
Abstract
Early evidence of remote, volunteer-led social support interventions to reduce social isolation in older adults has been encouraging; however, evaluation data on outcomes related to social isolation associated from these interventions is scarce. Here, we share programmatic details of a novel, statewide initiative, called the NEST Collaborative, rolled out to meet immediate emotional, informational, and instrumental needs of older adults in Nevada during the COVID-19 pandemic. The evaluation included 31 older adults participating in weekly one-to-one empathy-based phone calls with multi-generational volunteers seeking to enhance participants’ social networks through meaningful friendships. The calls were associated with programmatically meaningful, though not statistically significant, improvements in modified Hawthorne Friendship Scale and PHQ-2 Depression Scale scores over two waves of survey responses. These results suggest that social isolation and depression among older adults decreased among our sample over a period of increased isolation and mental health burden across the general population. With the potential for sustained impact in reducing social isolation over time, remote social support programs, such as the NEST Collaborative, may have persistent value long-term, beyond time-limited crisis response contexts.
Keywords
● A description of a statewide, remote, social support program for older adults in Nevada, with potential for replication by community elder service agencies nationwide. ● A quantitative assessment of a remote social support intervention on validated measures of depression (PHQ-2) and social isolation (Hawthorne Friendship Scale).
● Remote social support programs have potential to improve outcomes associated with social isolation among older adults and may be a viable alternative to in-person social support. ● Remote social support programs should be expanded given the need even beyond the COVID-19 emergency context in which this evaluation was performed. ● Funding for statewide remote social support programs should allow for services to extend beyond state lines given the transmissability of remote social support delivery. ● Although the social support intervention evaluated in this work was implemented through a state aging agency, remote social support programs could potentially be a cost-effective addition to health care system population health management strategies to reduce the burden of health conditions associated with social isolation.
Introduction
Social isolation (i.e., the absence of social interactions, contacts, and relationships), an objective and quantifiable construct, can reduce well-being. The mechanism can be both direct and indirect, mediated by the construct of loneliness (i.e., the subjective perception of social isolation) (Banerjee & Rai, 2020; Beller & Wagner, 2018; Golden et al., 2009). Together, social isolation and loneliness are closely linked to a myriad of medical and mental health conditions (including depression and anxiety), and have long been understood to contribute to premature mortality, especially among older adults (Berkman & Syme, 1979; Blazer, 1982; Fan et al., 2021; Hakulinen et al., 2018; National Academies of Sciences, Engineering, and Medicine et al., 2020). In the US, prior to the COVID-19 pandemic, approximately 24% of community-dwelling older adults experienced social isolation (Donovan & Blazer, 2020). The high prevalence of social isolation, and its negative impacts on health, motivate the development and evaluation of social support interventions.
The literature identifies four distinct elements of social support: emotional (expressions of empathy, caring, etc.), instrumental (tangible aid), evaluative (information useful for self-appraisal), and informative (advice, suggestions, etc.) (Cobo-Rendón et al., 2020). Social support is often provided by those within one’s social support network, which includes other individuals, groups, and the community in which a person has relationships or affiliation (Ozbay, 2007). Social support interventions for older adults often create opportunities for participation in peer groups, such as community group activities (i.e., clubs), which may form the basis of social support networks (Chiao et al., 2011; Zaitsu et al., 2018). Another form of social support intervention include organized peer and multigenerational social visits (Winningham & Pike, 2007). These programs are based on the idea that as individuals develop meaningful relationships through social visits and as their social support network grows, they will have greater access to the elements of social support described above, and social isolation will decrease.
The literature discusses two pathways in which social-visit interventions might exert their intended effect on social isolation. First, regular social interactions can diminish the absence of relationships, which defines social isolation (Chen & Schulz, 2016; Gardiner et al., 2018). Second, increased emotional and informative social support can reduce loneliness, the subjective experience of social isolation, and thus decrease social isolation itself (Chen & Schulz, 2016; Gardiner et al., 2018).
