
Abstract
Objective:
To determine the burden and quality of life of caregivers of stroke survivors with cognitive impairment in selected healthcare facilities in Anambra State, Nigeria.
Methods:
This was a cross-sectional survey using the World Health Organization QOL-BREF and Caregiver Strain Index (CSI) as instruments. Descriptive statistics of frequency, percentage counts, mean and standard deviation were used to summarize the socio-demographics. Spearman’s ranked order correlation; Mann–Whitney U test assessed the correlation and gender and age difference in QoL and caregiver’s burden. Alpha level was set at 0.05.
Results:
Physical health domain of QOL was slightly moderate (53.29 ± 15.19), psychological health was low (46.33 ± 16.96), social relationship was slightly moderate (51.16 ± 0.31), environmental health was slightly moderate (51.22 ± 15.88), the burden of caregivers was high (6.35 ± 1.29).
Conclusion:
The quality of life of the caregivers of stroke survivors with cognitive impairment was moderate, and the caregivers’ stress was high in the sample of the population studied.
Background
Stroke is one of the leading causes of severe long-term disability in adults worldwide, causing an enormous emotional and socioeconomic burden for patients, their families, and health services (Ibikunle et al., 2021). The current epidemiological data indicate that 16.9 million people suffer a stroke each year, which represents a global incidence of 258/100,000/year, with marked differences between high- and low-income countries, and an age-adjusted incidence 1.5 times higher in men than in women (Béjot et al., 2016). The overall incidence of stroke in Africa and Nigeria is 316 per 100,000 and 1.31 per 1,000 per annum respectively (Sanya et al., 2015). However, in Anambra State, Nigeria the prevalence of stroke is estimated at 1.63 per 1,000 per annum (Enwereji et al., 2014). It has been shown that stroke etiology is multifactorial (Christensen & Cordonnier, 2021). As of 2019, the five leading risk factors of stroke were high systolic blood pressure (contributing to 79.6 million), high body-mass index by 55.5% of total stroke (34.9 million), high fasting plasma glucose by 24.3% (28.9 million), ambient particulate matter pollution by 20.2%, and smoking (25.3 million) 17.6% (Lip & Ntaios, 2022). Some other risk factors that cannot be discountenanced according to previous studies include age at menopause for females (Lip & Ntaios, 2022), thrombosis and hemostasis (Dlamini & Jordan, 2021), preterm birth (Qureshi et al., 2021), Covid-19 (Georgakis & Gill, 2021), gene (Alnsasra et al., 2021), cardiac disease (Quinn et al., 2021). However, advancements in treatments and acute rehabilitation services (especially in developed countries) have resulted in increased survival of people affected by stroke, with many of such survivors ending up with long-term disabilities and impairments which adversely affect their cognition (Teasell et al., 2014), This cognitive impairment further complicates the stroke burden even among caregivers (Chen et al., 2017; Koh et al., 2021; Sun et al., 2014).
Post-stroke cognitive impairment occurs frequently in patients with stroke (Zauszniewski et al., 2021). The prevalence of post-stroke cognitive impairment ranges from 20% to 80% and varies between countries, races, and diagnostic criteria. The risk of post-stroke cognitive impairment is related to demographic factors like age, education, occupation, and some vascular factors (Zauszniewski et al., 2021). The underlying mechanisms of post-stroke cognitive impairment seem not to be known in detail. However, the neuroanatomical lesions caused by the stroke on strategic areas such as the hippocampus and the white matter lesions (WMLs), the cerebral microbleeds (CMBs) due to the small cerebrovascular Diseases and the mixed Alzheimer’s Disease (AD) with stroke, alone or in combination, contribute to the pathogenesis of post-stroke cognitive impairment. The treatment of post-stroke cognitive impairment may benefit not only from the anti-dementia drugs but also from the management measures for cerebrovascular diseases (Zauszniewski et al., 2021). It has been shown that the stroke burden is not only on the side of patients but also on their caregivers. A survey of the differences among caregivers on coping resources and mental health showed that stroke has the highest impact on caregivers followed by dementia (Owusu, 2021) and this has required them an inconsiderable amount of effort for their rehabilitation and planning of their daily events (Okonkwo et al., 2017). Most importantly the quality of life of such caregivers has been negatively affected (Wittenberg et al., 2021). A study had reported that the cognitive status of sub-acute stokes survivors with compromised cognition could improve significantly as well as those of non-cognitive impaired stroke survivors when subjected to long-term PNF and TSBT intervention (Okonkwo, Okoye, Ezeukwu, et al., 2017). This implies that an improvement in the cognitive status of stroke survivors with cognitive impairment can help reduce the burden of the caregivers and invariably improve their QoL.
