
Abstract
Keywords
Introduction
Several studies have shown associations between inadequate nocturnal sleep and negative health factors (Foley et al., 2004; Goldman et al., 2007). In fact, repetitive sleep deprivation (<6 hours/day) is associated with endocrine and immune dysregulations and cognitive decline (Tumiran et al., 2018), which increase the prevalence of chronic diseases such as diabetes (Tan et al., 2018), metabolic syndrome (Tan et al., 2018), obesity (Tan et al., 2019), osteoporosis (Yi et al., 2018), heart disease (Foley et al., 2004), neurodegenerative diseases (Wei et al., 2019), and even mortality (Stone et al., 2009).
Physical fitness is closely associated with one’s health status (Fu et al., 2017). A high level of physical fitness is related to the prevention of most of the mentioned chronic diseases and organic deterioration (Anderson & Durstine, 2019; Pedrero-Chamizo et al., 2012). It is important to note that physical fitness levels show sex and age specific differences in older adults (Pedrero-Chamizo et al., 2012). Research has suggested a bidirectional relationship between exercise and sleep (Kline, 2014). However, aging is associated with impairments in sleep patterns (Hargens et al., 2013), and therefore the benefits of regular physical activity on sleep in the elderly have been extensively studied (Moreno-Vecino et al., 2017; Vanderlinden et al., 2020). A recent systematic review concluded that moderate physical activity programs improved sleep variables in the elderly (Vanderlinden et al., 2020). Adults with sleep problems score lower in physical fitness and higher in physical frailty (Nakakubo et al., 2018), but there are still aspects regarding the association between sleep problems and body shape index that should be determined as for example short or long time sleeping (Moreno-Vecino et al., 2017). Older adults with sleep disruption demonstrate a high prevalence of risk factors associated with poor body composition (Tan et al., 2019), and too short or too long nocturnal sleep could be linked with greater adiposity in the middle-age and elderly (Theorell-Haglöw et al., 2014). A study has shown that lower nocturnal sleep time could be associated with greater body mass index (BMI), waist circumference (Faraone et al., 2021), and fat mass among Chinese males (Chen, Zhang et al., 2019). Furthermore, it is important to notice that both sexes sleep different (Mong & Cusmano, 2016). One of the main reasons is the role of sex steroids in sleep modulation in which females described poor quality and more disorders (Mong & Cusmano, 2016).
Diurnal sleep (also called nap) rarely is considered in total sleep time and efficiency, despite it is a noteworthy addition to daily sleep duration. In older adults, light and fragmented sleep during nocturnal sleep could lead to increased daytime somnolence, which also leads to longer daytime naps (Tan et al., 2018). A brief nap (<30 minutes) is considered as the optimal duration to promote the recuperative effects of napping in healthy people (Hilditch et al., 2017). It is not if producing sleep inertia and has a few minutes of slow-wave sleep, which is the most restful sleep phase (Tumiran et al., 2018). In healthy people, short naps improve cognitive performance, alertness, and mood (Tumiran et al., 2018); whereas long naps induce somnolence and impair cognitive abilities (Mantua & Simonelli, 2019), and could be a risk for hypertension (Cheungpasitporn et al., 2016). Naps could be a symptom of diurnal somnolence, especially in older people, which is related to cognitive degeneration, drug intake, obesity, and sleep impairment. People with sleep deprivation or sleep impairment could replace their sleep loss with diurnal naps. A study observed that napping could be protective against chronic diseases in older females (Stone et al., 2009). Nevertheless, scientific evidence of the long-term effect of napping is controversial (Lopez-Minguez et al., 2017) and it could be associated with obesity (Patel et al., 2006), fatigue, immune system (Faraut et al., 2011), and sleep wake-cycles (Endo et al., 1981). The effect of napping, where it is a rooted habit, remains unknown in Mediterranean, Asian, or Islamic countries (Tumiran et al., 2018).
Therefore, the aim of this study was to determine the associations of nocturnal sleep and nap time with physical fitness and body composition among older adults.
Methodology
Study Setting and Sample
This research is a cross-sectional study conducted in the framework of the EXERNET-Elder 3.0 project, whose protocol has been published elsewhere (Gomez-Bruton et al., 2020). EXERNET-Elder project is a multi-center study executed between 2008 and 2009 (baseline data) and 2016 and 2017 (follow-up) in Spain in older adults aged over 65 years old. Data collection was performed in sports centers or centers for the elderly where participants were used to attend. Participants were contacted by phone and once the study began. For the purpose of this study, we obtained data from the follow-up.
