu et al., 2019).
To build spaces for PwD, two-way relationships—wherein both sides “take care of” and “are taken care of”—and working on inclusive environmental design (Hung et al., 2021) are essential. Therefore, concerns have been raised about the aging of the directors and members of such groups (Gender Equality Bureau Cabinet Office, 2016; National Association of Chairpersons of City Councils, 2021). Hopefully, such efforts toward a dementia-inclusive society will be cultivated in these community-based organizations and groups, as well, even as population aging advances and challenges with dementia emerge.
Community-based dementia education programs are necessary. In Japan, Ninchisho supporter training sessions are held nationwide. These include a specialized 90-minute seminar for the public held at schools and offices and for community groups across the country. During the seminar, attendees learn about dementia, how it affects the lives of PwD, and what they should know to effectively support PwD (Alzheimer’s Disease International, 2017). As of March 2022, these sessions had trained approximately 13.8 million Ninchisho supporters (Community-based Co-Operation Policy-Alliance of Local Governments, 2022) working in accordance with the unique features and needs of diverse local communities (Community-Care Policy Network, 2020). However, some dementia supporters are unsure of how to help (Miyano et al., 2018; Uchida et al., 2017). Thus, there is a need for education programs that support this desire to help among willing individuals and empower them for community action (Arakawa et al., 2016). Internationally, public education to reduce stigma and increase awareness is a key strategy in the formation of dementia-friendly communities (Hung et al., 2021). Continuing the development of dementia-friendly communities requires education that also brings in stakeholders (Heward et al., 2017).
Several public dementia education programs that incorporate first-person experience and consideration of the feelings of PwD are currently in use. These include programs that encourage participation in community welfare initiatives and increase social activity to prevent dementia (Imaoka et al., 2019); programs for community members, which promote understanding of dementia and consideration of the feelings of PwD (Maruo & Kono, 2012); and programs enabling one to personally experience the perspective of someone with dementia through virtual reality (Sari et al., 2020; Silver Wood Co., Ltd, 2020). However, there are limited examples of educational materials that confront the challenges of dementia in the context of community activities, that is, residents’ groups or residents’ organization initiatives. Therefore, there is a need for systematic and theory-based development of educational materials and an education program emphasizing mutual learning based on adult learning theory.
Further, studies have verified the effects of dementia education programs using pre–post increases in knowledge (Imaoka et al., 2019; Matsuda et al., 2017) or changes in attitude toward dementia (Kim et al., 2011; Sari et al., 2020). Nevertheless, few have evaluated the impact of education programs qualitatively using participant learning. Therefore, this study developed a dementia education program based on mutual learning using instructional design alongside community members and stakeholders. The purpose was to evaluate this program and gain insight into dementia education for the community members to foster a dementia-inclusive society.
Methods
Developing Educational Materials Through Co-design
When developing these educational materials, the aim was to appropriately abide by the needs of the education program providers and end users—community members. Therefore, a diverse research group including administrative officers involved in policy on dementia education in universities and for the public; professionals who frequently support PwD; and community members participating in activities involving PwD or their families was constructed. Further, research team conferences were conducted according to the educational material development process and worked together while sharing opinions.
Table 1 shows details regarding the educational materials, developed based on instructional design—a system of procedures for developing education and training curricula following consistent and reliable methods (Reiser & Dempsey, 2012). The instructional design process comprises five stages: analysis, design, development, implementation, and evaluation.
Educational Materials Development Process Based on Instructional Design and Co-design.

Analysis
The researchers first asked research team members—one community social worker, four lifestyle support service coordinators, and two community leaders who participate in community activities—to complete a questionnaire. It comprised scenarios in which residents experience difficulties in interacting with PwD during community activities. Subsequently, at a research team conference, challenges in interacting with PwD common to those scenarios were identified under the supervision of other researchers who specialized in dementia care and had experience with producing video learning materials. These challenges were consistent with those faced by the families of PwD, as identified in a survey (Ishimaru et al., 2019). The research members confirmed the scenarios’ validity using their expertise and through discussion, considering the perspective of PwD. Next, the members engaged in discussion to define topics for mutual learning of how to respond to dementia when challenges were identified. Consequently, nine necessary learning topics were identified. These focused on a person with early stage dementia as the “main character.” The central themes comprised this person’s thoughts and feelings in their interactions during community activities and their family’s experience of “coming out” to the community (Nagata et al., 2019).