Quality of life refers to the individual’s perception of their position with the respect to the context of the culture and value systems in which they live and their goals, expectations, standards, and concerns (Kim, 2014). It is a broad concept encompassing a person’s physical health, psychological state, level of independence, social relationships, and personal beliefs as well as the environmental factors that affect a person (Barcaccia et al., 2013). More so, QoL is an overwhelming term for the quality of the various domains in life. It is a standard level that consists of the expectations of an individual or society for a good life. These expectations are guided by the values, goals, and socio-cultural context in individual lives. It is a subjective, multidimensional concept that defines a standard level for emotional, physical, material, and social well-being. It serves as a reference against which an individual or society can measure the different domains of one’s own life (Gunn & Var, 2002). Quality of life should not be confused with the concept of standard of living, which is based primarily on income (Khajedaluee et al., 2013). Standard indicators of the quality of life include not only wealth and employment but also the built environment, physical and mental health, education, recreation and leisure time, and social belonging (Gregory et al., 2009). Significantly Okonkwo, Okoye, Ibeneme, et al., (2017) in their previous study noted that there was strong evidence to explain that adaptive neural plasticity induced by PNF and TSBT enhanced functional motor recovery and hence improve QoL of cognitively impaired stroke survivors. This shows that amelioration of cognitive impairment can improve the quality of life of stroke survivors as well as that of the caregivers.
The quality of life and burden of caregivers of stroke survivors is not a virgin area of study, especially in the western world where QoL and the burden of care of individuals are mostly emphasized (Alquwez & Alshahrani, 2021; Byun & Evans, 2015; Carod-Artal, 2012; Caro et al., 2017, 2018; Moura et al., 2022; Persson et al., 2015). In lesser quantity, this same area has been explored in African settings (Akosile et al., 2013; Badaru et al., 2017; Bello et al., 2021; Imarhiagbe et al., 2017; Ogunlana et al., 2014). Irrespective of the in-depth study of this area as it concerns caregivers of stroke survivors, little to no attention has been paid specifically to how QoL and the burden of the caregivers relate with each other, especially among caregivers whose patients are cognitively impaired. Hence this study determined the relationship existing between QoL and the burden of caregivers of stroke survivors with cognitive impairment in selected healthcare facilities in Anambra State, Nigeria. It is thereby hypothesized that there will be no significant correlation amongst the scores of different components of Quality of life, Burden scores and selected socio-demographic characteristics of caregivers of stroke survivors with cognitive impairment in selected healthcare facilities in Anambra State.
Materials and Methods
Research Design
The study adopted a cross-sectional design.
Research Population
Participants comprised caregivers of stroke survivors with cognitive impairment residents in Anambra State, Nigeria. They were enrolled from the following health facilities: Nnamdi Azikiwe University Teaching Hospital Nnewi, Landmark Physiotherapy services Nnewi, General Hospital Ekwulobia, General Hospital Onitsha, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital Amaku Awka, and General Hospital Enugwu-Ukwu all in Anambra State, Nigeria.
Eligibility
The inclusion criteria were caregivers of stroke survivors with cognitive impairment aged 18 years and above, fluent in either English or Igbo language, attending physiotherapy outpatient rehabilitation programs, and who had been with the stroke survivors for a minimum of 3 months at the time of the study. Caregivers of patients with stroke on admission and part-time caregivers of stroke survivors were excluded from the study.
Sample size/Sampling Technique
A sample size of 55 was calculated using G*Power 3.0.1.0 which has a 95% power of detecting a difference of 0.25 at an alpha level of .05. Participants for this study were recruited using the purposive sampling technique.