Inclusion criterion was being over 65 years. Exclusion criteria for bioimpedance analysis were to wear a peacemaker and/or a metal prosthesis, and people suffering from cancer or dementia. For physical fitness tests, exclusion criteria were any medical advice against doing physical activity due to disease, recent heart failure, blood pressure over 180/100, and joint or chest pain when doing physical activity.
From an initial total sample of 3,093 participants in 2008, 236 deaths were noticed between 2008 and 2016, leaving a total of 2,857. Furthermore, one center could not perform the follow-up due to lack of funding and, the sample was reduced by 400 participants, moving to 2,457 eligible older adults. 1,055 participants were also not able to attend the follow-up (i.e., change of residence or city, did not answer the phone, became dependent and could not attend the follow-up or was not willing to undertake the evaluation). Therefore, 1,402 participants finalized all the evaluations. Sleep questionnaire was added in 2016 to 2017, and to be included in this research, only 830 participants completed sleep questionnaire, body composition, and physical fitness assessments. The protocol was approved by the Ethics Committee of Clinical Research of the Alcorcón Foundation University Hospital (16/50), Spain.
The protocol followed the ethical guidelines of the Declaration of Helsinki 1964, revised in Fortaleza (2013) by the World Medical Association, complying with the Spanish legislation and legal regulations for clinical research in humans (Law 14/2007 on biomedical research). Written informed consent was obtained from each participant.
Demographic Data
Demographic data were obtained on all participants through an interview conducted by junior researchers using a validated questionnaire (Lopez-Rodriguez et al., 2017). A question regarding organized physical activity was included: Are you currently engaged in organized physical activity? Organized physical activity refers to a collective guided and supervised activity that is developed by an instructor. Units were hours per week.
Sleep Assessments
Sleep patterns were assessed using the Jenkins Sleep Scale (Jenkins et al., 1988). The questions used for this study were: (1) How many hours do you sleep at night daily? (2) How many hours do you sleep or nap daily? Both questions quantify nap and nocturnal sleep duration and were answered in hours and minutes, respectively.
Nocturnal sleep was divided into three groups: <7, 7 to 9, and >9 hours (U.S. Department of Health & Human Services (HHS) (2016)). Nap time was categorized as: No nap, 1 to 30 minutes, and >30 minutes groups following the criteria used previously by Leng et al. (2019). Total daily sleep was also created as the sum of nocturnal sleep and nap time as a continuous variable.
Physical Fitness
Physical fitness was evaluated by trained researchers through a Senior Fitness Battery (Rikli, 2001), and some test modified from Eurofit Testing Battery (Eurofit, 2003), which has been described in detail and for which reference values for the Spanish population have previously given (Pedrero-Chamizo et al., 2012). Aerobic capacity, upper and lower body strength, maximum handgrip strength, static balance, agility/dynamic balance, and gait speed were tested using both batteries.
The results of each test were stratified by sex. Quartiles were calculated assigning punctuation between 1 and 4 for each test, 4 being the highest level. The sum of all punctuations was divided by the number of tests giving a physical fitness index for each participant.
Body Composition
Anthropometric measurements included weight and fat mass, which were measured using an electric bioimpedance (Tanita BC-418MA, Corp., Tokyo, Japan). For all participants, 0.6 kg were subtracted for the total weight to correct for clothes weight. Participants also removed all the metallic objects and went up to the Tanita without footwear.
Height was measured with a stadiometer (Seca, Hamburg, Germany) and was adjusted using an estimation proposed by Chumlea et al. (1985) after measurement as height is usually shorter in older adults because of the minor inter-vertebral distance. Furthermore, BMI was calculated using the formula BMI = Weight (kg)/Squared Height (m2) (Chumlea et al., 1985).
Waist and hip circumference were assessed with a metal non-elastic metric band. Waist circumference was conducted in the anthropometric position. The measure was made in the thinnest region between the last rib and the iliac crest without clothes. Body shape index (waist circumference (m)/BMI (kg/m2)⅔ × Height (m)½), and waist to height ratio (waist circumference (m)/Height (m)) were then calculated.
Data Analysis
Baseline characteristics are presented as mean ± standard deviation (SD) for continuous variables and frequency (%) for categorical variables. A Kolmogorov-Smirnov test was done to check the data normality. Differences between sex groups were assessed using an independent sample t-test for continuous variables, and chi-squared test for categorical variables. All statistical models were divided by sex because both groups were not homogeneous regarding physical fitness, body composition, nap, and nocturnal sleep duration. Comparisons were done using Bonferroni or T2 Tamhane post hoc analysis between nocturnal sleep and nap groups with body composition and physical fitness. The Levene test was done to check the homogeneity of the variances (p < .05). Odds ratios (OR) and 95% confidence interval were calculated by multinomial regression models with nocturnal sleep groups (<7, 7–9, and >9 hours) and nap groups (no nap, 1–30 minutes, and >30 minutes) as dependent variables, and physical fitness and body composition as independent variables. Nocturnal sleep 7 to 9 hours and no nap groups were the reference groups in all the models. Each model was adjusted for the age, BMI (except for BMI model), physical fitness index (except for physical fitness index model), and nocturnal sleep time. Significant difference was set considered at p < .05. All tests were conducted with SPSS for Windows, Version 25.0. Armonk, NY: IBM Corp.