Empirical studies support the hypothesis that social support provided through repeated social visits can reduce social isolation (Kharicha et al., 2018; Kremers et al., 2006; Winningham & Pike, 2007). A one-to-one, in-person volunteer befriending program in the U.K. showed that older adults participating in the program looked forward to the visits and that these visits reduced loneliness (Butler, 2006). Reinke et al. (1981), explored the effects of in-person casual conversation with older adults and found improved morale (measured via the Life Satisfaction Index and self-perceived health) and sociability (as rated by the nursing home employees). Cohen-Mansfield et al. (2007) discovered that in-person shared interest groups, which revolved around cordial conversation about a topic of interest (such as music), reduced measures of loneliness. While this evidence has been encouraging, these social support programs require in-person interactions, whereas social distancing practices required by COVID-19 paused participation in these types of programs. Thus, remote social support opportunities emerged nationwide, with little documented evidence regarding their potential impact.
Following on established successes of in-person social support programs (Cohen-Mansfield et al., 2007; Kharicha et al., 2018; Kremers et al., 2006; Reinke et al., 1981; Winningham & Pike, 2007), the NEST Collaborative, a statewide service that is part of a larger initiative known as the Nevada COVID-19 Aging Network Rapid Response (Nevada CAN), devised a program to deliver remote social support to older adults. As with in-person social support programs, the NEST Collaborative emphasized creation of meaningful, ongoing friendships through which older adults would have increased access to emotional, informational, and (for some) instrumental support. The NEST Collaborative initiated the use of multi-generational volunteers to deliver social support via weekly empathy-based phone conversations throughout the COVID-19 pandemic, with continued service delivery ongoing to date.
The NEST Collaborative identified ongoing one-to-one phone conversations as a potentially meaningful and viable form of social support for several reasons. First, its remote and socially-distant nature meant that no risk of virus exposure was involved. Second, prior research has shown that in order to benefit from social support, the older adult must play an active role in the intervention, which, in this case, is achieved through a one-on-one conversation (Chiao et al., 2011). Third, research has demonstrated higher efficacy of long-term (i.e., more than 6 months) empathy-based conversation interventions on outcomes related to social isolation (Chiao et al., 2011). Fourth, choosing a phone-based rather than a video-based intervention was intended to maximize accessibility for older adults, since video-based technology can be less user friendly and can introduce access disparities in remote areas without adequate bandwidth (Gorenko et al., 2021).
Early evidence that social support can reduce social isolation and related harms, when delivered remotely, is encouraging (Dassieu & Sourial, 2021). One study evaluated a 6-month, computer-driven, peer-based social support program administered to 150 older adults. It found that participants in the intervention group reported significantly less loneliness and increased perceived social support, compared to the comparison group (Czaja et al., 2018). Notably, while the perception of social support (i.e., the subjective belief that one’s social network of friends and family will provide the four elements of social support) and actual social support, are not necessarily correlated (Eagle et al., 2019), Czaja et al. (2021) found the perception of social support to be associated with reduced depression, an outcome of interest to the present evaluation.
More recently, in response to the COVID-19 pandemic, a randomized trial by Kahlon et al. (2021) investigated the effects of empathy-based telephone calls delivered by volunteers. Kahlon defines “empathy-oriented” as “prioritizing listening and eliciting conversation from the participant on topics of their choice.” The study found that measures of loneliness, depression, and anxiety were significantly improved in individuals receiving the intervention compared to a control. This intense intervention involved daily calls for the first 5 days, and then two or more calls per week for 1 month (Kahlon et al., 2021). This study shows the value of empathy-based telephone calls on harms related to social isolation. However, it leaves unanswered how a longer but less intensive program delivery (i.e., occurring over more months but with fewer calls per week) could benefit older adults.
Our aims are two-fold: (1) Describe key components of a remote, multi-generational, volunteer-led social support intervention for older adults, implemented to address the immediate needs of this population during implementation of Nevada’s COVID-19 stay-at-home order; (2) Examine whether levels of social isolation, depression, and anxiety decreased among older adults receiving one-to-one, empathy-based social calls through two waves of a telephone survey including two psychometrically-validated scales, with data collected as part of a pragmatic evaluation of the NEST Collaborative.