Research Instruments
World Health Organization (WHOQOL)-BREF
This is used to measure the quality of life of individuals and populations. The WHOQOL-BREF is a shorter version of the WHOQOL-100. Both were developed by the World Health Organization (WHO) and published in 1995. It was developed over several years and from 15 centers around the world (World Health Organization, 2020). The questions stem from multiple statements about the quality of life, health, and well-being of people with and without disease, and health professionals (World Health Organization, 2020). It has been tested for reliability and validity (Cambridge University Press, 1998; World Health Organization, 2020). The WHOQOL-BREF has shown good discriminate validity, content validity, internal consistency, and test-retest reliability (Cambridge University Press, 1998; Skevington et al., 2004). The WHOQOL-BREF correlates well with the WHOQOL-100 suggesting that it is a suitable alternative to the longer version (Cambridge University Press, 1998; Skevington et al., 2004) if time does not permit. It has been tested in multiple languages, cultural groups, and disease populations. Searches of literature databases or Google Scholar will bring up dozens more research articles than can be listed here (Skevington et al., 2004) note that, after testing, the WHOQOL-BREF is a sound, cross-culturally valid assessment of QOL. A work by Skevington et al. (2004) provided detailed Psychometric Properties such as internal consistency. As a measure of the scale’s internal consistency. Domains A, B, and C, that is, physical health 0.82, psychological 0.81, environment 0.80, but marginal for social relationships 0.68. Across sites, results were consistently high with most of the Cronbach’s alpha in Domains 1 and 2 above 0.75, and in the range of 0.51 to 0.77 for Domain 3, and 0.65 to 0.87 for Domain 4. Alpha analyses carried out by systematically removing and then replacing each item showed that all 26 items made a significant contribution to the variance in the WHOQOLBREF. A higher score denotes a better quality of life.
Caregiver Strain Index (CSI)
This will be used to estimate the level of burden of caring for stroke survivors with cognitive impairment on caregivers. It is a 13-item questionnaire that measures strain related to taking care of stroke survivors with cognitive impairment (Sullivan, 2002). reported that the CSI construct validity is supported by correlations with the physical and emotional health of the caregiver and with the subjective view of the caregiving situation. CSI has a high internal consistency (0.86) (Sullivan, 2002). There is at least one item for each of the following major domains: Employment, Physical, Financial, Social, and Time. Positive responses to seven or more items on the index indicate a greater level of strain (Sullivan, 2002). The CSI consists of 13 items that are posed to caregivers as questions. The caregivers have to answer YES or NO. A “NO” is given a value “0” while a “YES” is given a value of “1” The CSI is then computed by summing “0” (no) and “1” (yes) responses to give a total yes of 13, in other words, the scores of several “YES” answer. This simply means that the CSI scores range from 0 to 13. Positives responses to seven or more on the index indicate a greater level of stress (Bellani et al., 2016). According to Hartford Institute for Geriatric Nursing (HIGN), a score of 7 or more would indicate a greater level of stress (Gerdtham & Ruhm, 2006; Ruhm, 2015).
Procedure for Data Collection
Ethical approval was sought and obtained from the Ethical Review Committee of the Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, College of Health Sciences, Nnewi Campus. A letter of introduction was obtained from the Head of the Department of Medical Rehabilitation and sent to the Head of the Department of the healthcare facilities under study. Informed consent was sought and obtained from the participants of this study before the administration of the questionnaire. All the participants were informed that their responses would remain confidential. Research assistants were recruited and tutored on the procedure of this research. They helped in administering the research instruments to the participants. An estimated period of 4 weeks was utilized to administer the questionnaires to the participants. The research was carried out among caregivers of stroke survivors in some selected health facilities in Anambra State, Nigeria. Information on participant’s sociodemographic data (age, sex, duration of illness of the stroke patient they are caring for, average number of days such participants stay with the patients per week, and average number of hours the participants stay with the patient per day, educational level) was as well obtained. Quality of life and burden of caregivers of stroke survivors with cognitive impairment was assessed subjectively using a short form 12-items health survey and caregiver’s strain index respectively. All the data that was collected was anonymized and entered into a password-protected electronic spreadsheet and was stored in a flash accessible only to the statistician involved in the data analysis.
Analysis of Data
The demographic and clinical variable data, as well as the scores on the WHOQOL-Brief Questionnaire and the CSI—Questionnaire, were summarized using frequency counts and percentages, mean and standard deviation with Statistical Package for Social Sciences (SPSS) version 27. Inferential statistics of Spearman rank-order correlation and Mann-Whitney U test were used to test the relationship and sex and marital status score differences between the variables. Alpha level was set at p < .05.
Results
Returning Rate of Questionnaires
The total number of questionnaires dispersed was 55 and the same number was returned making a return rate of 100% (Table 1).
Socio-Demographic Care-Related Profiles of the Participants.