Results
Descriptive Characteristics
Table 1 shows the 830 participants’ characteristics of this study. Participants were 75.1% female with a mean age of 77.7 ± 5.1 years. Females presented less nocturnal sleep, nap, physical fitness (except for flexibility), but had higher BMI, and fat mass (p < .05) than males. Among 623 females, 51.0% and 54.0% slept below 7 hours and did not take a nap, respectively. In males, only 32.0% had nocturnal sleep below 7 hours and 30.4% did not nap during the day.
Descriptive Characteristics Split by Sex.

Note. Independent sample t-test for continuous and chi-squared test for categorical variables. Significant differences are in bold (p < .05). SD = standard deviation.
Differences in Physical Fitness and Body Composition According to Nocturnal Sleep and Nap Time Groups (Tables 2 and 3)
Physical Fitness and Body Composition Values by Sex, and Stratified by Nocturnal Sleep Time Groups.
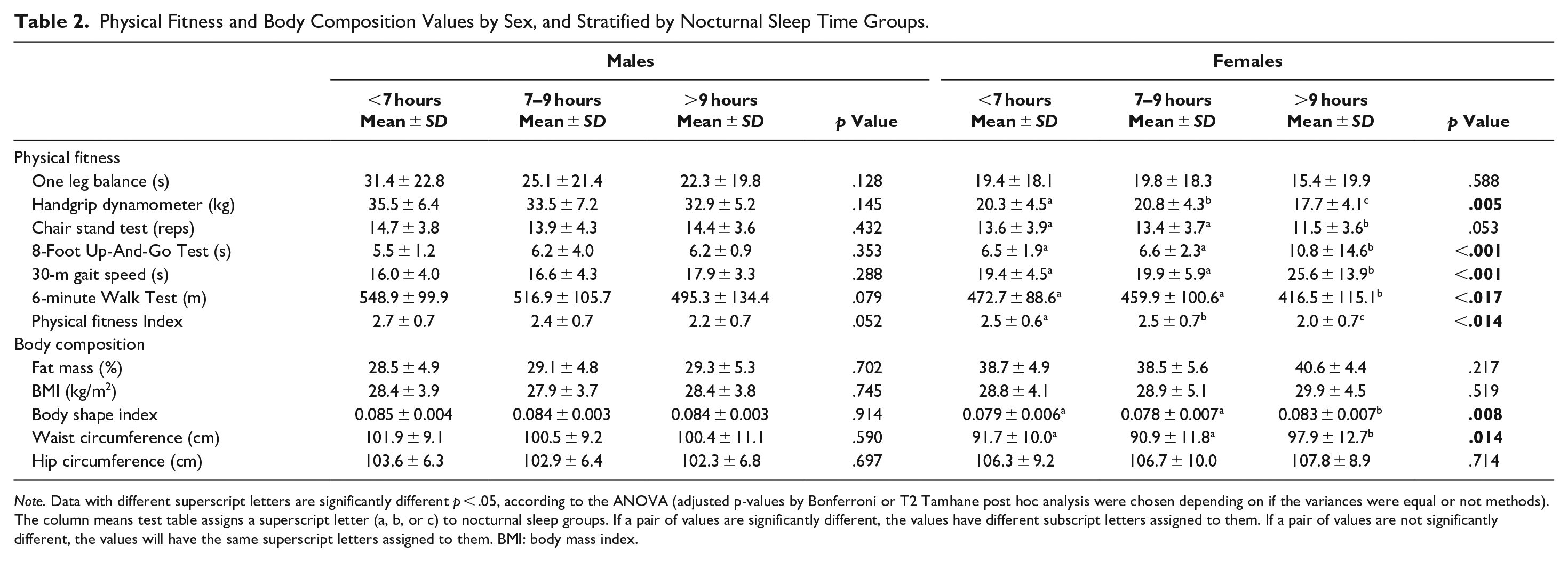
Note. Data with different superscript letters are significantly different p < .05, according to the ANOVA (adjusted p-values by Bonferroni or T2 Tamhane post hoc analysis were chosen depending on if the variances were equal or not methods). The column means test table assigns a superscript letter (a, b, or c) to nocturnal sleep groups. If a pair of values are significantly different, the values have different subscript letters assigned to them. If a pair of values are not significantly different, the values will have the same superscript letters assigned to them. BMI: body mass index.