Next, the necessary media and tools were determined. Video materials at the recommendation of a researcher with experience in this medium were produced. Video was considered a more appropriate medium than text for helping participants easily imagine the community activities of PwD and faithfully reproducing the changes in residents’ situations in the context of community life.
Design
The learning and concrete goals, and the learning content and structure were clarified, and the research protocol was created (Table 2). The learning goals were as follows: (1) contemplate how to respond to PwD and their families as a personally relevant matter (e.g., what would I think if it were me?) and (2) think about how to respond to PwD and their families as a personally relevant matter to consider everyday community interactions and activities. Five concrete goals were also established. Subsequently, an 80-minute education program in which participants watched video scenarios and completed three worksheets to organize their views was drafted. Further, they completed mutual learning group work (four–six people) based on adult learning theory.
Program Plan.

Development (production)
A video based on the scenario outlines of the defined learning topics was produced and the production was outsourced to a video production company. The first half comprised three scenarios. In Scenario 1, Mr. Chiba—an older man participating in a community activity—experiences short-term memory loss, leading to trouble with someone attending the activity. Mr. Chiba experiences frustration, and the other attending community members are bewildered. In Scenario 2, the community leader bumps into Mr. Chiba’s wife at the local pharmacy and apologizes. Mrs. Chiba confides that she, too, has been previously perplexed by her husband’s dementia symptoms. Subsequently, in Scenario 3, the community leader seeks advice about how to interact with Mr. Chiba from a staff member at the integrated community support center who asks those involved to consider what Mr. Chiba is thinking and feeling. This prompts the viewers to ponder the importance of understanding the thoughts and feelings of PwD. The video subsequently shows Mr. Chiba and his wife seeking advice at the integrated community support center and smiling during a pleasant chat at a community activity, showing those watching that Mr. Chiba continued to participate in community activities. The video reflects the opinions of the community residents and dementia professionals at the research team conference. They stated that the video should cover a common dementia-related problem in the community and evoke a positive image of living hopefully even after developing dementia. The video’s second half comprised commentary from the researchers and dementia professionals on the research team and was intended to be a learning summary after the participants had completed the coursework.
The video—filmed at the meeting hall used for community activities—was produced to recreate an everyday situation. The residents and dementia professionals from the research team served as actors.
Further, tools to expand the education program (PowerPoint and procedural manuals, worksheets, evaluation sheets) were developed. Worksheets to help participants organize their thoughts after watching the video were created (Table 2). The aim was for participants’ thinking to gradually grow deeper by watching the video scenarios and completing a worksheet each time.
Implementation
The education program with community members using the created products was implemented. Three local organizations participated (two neighborhood associations [A & B] and one community group [C]), who engaged in community building at the suggestion of members of the research team conference. Programs were held at a meeting hall or other community buildings. There were 48, 50, and 20 participating community members, respectively, for organizations A, B, and C (N = 118). Neighborhood association A’s participants included two staff members of an integrated community support center. As a general rule, only one person was in charge of the program designed to be led by one person. Upon implementing the program for the first time with neighborhood association A, seven research team members participated, offered support, and observed how the group work proceeded but did not actively intervene.
Evaluation
Administrative officers, professionals, and community members of the research team evaluated the program’s validity and practicality (Table 3) for mutual learning of how to respond to PwD during community activities. All seven evaluating team members found the educational materials valid and practical.
Evaluation of Developed Educational Materials by Research Team Members (Administrative Officers, Professionals, and Community Members; n = 7).

Note : There were 0 responses of “not really” and “no” for Questions 1 and 2.
Evaluating the Program Using Developed Educational Materials
Participants
Three local organizations in the suburbs of metropolitan Japan—A, B, and C (N = 118 Japanese participants who were both members and users of the target organizations)—participated. The sample comprised individuals who participated in the education program and consented to their data’s use in a study of the educational materials.