A total of 55 caregivers participated in the study; 27 males and 28 females. The mean age of the participants was 42.76 ± 10.60. Regarding educational attainment, 25 (50.9%) participants were secondary school leavers, 15 (27.3%), and 12 (21.8%) were primary and tertiary school leavers respectively. Most of the respondents 25 (45.5%) were married, 12 (21.8%) were single, 14 (25.5%) were separated and 4 (7.3%) were widowed. The number of days per week the caregiver offered care is as thus: for 1 to 3 days 6 (10.9%), 4 to 5 days 31 (56.4%), 6 to 7 days 18 (32.7%). Care hours per day were recorded as follows: 1 to 5 hours 16 (29.1%), 6 to 10 hours 12 (21.8%), 11 to 15 hours 14 (25.5%) and >15 hours 13 (23.6%). Care duration for less than 6 months was 17 (30.9%), 6 to 12 months 30 (54.5%), and less than 12 months was 8 (14%). Post-stroke duration of 6 to 12 months had the highest number of respondents (54.5%) followed by greater than 12 months (30.9%) and less than 6 months recorded the least percentage of participants (10.9%).
Table 2. The physical health domain of quality of life was slightly moderate (53.29 ± 15.19), Psychological health was low (46.33 ± 16.96), Social relationship was slightly moderate (51.16 ± 0.31), environmental health was slightly moderate (51.22 ± 15.88), the burden of caregivers was high (6.35 ± 1.29).
Mean Age, Quality of Life, and Burden of the Participants.

Table 3a result revealed that there was a significant moderate positive correlation between the physical health component of the QoL and psychological health (rho = .51, p < .001), social relationship (rho = 0.63, p < .001), and environmental health (rho = 0.55, p < .001). There was also a significant moderate positive correlation between the psychological health component of the QoL and social relationship (rho = .46, p < .001), environmental health (rho = 0.45, p < .001), and burden of