Physical Fitness and Body CompoSition Values by Sex.Stratified by Nap.

Note. Data with different superscript letters are significantly different p < .05 (in bold), according to the ANOVA (adjust p-values by Bonferroni or T2 Tamhane post hoc analysis were chosen depending on if the variances were equal or not methods). The column means test table assigns a superscript letter (a, b, or c) to nap groups. If a pair of values is significantly different, the values have different subscript letters assigned to them. If a pair of values are not significantly different, the values will have the same superscript letters assigned to them. BMI = body mass index.
Males: There were no significant differences between nocturnal sleep groups nor in physical fitness neither in body composition. There were significant differences among the three nap groups in all physical fitness tests (except for handgrip and balance), having nap groups higher scores than the no nap group (p < .05). Furthermore, males who took a nap >30 minutes showed higher waist circumference than the other groups (p < .05).
Females: Significant differences were found between nocturnal sleep and all physical fitness tests (except for balance and chair stand test) (p < .05). Females who slept <7 hours presented higher physical fitness scores than the other groups (except for handgrip). Regarding body composition, higher waist circumference and body shape index were observed in females who slept >9 hours (p < .05) compared to those who slept <7 hours and between 7 and 9 hours. Those in the no nap group had significantly higher scores for the chair stand test (p < .05).
Association between sleep patterns, physical fitness and body composition
Males: For the nap time groups, waist and hip circumference were significantly related to nap duration between 1 and 30 minutes, OR = 1.08 (1.02 and 1.16, p = .009) and OR = 1.08 (1.00–1.17, p = .048), respectively (Table 4).
(a) Association of Nocturnal Sleep Groups on Physical Fitness and Body Composition in Males.

Note. Each model was adjusted for age, BMI (except for BMI model), Physical fitness Index (except for physical fitness index model), and nocturnal sleep time. Significant associations are in bold (p < .05). CI = confidence interval; BMI = body mass index.
Females: The >9 hours nocturnal sleep group was significantly associated with body shape index and waist circumference, OR = 4.07 (2.87–5.76, p = .011) and OR = 1.04 (1.00–1.08, p = .024), respectively. A nap time >30 minutes was associated with higher fat mass and body shape index, OR = 1.22 (1.01–1.46, p = .032) and OR = 3.95 (1.82–8.38, p = .027), respectively (Table 5).
(b) Association of nocturnal sleep groups on physical fitness and body composition in females.

Note. CI = confidence interval; BMI = body mass index. Each model was adjusted for age, BMI (except for BMI model), physical fitness index (except for physical fitness index model), and nocturnal sleep time. Significant associations are in bold (p < .05).
(a) Association of nap groups on physical fitness and body composition in males.

Note. Each model was adjusted for age, BMI (except for BMI model), physical fitness index (except for physical fitness index model), and nocturnal sleep time. Significant associations are in bold (p < .05). CI = confidence interval; BMI = body mass index.
(b) Association of nap groups on physical fitness and body composition in females.

Note. Each model was adjusted for age, BMI (except for BMI model), physical fitness index (except for physical fitness index model), and nocturnal sleep time. Significant associations are in bold (p < .05). CI = confidence interval; BMI = body mass index.
Discussion
A cross-sectional study was conducted to analyze the association between nocturnal sleep and nap time with physical fitness and body composition among a population of Spanish community-dwelling older adults. In our sample, higher nocturnal sleep was related to poor body composition outcomes in females. Nap time >30 minutes was associated with greater risk for high fat mass and body shape index in females, whereas naps during <30 minutes were associated with higher waist and hip circumference in males. Our results suggested that body composition and physical fitness were associated with sleep patterns in different ways. In multinomial regression models, the nap groups showed an association with some body composition outcomes in both sexes; however, no significant connections were found between physical fitness with nocturnal sleep and nap groups.
The dissimilar results with nocturnal sleep and nap time with physical fitness and body composition in each sex may be partially explained due to females tend to sleep less than males and could happen because of biological, social, and/or physiologic factors (Burgard & Ailshire, 2013; Jung et al., 2013). According to Kim et al. (2021), females slept more than they reported, or they had better sleep quality (Kim et al., 2021).