Data collection
Questionnaire survey (Quantitative and qualitative)
To evaluate pre–post changes in attitude toward dementia, a questionnaire using the concrete goals of the program and the Attitudes Toward Dementia Scale (ATDS; Kuroda et al., 2011) was created. This instrument was chosen because research has shown that people who acted (e.g., by volunteering) after attending a Ninchisho supporter training session had a high level of dementia acceptance even before attending the training. Thus, the scale was deemed a valid outcome evaluation. Moreover, the first item of the ATDS is nearly identical in meaning to Concrete Goal 3 (“consider a person with dementia with respect to their wishes”).
Accordingly, the survey included sex, age, the eight ATDS items, and two items about attitude toward dementia that were related to two concrete goals (Q5: “Use various assistance services when dementia causes problems” and Q2: “Devise concrete plans to find a role in community activities for people showing signs of dementia to allow them to continue participating”). Responses were selected from a five-point Likert scale as follows: 1, agree; 2, somewhat agree; 3, neither agree nor disagree; 4, somewhat disagree; and 5, disagree. Each item was assigned a score from 1 to 5. The first four items of the ATDS and the two newly added items had inverted response scores, with higher scores indicating more accepting attitudes. The total score for the ATDS was 40 points. Based on the pre-program responses, the Cronbach’s alpha for attitude toward dementia was 0.78. Surveys were administered in approximately 5 minutes immediately before and after the program.
When evaluating learning goal achievement, the ability to step into the shoes of someone with dementia and think concretely were considered crucial. Therefore, the content of participants’ worksheets, understanding that they represented the students’ progress on the learning goals was examined.
Data Analysis
Pre–post changes in attitude toward dementia (Quantitative)
Analyses were conducted using SPSS Statistics 27.0 (IBM Corp., Armonk, NY, USA). As a Shapiro–Wilk test did not confirm data normality, a nonparametric test was performed. Concerning changes in attitude toward PwD, a Wilcoxon signed-rank test was performed to investigate pre–post changes in total scores and scores for each ATDS item. The two new questions on attitude concerning how to respond to PwD were also compared pre- and post-program using the Wilcoxon signed-rank test. The significance level was set at 5%.
Achievement of learning goals (Qualitative)
First, for Learning Goal 1 (Table 2), the number of participants who responded that they empathized with each character was summed. Subsequently, examples of participant responses to the question, “What do you think they felt?” concerning that character were presented. Second, for Learning Goal 2 (Table 2), a qualitative inductive analysis was performed. Descriptions of realizations that connected to concrete behaviors from the relevant sections of the individual worksheets were extracted, with one behavior considered one unit, and categorized these data based on semantic similarity.
Results
Pre–post Changes in Attitude Toward Dementia
Of the 102 respondents, aggregate results were analyzed for the 80 who provided consent and completed the ATDS and additional two items both pre- and post-program.
Attributes of the analysis set
The 80 participants comprised 54 women (67.5%) and 26 men (32.5%). Most participants were in their 60s (38.8%), and approximately 65% were aged ≥60 years (Table 4).
Attributes of the Questionnaire Survey Analysis Set (n = 80).

Pre-post Changes in ATDS Score and Attitudes Toward PwD
ATDS
A higher total ATDS score indicated a more accepting attitude. The mean total score rose significantly after the program (32.1 vs. 33.7; p < .001). Scores for individual questions were examined: the total mean score for “I do not know how to interact with PwD” rose from 2.7 to 3.2 points.
Attitude
Scores for “I want to devise concrete plans to find a role in community activities for people showing signs of dementia to allow them to continue participating” rose significantly after the program (p = .009; Table 5).
Changes in Dementia Acceptance Scale Mean Score and Attitude Concerning How to Respond to People With Dementia Pre- and Post-Program (n = 80).

Note. Wilcoxon signed-rank test. IQR = interquartile range.