caregivers of stroke survivors (rho = 0.45, p < .001). The social relationship also showed a significant moderate positive correlation with the environmental health component of QoL (rho = .574, p < .001). Educational level and burden of caregivers showed a significant moderate yet positive correlation (rho = .316, p = .005). Care days per week and the psychological health of the participants showed a significant weak yet positive correlation. No other paired variable showed a significant correlation.
(a) Spearman Rank-Order Correlation Showing the Relationships Between Quality of life, the Burden of Caregivers, Age, and Educational Level of the Participants.
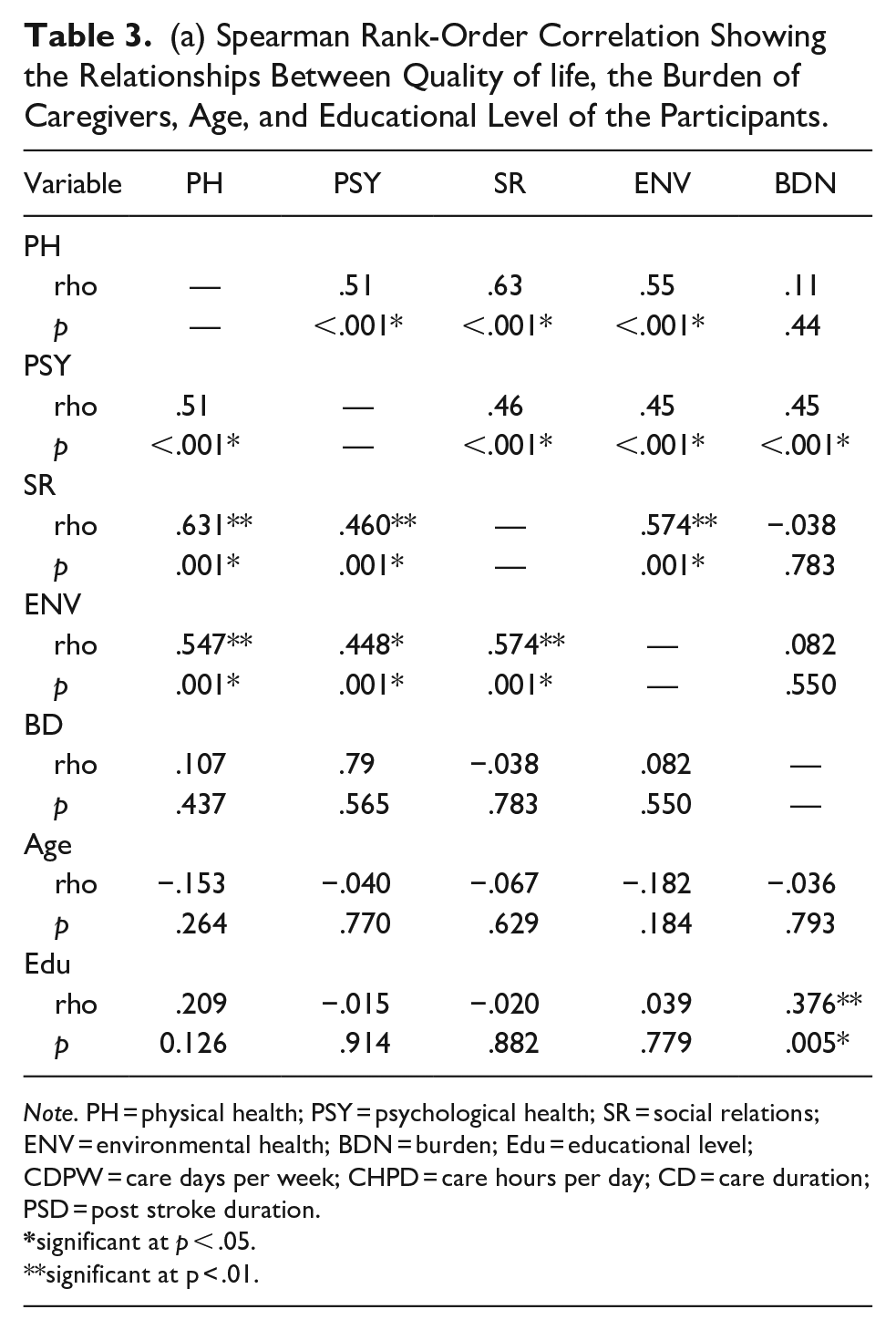
Note. PH = physical health; PSY = psychological health; SR = social relations; ENV = environmental health; BDN = burden; Edu = educational level; CDPW = care days per week; CHPD = care hours per day; CD = care duration; PSD = post stroke duration.
significant at p < .05.
significant at p < .01.
Table 3b CDPW had a moderate yet positive relationship with the PSY component of the quality of life (rho = .28, p < .04. CDPW has no relationship with PH (rho = .11, p > .45), SR (rho = .01, p > .94), ENV. (rho = .21, p > .12) and BDN (rho = .14, p > .30. CHPD has no relationships with PH (rho = 0.52, p > .267), PSY (rho = 0.23, p > .09) SR (rho = 0.10, p > .45), ENV (rho = 0.1, p > .92), and BDN (rho = .09, p > .53. CD has no relationship with PH (rho = −.13, p > .35), PSY (rho = −.04, p > .80), SR (rho = −.10, p > .46), ENV (rho = .01, p > .92), and BDN (rho = −.13, p > .36. PSD has no relationship with PH (rho = .10, p > .49), PSY (rho = .09, p > .54), SR (rho = .04, p > .76), ENV (rho = .05, p > .69, and BDN (rho = −0.08, p > .57)
(b) Spearman Rank-Order Correlation Showing the Relationships Between Quality of life, the Burden of Care and Vital Parameters of the Participants.