On the one hand, the group-based differences in the physical fitness scores were also similar in those found in previous research (Pedrero-Chamizo et al., 2012), showing higher physical fitness levels in males than females (Bibiloni et al., 2018). Females who got <7 hours nocturnal sleep also reported significantly better results in all physical fitness tests (except for handgrip) compared to the other female groups. A good physical fitness is essential to reduce risk of falls and promote functionality, but also is associated with less risk of suffering from non-communicable chronic diseases and early mortality in the elderly (Yerrakalva et al., 2015). Nevertheless, it could be appreciated that physical fitness did not present a significant association with either nocturnal sleep or nap groups in both sexes. In this sense, results could be different if objective methodologies to measure sleep time will be used in this study.
Regarding the prevalence, the prevalence of high BMI and percentage of fat mass was consistently higher in females in most studies (Kim et al., 2016; Valentine et al., 2009; Vogel et al., 1986; Wray & Blaum, 2001). Moreno-Vecino et al. found females with sleep disturbance presented higher BMI and waist circumference (Moreno-Vecino et al., 2017). In our study, females who slept >9 hours during the night had higher waist circumference and body shape index. Sleep duration is associated with hormonal disruption, diurnal somnolence, and increased sedentary time, which increases the risk of developing chronic diseases such as type 2 diabetes or obesity by different mechanisms (Patel et al., 2008; Vgontzas et al., 2008). Furthermore, diurnal somnolence is associated with an increased risk of obesity in elderly adults (Beccuti & Pannain, 2011), while Chen et al. (2019) found that napping is associated with being overweight (Chen, Zhang et al., 2019). Concretely, they found that poor nocturnal sleep time was associated with greater BMI, waist circumference, and fat mass in Chinese older males (Chen, Zhang et al., 2019).
Our data also indicated that napping was also more frequent in males than females (37.4 ± 41.5 vs. 18.7 ± 31.5 minutes). These findings agree with previous studies (Guidozzi, 2015; Jung et al., 2013). Nonetheless, other studies have reported negative association between long naps and functional capacity and independency in older adults (Guarnieri Ribeiro Bueno et al., 2019; Jung et al., 2013) as it is directly affected by the physical fitness. The acute effects of moderate length naps are undeniably beneficial for cognitive performance and could be a remedy to compensate impairments in nocturnal sleep, even for an older population (Qian et al., 2020). However, naps, especially long naps, are associated with diurnal somnolence, thus longer naps could cause health issues and age-related body and brain degeneration which could lead to less physical performance and worse body composition (Mantua & Simonelli, 2019).
This study presents some limitations. The major limitations are a) sleep habits were self-reported, and we could not use actigraphy, which is a gold standard. Nevertheless, sleep self-reported questionnaires are widely used in clinical area. Further, medications have not considered as covariates. Nevertheless, it would be included in future investigations. We checked medical questions and only seven participants referred obstructive sleep apnea, thus, it was not significant over the total sample. On the other hand, the sample was divided in groups (regarding nap or nocturnal sleep) and these groups were not homogeneous. This could lead to greater variances and to more conservative results. Moreover, it is a cross-sectional study, limiting our conclusions about the causal effect of nocturnal sleep and nap time on physical fitness and body composition. Nevertheless, this study has several strengths. EXERNET cohort is part of a representative sample of the Spanish territory with a large sample size. Furthermore, outcomes were evaluated using objective measurements and validated questionnaires.
Moreover, next steps should be done in geriatric and institutionalized context. For example, healthy habits as performing daily physical activity, eating adequately, and avoiding sleep disorders are essential to keep a good quality of life.
Conclusions
This cross-sectional study reveals differences between sleep patterns, body composition and sex taking into consideration that sleep patterns have been analyzed by subjective methods. However, no connections were found between physical fitness with nocturnal sleep and nap groups. Concretely, long nocturnal sleep and nap time were related to a higher value of fat mass and body shape index in females. In males, brief nap times were associated with higher waist circumference and hip values. Further research could examine the longitudinal effects of these sleeping habits in older adults to applied specific interventions.
Footnotes
Acknowledgements
The authors are grateful to all collaborators: the nursing homes, health centers, and participants whose cooperation and dedication made this study possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by “Ministerio de Economía, Industria y Competitividad” (DEP2016–78309-R), “Centro Universitario de la Defensa de Zaragoza” (UZCUD2017-BIO-01), Zaragoza City Council, the Biomedical Research Networking Center on Frailty and Healthy Aging (CIBERFES), and the official funding agency for biomedical research of the Spanish government, Institute of Health Carlos III (ISCIII), which is co-funded by the European Regional Development Fund (CIBEROBN CB12/03/30038).
Ethical Statement
The protocol was approved by the Ethics Committee of Clinical Research of the Alcorcón Foundation University Hospital (16/50), Spain.