Program Description: Nevada CAN and The NEST Collaborative
The TIDieR guidelines, a checklist for a standardized description of interventions, were used in the summary that follows (2014). The NEST Collaborative is an initiative of the Nevada CAN Rapid Response, established in March of 2020. The Nevada Aging and Disability Service Division (ADSD) created a partnership with the Sanford Center for Aging, along with the Dementia Engagement, Education, and Research (DEER) Program, and Nevada Senior Services to launch Nevada CAN. Nevada CAN sought to maximize coordination of service delivery, including delivery of food and medications, telehealth services, and as emphasized in this report, social support for (suddenly) homebound older adults during the COVID-19 pandemic.
The NEST Collaborative, the social support component of Nevada CAN, led by the University of Nevada, Reno DEER Program, consisted of more than 30 aging and social service organizations and was led by an advisory team tasked with providing guidance on program design and implementation. The NEST Collaborative Advisory Team was primarily composed of representatives from partner organizations (n = 18), but also included NEST Collaborative volunteers (n = 7), administrative program staff (n = 5), and program participants (n = 3).
The NEST Collaborative social support social call program was designed to reduce social isolation, in the hopes of also reducing loneliness, depression, and anxiety. The social call program, offered in English, Spanish and other languages based on volunteer availability, facilitated regular one-to-one telephone calls to assigned older adult participants by volunteers. The NEST Collaborative differed from other remote, volunteer-led social support intervention programs through the use of one-to-one phone calls (rather than social media groups, video chat groups, or hybrid approaches, multi-generational volunteers rather than peers, and through weekly or twice weekly rather than more frequent interactions). The frequency of the phone calls, once or twice per week, was chosen by each participant. The vast majority of participants opted for calls once per week.
The NEST Collaborative’s one-to-one calls served as an opportunity for social interaction between older adult participants and volunteers, while avoiding the risk of exposure to the COVID-19 virus. In making these social calls, the volunteer’s role was to have phone conversations intended to help the older adult feel comfortable and supported. The NEST Collaborative’s intention was that, over time, these interactions would form the basis for meaningful friendships between the older adult and volunteer, adding a new node to the older adult’s social network. This intervention was tailored to be casual, friendly, and, using the approach of a similar intervention described in the literature, empathy-based (Kahlon et al., 2021). The empathy-based nature of the intervention was critical to the ability of its volunteers to provide emotional and informational social support to the older adult participants.
Empathy-based conversations were guided by principals including active listening, respect for people’s opinions, and an emphasis on authenticity. The conversations were peppered with “getting to know you” questions about values, important likes and preferences, and memories. The conversations also included opportunities for both conversation partners to share things that are important to them. Some commonly-reported conversation topics were descriptions of day-to-day activities, stressors, major life changes, interests and hobbies, and the importance of friendship. Through these conversations, emotional and information social support needs were addressed.
In preparation for delivering this intervention, volunteers were trained through the NEST Collaborative’s intensive 9-hour volunteer training series, to connect on a personal level with their older adult participants. The remote training consisted of two parts. Part 1 was self-directed and led the volunteer through a series of webinar topics such as effective communication with older adults, cultural competency, suicide prevention, elder abuse awareness and reporting, as well as, perhaps most importantly, how to conduct an empathy-based conversations. Excerpts from the Volunteer Handbook about empathy-based conversations are included in Supplemental Web Appendix C. Part 1 included interspersed knowledge quizzes to encourage active participation. Part 2, facilitated live on Zoom by NEST Collaborative staff, involved a moderated discussion with volunteers-in-training. The discussions used role play scenarios to drive conversations about model interactions and ways to handle a variety of challenges that can arise during the social calls, ranging from awkward pauses in conversation to older adults expressing despair. This part of training further emphasized empathy-based conversations and provided volunteers with practical examples of how to engage in such conversations.
Additional support was provided to the volunteers through assigned Volunteer Guides, who were experienced aging services professionals serving as program volunteers. Volunteer Guides were assigned to a small group (approximately 3–8) of volunteers. These Guides led ongoing, weekly, Zoom-based meetings, called “huddles,” where volunteers shared successful conversation strategies and solutions for challenges in creating relationships with the older adult participant. The Volunteer Guides provided advice and support to volunteers throughout the duration of the program.