Achievement of Learning Goals
Contemplating how to respond as a personally relevant matter
The analysis set comprised 77 participants. The analysis revealed the following: 41 participants empathized with Mr. Chiba, 18 with his wife, 12 with the community activity’s leader, two with neighborhood association participant A (who criticizes Mr. Chiba), and four with neighborhood association participant B (who suggests that Mr. Chiba resign from his position as treasurer).
Reasons for empathizing were as follows. For Mr. Chiba, the participants described uneasiness, disorientation, embarrassment, and a state of not understanding why what had happened had occurred, with statements such as the following: “discomfort and disorientation at having his mistake pointed out and uneasiness about possibly having dementia” and “his pride was hurt, and he couldn’t accept it, so he felt anger and uneasiness.” The second most common response was concerning Mr. Chiba’s wife. Participants wrote that she would also be feeling distressed at the appearance of dementia symptoms and even relayed that they had experienced this themselves. Their statements included the following: “she’s distressed about how best to understand and cope with her husband’s condition,” “she doesn’t know how things will turn out and doesn’t know what to do,” and “it felt close to home because I’ve dealt with dementia in my own family.” Eighteen participants responded that they empathized most with the leader or attendees of the community activity because they had had similar experiences, with statements such as: “I’ve dealt with several people who are verging on dementia” and “it’s similar to my perception of my father-in-law with dementia” (Table 6).
Learning Concerning Thinking About How to Respond as a Personally Relevant Matter (n = 77).

Concrete ways to respond to PwD in the community
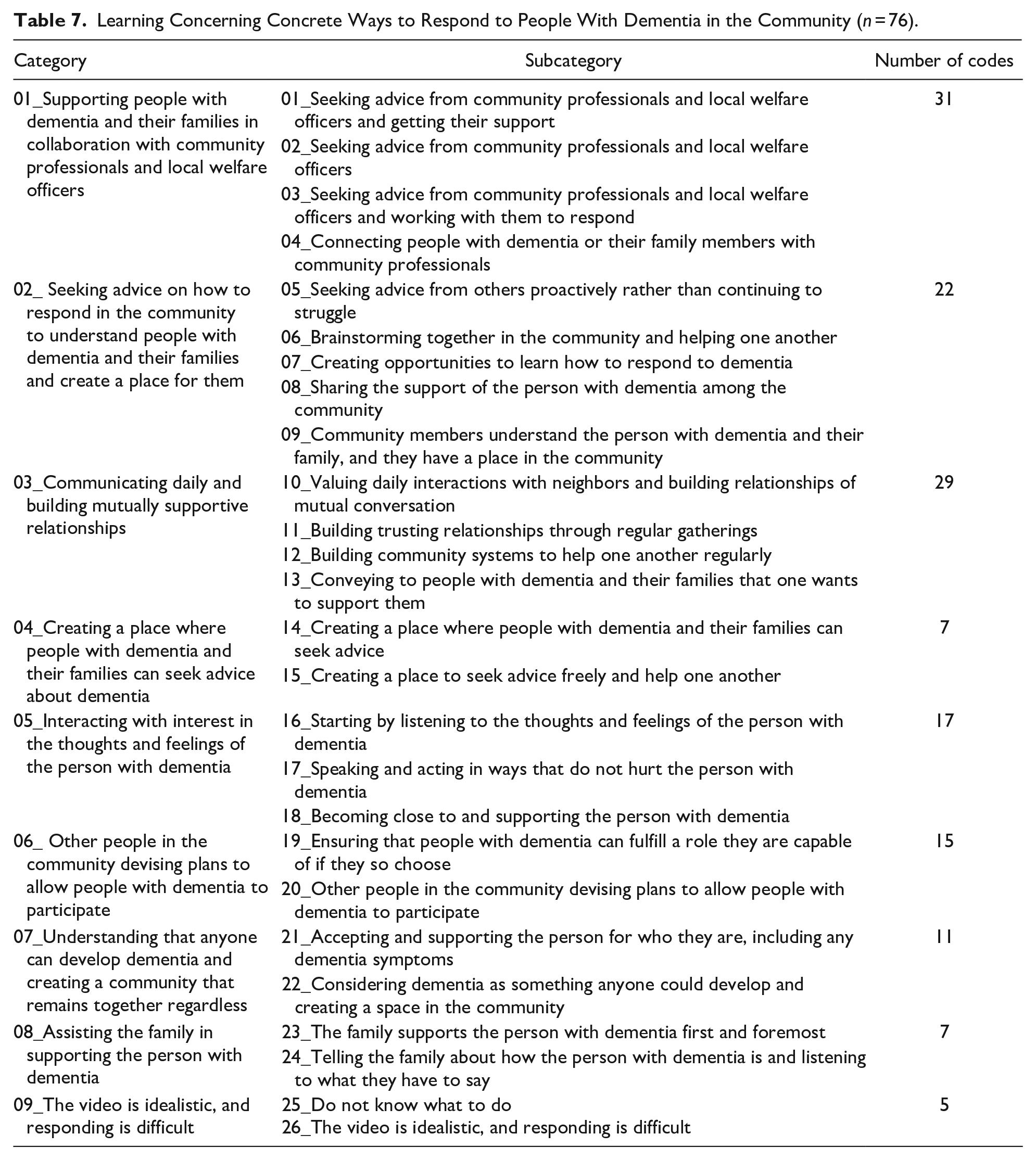
The analysis set comprised 76 participants. Analysis resulted in the creation of 144 codes, 26 subcategories, and 9 learning categories (Table 7). Categories are presented in square brackets [ ] and subcategories in angle brackets ⟨ ⟩. The first category was [01_Supporting PwD and their families in collaboration with community professionals and local welfare officers], with four subcategories. The first was ⟨01_Seeking advice from community professionals and local welfare officers and getting their support⟩. The second category was [02_ Seeking advice on how to respond in the community to understand PwD and their families and create a place for them], yielding five subcategories, such as ⟨05_Seeking advice from others