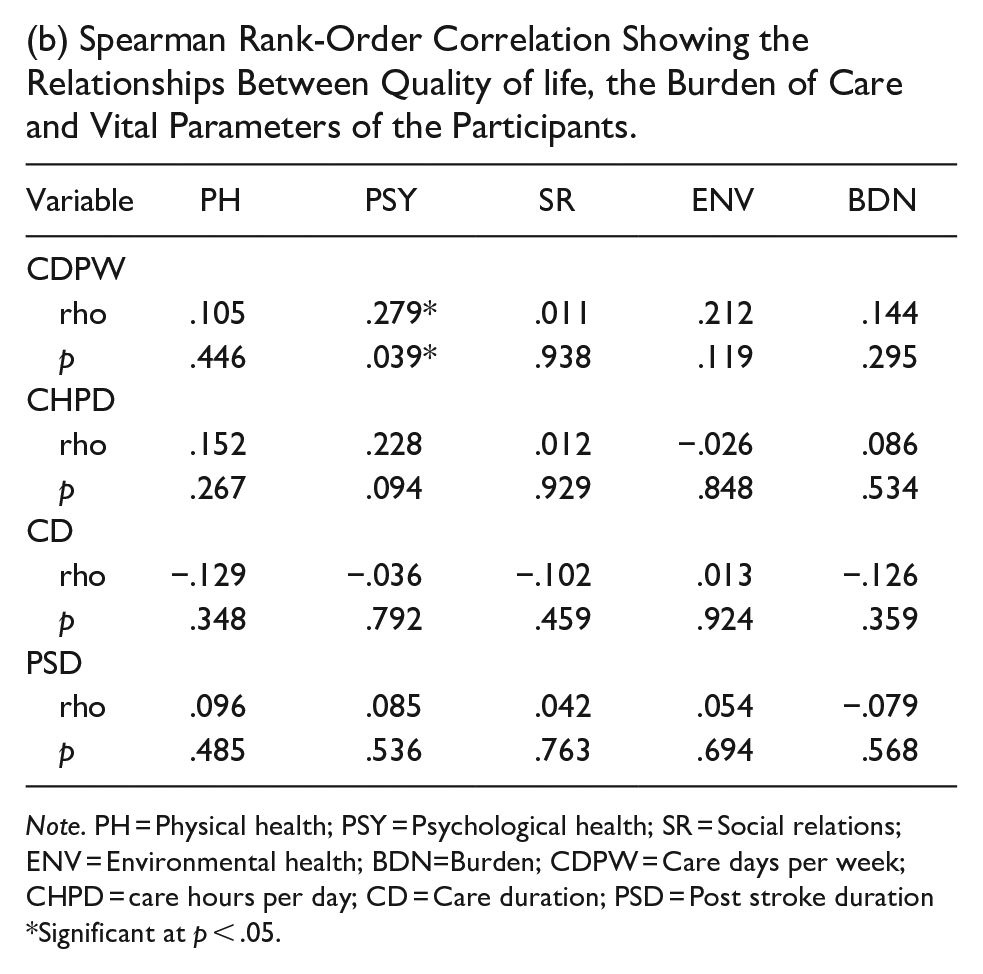
Note. PH = Physical health; PSY = Psychological health; SR = Social relations; ENV = Environmental health; BDN=Burden; CDPW = Care days per week; CHPD = care hours per day; CD = Care duration; PSD = Post stroke duration *Significant at p < .05.
Table 4 result showed that none of the variables (physical, psychological, social, and environmental health and burden of caregivers) had a significant sex difference. Physical health u = 340, p = .52, Psychological health u = 351, p = .65, Social relationship u = 365, p = .062, Environment u = 376, p = .98, Burden u = 369, p = .88
Mann–Whitney U Test Assessing the Sex Differences in Quality of Life and Burden Among the Participants.

Table 5 result showed that none of the variables (physical, psychological, social, environmental health, and burden of caregivers) had a significant marital status difference. Physical health u = 6.09, p = .11, Psychological health u = 1.10, p = .78, Social relationship u = 4.03, p = .026, Environment u = 4.44, p = .22, Burden u = 6.85, p = .08
Mann–Whitney U Test Assessing the Marital Status Differences in Quality of Life and burden Among the Participants.

Discussion
The emphasis on stroke rehabilitation needs to shift from a patient-focused approach to a combined patient- and caregiver-focused paradigm because these individuals are central in preserving rehabilitation gains and the long-term well-being of stroke survivors (Blake et al., 2003; Revenson et al., 2016). However, the success of early attempts to support caregivers has been limited, largely because the determinants of caregiving burden and the needs of caregivers remain poorly understood including their quality of life (Johansson & Wild, 2011; Quinn et al., 2014; Reimer et al., 1998). Most of the cognitively impaired stroke survivors that received care in this study were in the chronic stage at the time the data was collated. We speculate that caring for stroke patients with cognitive impairment, and at the chronic stage of their disability could be more debilitating and depressing than for those with acute conditions or not cognitively impaired. Also, this study revealed that most caregivers were not on full-time (24 hours) caregiving, as well, most of them operated from their various places of domicile. The caregivers operated on a part-time basis, the family careers continue with the caring until the hired caregivers report back.
Assessing the quality of life and burden of care in an individual caregiver of stroke survivor with cognitive impairment can provide important information for the development of health policies that address the actual health needs of such population. In the study sample, most caregivers were predominantly seen among middle-aged adults. The physical health domain of quality of life was slightly moderate, psychological health was low, the social relationship was slightly moderate, environmental health was slightly moderate, and the burden of caregivers was high. In other words, the caregivers exhibited a high burden of care although there was moderate health in all the quality of life domains except psychological health. This may be attributed to the high burden of care experienced by the caregivers which inadvertently led to stress with concomitant decreased psychological well-being.