While it was not the primary purpose of the calls, the calls also served as a way to identify any unmet needs (e.g., financial, medical) of the older adult (hereafter referred to as “participant”). Volunteers were not tasked with directly checking in on these needs, however, if the older adult brought them up, volunteers were instructed to ask the participants if they would like assistance connecting to support, with a referral to Nevada 211 or specific services within Nevada CAN. If the participant agreed, the volunteer would then contact the NEST Collaborative Support Team, who would then make the referral to the appropriate services, including, among other resources, the Nevada Aging and Disability Resource Centers. This component of the program addressed instrumental social support.
Volunteer recruitment targeted students attending the University of Nevada, Reno, the University of Nevada, Las Vegas, as well as existing workers and volunteers at Nevada Social Services. Volunteers were eligible to serve if they were 18 years old or older, underwent a background check, and participated in the volunteer training described above. The age range of volunteers (n = 34) spanned from 18 to 70 years old, though a majority of volunteers were traditional college age. Volunteer education level ranged from those pursuing a bachelor’s degree, to those who have a graduate or professional degree. Due to recruitment and outreach efforts being focused to the aforementioned institutions and programs, all volunteers resided in the state of Nevada at their time of program participation.
Participants were referred to the program through word-of-mouth, often by NEST Collaborative partner organizations, as well as through an online referral and triage system established by Nevada CAN. Most participants lived independently in private homes, while a small minority lived in assisted living communities.
Methods
Data Collection
A trained data collector conducted phone surveys using Qualtrics online software between September 2020 and February 2021. Data collection training emphasized speaking slowly and clearly, as well as repeating questions or responses as needed, in preparation for administering a phone survey, and in case participants experienced hearing loss. Consent was verbally requested for each phone call, and the study was determined to be exempt by the University of Nevada, Reno institutional review board.
All NEST Collaborative participants (n = 152) were eligible to complete the survey if they had received at least one one-to-one social call from a volunteer. This criterion ensured that survey responses reflect participants’ experiences after beginning the program. Participants were asked to complete the survey twice (Wave 1, Wave 2), with 3 months between Wave 1 and Wave 2. A total of 31 participants completed Wave 1 and 17 completed Wave 2. Surveyed individuals were read a consent letter indicating that the survey was voluntary and that NEST Collaborative participants who declined to respond were able to continue the program.
We noted how long each participant had been a program participant when they completed the Wave 1 and Wave 2 survey, as there was some variation. Participants who had received calls for 3 months or less at Wave 1 were identified as “short-term” and participants who had received calls for 4 to 6 months (the maximum) at Wave 1 were identified as “long-term.”
Demographics
The survey gathered basic demographic characteristics (age, location, race/ethnicity), other relevant demographic information (e.g., veteran status, driving status, place of residency), and information about pre-COVID-19 socializing and mobility. Place of residency was included because while most participants lived in private homes, some lived in assisted living communities. A subset of time-variant questions were repeated during the second survey.
Modified PHQ-2
The 2-item PHQ-2 scale is a validated screening tool for depressive symptoms (Cronbach α = .767) (Levis et al., 2020). This scale can be used to indicate further screening for depression via the more thorough PHQ-9 (Levis, 2020). The PHQ-2 was answered on a five-point Likert type scale, with never (1) and almost always (5) as the endpoints (Levis, 2020; Löwe et al., 2005). To reduce response burden among participants, this evaluation used a modified version of the PHQ-2 Depression Scale (PHQ-2) (Brosnan et al., 2021). These answer choices were modified to align with the phrasing of the Hawthorne Friendship Scale (HFS) answer choices (see Supplemental Web Appendix A). High scores suggest a higher likelihood the respondent has clinical depression, and low scores suggest a lower likelihood of clinical depression.