proactively rather than continuing to struggle⟩. The third category was [03_Communicating daily and building mutually supportive relationships], with four subcategories, such as ⟨10_Valuing daily interactions with neighbors and building relationships of mutual conversation⟩. The fourth category was [04_Creating a place where PwD and their families can seek advice about dementia], including two subcategories. The fifth category was [05_Interacting with interest in the thoughts and feelings of PwD], yielding three subcategories, such as ⟨16_Starting by listening to the thoughts and feelings of the person with dementia⟩. The sixth category was [06_Other people in the community devising plans to allow PwD to participate], with two subcategories, such as ⟨19_Ensuring that PwD can fulfill a role they are capable of if they so choose⟩. The seventh category was [07_Understanding that anyone can develop dementia and creating a community that remains together regardless], with two subcategories, such as ⟨21_Accepting and supporting the person for who they are, including any dementia symptoms⟩. The eighth category was [08_Assisting the family in supporting the person with dementia], with two subcategories, such as ⟨23_The family supports the person with dementia first and foremost⟩. Finally, the ninth category was [09_The video is idealistic, and responding is difficult], with two subcategories, such as ⟨25_Do not know what to do⟩.
Learning Concerning Concrete Ways to Respond to People With Dementia in the Community (n = 76).
Discussion
Usefulness of the Community Dementia Education Program
This study discussed the usefulness of the education program from the perspective of the developed materials’ features and the program structure according to participants’ responses.
Contemplate responding focusing on the person with dementia based on challenges from various perspectives by watching scenario stories
Results for Learning Goal 1 showed that over half of the participants (n = 41) watched the video from the perspective of the person with dementia, 18 from the wife’s perspective, and another 18 watched while empathizing with the community activity’s leader or attendees. Participants empathized with certain characters because they had had similar experiences. Nearly 70% of the participants had attended a Ninchisho supporter training session, and almost 20% had attended a Ninchisho supporter step-up session. Thus, the participants likely had engaged with PwD from a standpoint similar to that of the community activity attendees or leader. This may be why many participants watched the video from that perspective.