There was a relationship between the physical health component of the QoL and psychological health. This finding is significant when we realize that if the physical health component of the quality of life is good the psychological health component will be stable and this can impact positively on the caregiver’s ability to deliver quality caregiving to the care recipient. The contrast will be the case when the caregiver is facing a lot of psychological challenges like poor bodily image and appearance, negative feelings, poor low esteem and cognitive challenges. This implies that caregivers who present with low physical health components would most likely present with psychological health leading to an increased burden on the caregivers. Previous studies had noted that when stress (Zarit, 2002) is maintained over time it places a burden on the caregiver which has negative physical health effects and psychological consequences (Carretero et al., 2009) such as anxiety, depression, and psychological distress (Pinquart & Sörensen, 2005). The social relationship was equally found to be moderately associated with environmental health. When the environmental health component of the QoL of caregivers such as financial resources, freedom and security, health and social care, physical environment, transportation etcetera are poor, it will impact negatively on the quality of social interactions like personal relationships, social support and sexual activity hence adding to the caregivers’ strain. For example, numerous studies had reported that social support can be effective in improving the well-being of caregivers. Specifically, a previous study reported that higher levels of social support reduce the negative effects of caregiving (Pinquart & Sörensen, 2005) and are associated with greater life satisfaction, less depression, less caregiver stress (Ruiz-Robledillo & Moya-Albiol, 2012) and lower risk of perceived burden (Jofré Aravena & Sanhueza Alvarado, 2010) It was also reported that caregivers who devout large amount of time to give care and who have few social ties are more likely to experience depressive symptoms (Cannuscio et al., 2004). Hence, the level of social support is considered predictive of burden (Kahriman & Zaybak, 2015; Manso Martíez et al., 2013). The further finding indicates that the psychological component of QoL and the social relationship have a significant moderate positive correlation. In line with this finding, a previous study had reported that female caregivers have greater social support than male caregivers with the negative impact of caregiving on mental health being high in women (Larrañaga et al., 2008). Interestingly, although social support could be protective of potential negative impacts on caregivers when the time devoted to informal caregiving is taken into account, it is seen that social support has a limited role in protecting the mental health of caregivers when many hours are devoted to caregiving (Masanet & La Parra, 2011). The moderate yet positive relation between the environmental health of QoL and the burden on caregivers of stroke survivors is an indication that good environmental health of QoL will lead to reduced caregivers strain. Improving the financial resources, physical safety, home environment, and other components of the environmental health where the caregiver works will create a conducive environment and help to lessen the caregiver strain. This implies that the caregivers who are operating under a protected and conducive environment will have less caregiver strain and hence more ability to deliver care to the care recipient. Our study outcome also shows that social relationship was directly associated with the environmental health component of QoL. A previous study reported that factors in the social environment that are important to the health of the caregiver include those related to safety, violence, and social disorder in general, and more specific factors related to the type, quality, and stability of social connections, including social participation, social cohesion, social capital, and the collective efficacy of the neighborhood (or work) environment (Ahern & Galea, 2011). Caregivers who have the opportunities to engage in meaningful relationships, such as support from friends and family, have been associated with lower reported caregiver stress (Yatchmenoff et al., 1998) Furthermore, Song and Singer (2006) found that caregivers of family members with psychiatric disorders, satisfaction with social support was shown to have buffering effects on stress and depressive symptoms, although social support was not directly associated with caregiver stress relief . The current study found that educational level has a direct relationship with the caregiver strain. According to Adelman et al. (2014), the caregiver burden was greater in caregivers who had less educational attainment than those with more education. Also, caregivers had lower odds of feeling physically burdened and had increased odds of feeling mentally burdened by caregiving; this was related to their good health status. This is because the greater mental burden of caregivers with a higher education level may result from feared losses of autonomy, which increase with higher investment in education (Oedekoven et al., 2017). The authors are of the view that caregivers with higher education might feel more psychological strain than those with lower education because of a lack of job satisfaction, and low perception and evaluation of the caregiving job relative to their educational qualification. Most of them seem to have taken up the job of caregiving to meet their daily needs not because it is where they want to end. This finding has made us conclude that the educational status of the caregiver is one of the predictors of caregiver strain. We found no relationship between components of QoL, the burden on caregivers and other vital parameters of the participants except the care days per week which show a relationship with psychological health. This is supported by the previous finding that the number of hours spent caregiving determines or influences the negative effects on mental health hence adding to the burden of care of the caregivers (Masanet & La Parra, 2011). Similarly, Bugge et al. (1999) reported that the amount of time a caregiver spent helping a stroke patient, the amount of time the caregiver spent with the patient, and the caregiver’s health were all significantly associated with the level of strain experienced. The age of the caregivers in the sample was not associated with any of the components of the QoL or caregiver burden. This connotes that being an older or younger adult caregiver in the study sample does not determine the quality of life or the caregiver strain. This contrasted with a previous study where a post hoc analysis revealed that young adults reported less caregiver burden, less physical strain, and greater financial strain than older adults (Koumoutzis et al., 2021). Interestingly, also, linear regression analyses reported associations between caregiver burden and financial strain with emotional and physical strain for all respondents (Koumoutzis et al., 2021).