Modified Hawthorne Friendship Scale
The Hawthorne Friendship Scale has been validated to measure social isolation in older adults (CFI = 0.99, RMSEA = 0.02, Cronbach’s α = .83) (Hawthorne, 2006). The HFS was answered on a five-point Likert type scale, from never (5) to almost always (1). A modified version of the HFS, which excluded a question unlikely to be impacted by the one-on-one intervention, was used (Hawthorne, 2006; Hawthorne & Griffith, 2008) (see Supplemental Web Appendix A). Question 2 (regarding feelings of isolation) was reverse scored to make high scores consistently indicative of more loneliness and low scores consistently indicative of less loneliness.
Stress Level and Post-COVID-19 Social Outings
In addition, single-item questions gauged stress due to COVID-19 and number of social outings a week. These questions were: “Over the last two weeks, how often have changes brought about by COVID-19 caused you to feel stressed or anxious?” and “Over the last two weeks, how many times have you left your house for a social outing to visit friends or family in their homes or engage in social recreational activities?” Possible responses ranged from never (1) to almost always (5).
Satisfaction With Volunteers and Conversation Topics
Questions about participants’ satisfaction with their volunteer were also included. Participants were asked about their satisfaction regarding the frequency of calls, length of calls, how well their volunteer listens, and their overall satisfaction with their volunteer. Answer choices ranged from extremely unsatisfied (1) to extremely satisfied (5).
Participant Growth and Retention
In addition to the survey data collected, participant retention was tracked between May 2020 and July 2021. The NEST Collaborative’s internal data from participant sign-up and participant status in the program was used to determine growth in active participants over the 9-month time period, as well as participant retention over this same period.
Data Analysis
The frequency of demographic and other characteristics for all participants who received at least one volunteer phone call, as well as for the subset of older adults who completed Wave 1 (n = 31; hereafter referred to as “partial respondents”) and Wave 2 (n = 17; hereafter referred to as “complete respondents”) are reported. T-tests and Chi-square were used to identify any significant differences in average age, gender, race/ethnicity, and location between all participants and complete respondents.
Mean volunteer satisfaction data are reported among partial respondents, while mean HFS, PHQ-2, and stress due to COVID-19 scores, and frequency of weekly social outings are reported for Waves 1 and 2 among the complete respondents. Wilcoxon Signed Rank Test was used to determine significant differences between Waves 1 and 2. A longitudinal analysis compared changes in the depression and friendship outcomes in Waves 1 and 2 between short-term and long-term participants.
Results
Participant Demographics
Wave 1 participants (n = 31) had a mean age of 72 years, over three quarters were female (n = 27) and over half (n = 22) non-Hispanic white, while an additional 19% did not report race/ethnicity (Table 1). Participants resided in both major metropolitan areas in Nevada (Clark County, n = 15 and Washoe County, n = 14) as well as rural counties (n = 2). There were no statistically-significant differences in demographic characteristics between individuals who completed Wave 1 and all program participants; however, participants who completed Wave 1 were less likely to be white than those who completed Wave 2. Other demographic information, such as veteran status, driving status, mobility device use, and residence status were also collected and reported in Table 1. For both surveys, most respondents were not veterans, did not drive, and reside in a private residence.
Demographic Information.