Some dementia education programs utilize virtual reality to facilitate understanding of the perspective of a person with dementia through vicarious experience (Sari et al., 2020). In the present education program, camera work from the perspective of the person with dementia hints about what their inner voice might be saying. An action camera likely facilitated understanding of the perspective and feelings of a person with dementia. Moreover, the educational materials presented the feelings of the person with dementia where attendees experienced that person’s conflict with them, their family, and a professional, along with the changing relationships between them in a story format centering on a community activity. Thus, they likely caused the participants to think deeply about the feelings of the wife, the community activity attendees, and the leader.
Next, the educational materials were created to teach participants to contemplate what the person with dementia wants. Thus, their wishes could be respected rather than resolving problems based on others’ opinions when dementia symptoms or signs appear. Concerning concrete responses (Learning Goal 2), the participants learned about [05_Interacting with interest in the thoughts and feelings of PwD]. This included ⟨16_Starting by listening to the thoughts and feelings of the person with dementia⟩. As evidenced by the research team members’ evaluations as well, the present education program prompted participants to focus primarily on the person with dementia despite the tendency to emphasize engagement with the family and surrounding people when “dementia” is mentioned. However, item 1 of the ATDS, “I would like to respect their wishes as much as possible, even if they develop dementia,” did not show a significant pre–post difference. This may be because the participants started with a high score for attitude regarding respecting the wishes of PwD (4.8 out of 5). The worksheets show that, in terms of learning to think about responding as a personally relevant matter, a few participants empathized with community activity participant B, who suggested that the person with dementia resign from their position as treasurer. Thus, even if the wishes of PwD are respected, those around them may still adopt exclusionary behaviors owing to their cognitive deficits.
Next, learning about [01_Supporting PwD and their families in collaboration with community professionals and local welfare officers] was commonly noted, with 31 codes. This and subcategories such as ⟨5_Seeking advice from others proactively rather than continuing to struggle⟩ were understood to represent learning that shows an intention to consult with other concerned parties, such as community professionals and local welfare officers. Moreover, learning about [03_Communicating daily and building mutually supportive relationships] was demonstrated. This suggested that the participants began to consider daily communication, mutual helping behavior, and building interpersonal relationships as a necessary foundation for the local community. Uchida et al. (2020) examined attitudes toward dementia among local residents and revealed that people with a high score for helping each other and building relationships, also had a high score for acceptance of dementia. Therefore, learning through the educational program will help create a dementia-inclusive society.
A dementia-inclusive society is one in which PwD and their caregivers can actively participate and have a sense of belonging place. However, Japan has a cultural and social background where people tend to understand dementia in terms of relationships with family members and society. Drott (2018) noted that the Japanese discourse on senility has commonly expressed anxieties over the difficulties faced by caregivers or the potential of senile elders to engage in socially disruptive behavior owing to cultural factors. Therefore, video materials with scenario stories could facilitate sharing a positive image of the relationship with PwD, which continues despite the issues faced in the community. Specifically, it could assist in cultivating a culture that promotes a dementia-inclusive society.
Concrete strategies to increase the potential of PwD and foster community participation
The evaluation of attitude toward dementia showed a significant pre–post difference in scores for “I want to devise concrete plans to find a role in community activities for people showing signs of dementia to allow them to continue participating.” Participants had also learned about concrete, practical strategies, as evidenced by [05_Interacting with interest in the thoughts and feelings of PwD] and [06_Other people in the community devising plans to allow PwD to participate], with 15 and 17 codes, respectively.
Concerning Ninchisho supporter training sessions, attendees who have learned more about dementia actually have greater anxiety when they or one of their family members develop dementia (Teshima, 2020). However, the participants contemplated problems, showed solutions, and offered feelings of hope. This effective learning is likely to have been owing to the development of educational materials that reproduced a realistic and common scenario that aimed to reduce psychological resistance as much as possible, understanding that societal prejudice against dementia remains (Hung et al., 2021). Further, participants hoped that PwD could continue to participate socially and interact with others (Nagai et al., 2021). Moreover, the education program was structured such that participants organized their thoughts after watching the video scenarios. They considered the question “What would you do if it were you?” and completed worksheets. Subsequently, they learned about different viewpoints by listening to others’ opinions. These activities likely made the participants consider their ideas in the context of diverse values and think concretely about dementia as a personally relevant matter.