In the sample, the QoL and burden of care of caregivers of stroke patients complicated with cognitive impairment were not gender-biased as stated by the outcome of this result. This, finding, however, was at variance with that of a previous study (Lubomski et al., 2014) which reported that—men caregivers are more burdened than their female counterparts; although the study was carried out among patients with Parkinson’s disease experiencing similar cognitive impairment and reported that men were more burdened than females. However, another study stated that gender differences arise because female caregivers have greater exposure to caregiving stressors, and differ in their appraisal, coping and availability of social support while managing these demands than men (Pinquart & Sorensen, 2006).
Our study revealed that the caregiver’s strain and QoL did not show any marital bias in the sample. Being single was never an advantage to being married nor did being widowed place itself in a more favorable condition than the separated. It could be assumed that there is not much feeling of deprivation across different gender statuses bearing in the outcome of this study. This is only when all things are equal that there is no potential factor of consideration. For instance, the individual involved is not married and still has problems in his marriage or workplace or says singleness did not mix with academics or any other interest. As a standalone, it could be true that marital status has no significant difference. We have to affirm, except proven otherwise, that gender and marital status have no significant difference across the studied variables.
Limitations
Some limitations to the present study ought to be acknowledged. The sample was non-randomized and bias cannot be completely ignored. The cross-sectional nature of the study did not allow the establishment of the direction of causality with findings only reported based on the observed relationships. It would be useful to conduct a longitudinal study to assess whether there are changes in caregivers’ burden and QoL and determine the variables that might affect those changes. Also, the stroke patients in this sample had cognitive impairment and we did not study the burden of care and QoL related to the clinical stage of the cognitive impairment. The low sample size would also affect the generalizability of the study hence the present study should be interpreted with caution.
Implications for Practice
The outcome of this study has shown that efforts should be made to ensure that caregivers of stroke patients are adequately prepared to give the care to ameliorate the negative impacts of caregiving on the health of caregivers of stroke patients with cognitive impairment. Also, psychological support such as support groups or psychotherapy for caregivers will go a long way in improving and stabilizing their psychological health. There is a need to ensure that the welfare of the caregivers is well taken care of by the family of the person receiving care. The service providers need to identify caregivers at risk of greater strain and to help caregivers work through situations that services cannot alter. The target of caregiver interventions should be tailored to reduce the negative effect of caregivers’ stress. Also, some interventions should be directed to increase the caregivers’ knowledge of resources and appropriate care techniques such as providing education about the availability of local services and education on how to bathe an uncooperative care receiver. Something that should not be overlooked while providing caregivers emotional support (listening, giving advice, and reassuring them) in an individual or group counseling session is to focus on increasing problem-solving strategies and support-seeking behaviors for the caregiver.
Conclusion
The outcome of this study shows that the physical health domain of quality of life, the social relationship and the environmental health were slightly moderate, the psychological health was low, and the burden of caregivers was high. This implies that the quality of life of the caregivers of stroke survivors with cognitive impairment was moderate, and the caregivers’ stress was high in the sample studied.
Footnotes
Acknowledgements
We are grateful to the families of patients who allowed us access to the caregivers of their loved ones, and the caregivers who served as respondents.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Before commencement of data collection, the study was approved by the Ethics Committee of the Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Nnewi Campus, Anambra State, Nigeria, by the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from the participants before data collection.
Data Availability
The dataset used and/or analyzed during the current study is available from the corresponding author upon reasonable request.