In sum, the program format incorporated mutual learning—a principle of adult learning theory. Learning from other participants’ experiences through group work likely allowed the participants to think about concrete responses.
Implications for Community Dementia Education
Pre- and post-test results confirmed that those who attended the education program developed a more accepting attitude toward PwD and could contemplate solutions to allow PwD to live and play a role in their community.
The learning content, corresponding to learning goals obtained from individual participant worksheets, confirmed that the participants could take the various perspectives of a person with dementia, a family member, or a community member and perceive dementia as something that could happen to them. Further, the participants could think concretely about how to respond to PwD in the community based on their feelings.
Considering these findings, the recommendations for the community dementia education are as follows. First, there should be a scenario story that makes viewers realize that even an issue with PwD in the community can be resolved through interaction with other people, including family members, neighbors, and professionals. According to adult learning principles (Bryan et al., 2009), adults’ previous experiences must be respected and built upon. A scenario story is needed that allows participants to reflect on their own experiences and to consider how they would handle the situation from the perspective of various people.
Further, this story should be converted to visual media to foster a shared impression of the challenges faced by PwD in the community and how they live. Scenario teaching can bridge the gap between knowledge and practical reality by simulating real world situations that include behavior and attitudes (McNaughton et al., 2008). The visualization can simulate the challenges and living conditions of PwDs who experience stigma and find it difficult to talk about it in public and help them understand the reality of the situation.
The scenarios are presented in sections, and individual work can be done to narrow down the points and organize individual thoughts. This allows for more effective group discussions. Subsequently, programs should introduce mutual learning based on adult learning theory in which individuals learn from other participants’ experiences through group work. By watching the video, a common understanding can be created, enabling more effective goal-oriented discussions.
Limitations and Challenges
The developed education program was useful. However, the mean ATDS score was 32.1 points pre-program and 33.7 points post-program compared to the scores for Ninchisho supporter training session participants (29.58 points pre-session and 32.78 points post-session) as surveyed by Kim et al. (2011). The participants were a group with an initially high level of dementia acceptance. Further investigation is necessary to determine whether this education program aids populations with low dementia acceptance. One of the two newly added items—“I want to use various assistance services when dementia causes problems”—had a considerably high mean score of 4.8 even before the program. Therefore, a significant increase in the score owing to program implementation could not be confirmed for that item. In the future, it is necessary to consider the items’ content and response method. Concerning learning content compared to learning goals, some participants viewed the hopes depicted as idealistic and felt that a realistic response was more difficult. A facilitation guide describing how to connect to mutual learning (e.g., in group work) when such opinions arise is likely necessary.
The education program was implemented after creating a PowerPoint and worksheets in addition to the video materials; however, owing to the 2019 coronavirus disease pandemic, it was impossible to host group programs, and further validation and improvement have been deferred. This study will hopefully resume once the pandemic is under control.
Finally, this study was conducted in Japan. In the Asia Pacific region, dementia-friendly efforts have reflected an array of vibrant cultures and traditions for several years (Alzheimer’s Disease International, 2017). Thus, the results of this study may not be generalizable to other cultures.
Conclusion
This study developed educational materials for mutual learning of how to respond to dementia for local residents participating in community activities alongside local residents and stakeholders with reference to instructional design. Subsequently, the program was implemented and evaluated.
The program could successfully teach participants to take the perspectives of various other people to view dementia as something relevant to themselves and think about ways of responding to PwD, considering their feelings. The results suggest that community dementia education aiming for a dementia-inclusive society should be developed through co-design with community members and stakeholders. It is important to create scenario stories that depict the desire to be a part of the community even with dementia, use visual depictions to create a shared impression, and facilitate mutual learning.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chiba City and the Chiba University Collaborative Research Project Grant [H30].
Ethical Considerations
This study was approved by the Ethics Review Board of the Graduate School of Nursing, Chiba University, No. 30-2 (Development & Research) and No. 30-93 (Evaluation & Training).