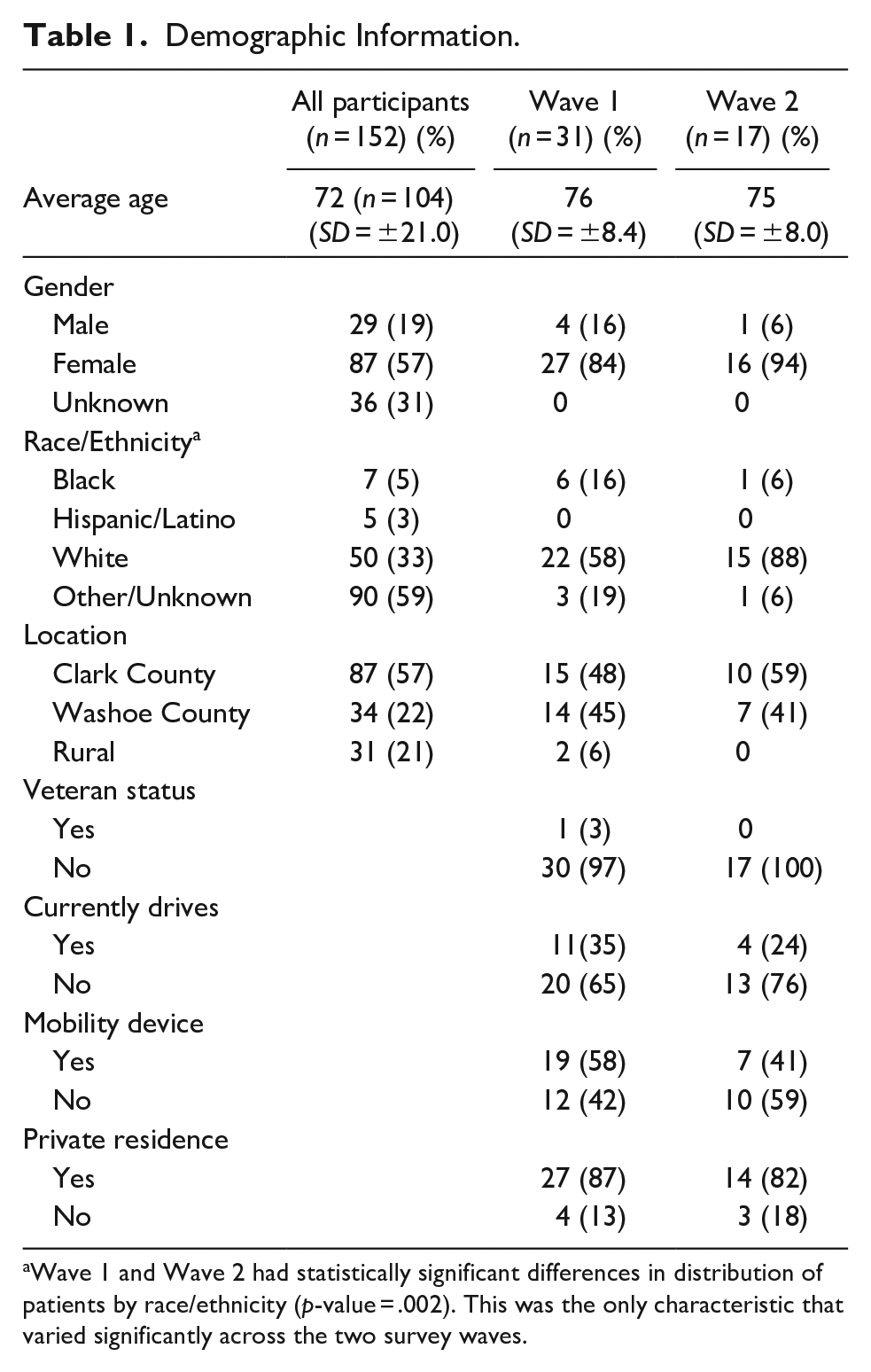
Wave 1 and Wave 2 had statistically significant differences in distribution of patients by race/ethnicity (p-value = .002). This was the only characteristic that varied significantly across the two survey waves.
Pre-COVID-19 Outings and Social Isolation
Wave 1 data indicate that 71% of participants were able to leave their house prior to COVID-19 lockdown measures, 52% had an average of 1 to 3 social outings per week, and 52% had occasional feelings of social isolation prior to the lockdown measures (Table 2).
Questions about pre-COVID-19 life. a

Asked during Wave 1 only.
Modified PHQ-2, Hawthorne Friendship Scale, and Stress Level
Figures 1 and 2 report PHQ-2 and HFS outcomes among the set of complete respondents, respectively (n = 17). Overall, average PHQ-2 scores decreased from 2.0 to 1.8 between surveys, but this improvement was not statistically significant (p: .19). The average HFS also decreased from 3.1 to 2.8, and this improvement was also not statistically significant (p: .45).

Modified PHQ-2 scores for respondents who completed both Wave 1 and 2 surveys.

Modified Hawthorne Friendship Scale for complete respondents who completed both Wave 1 and 2 surveys. Felt Isolated reverse scored to match lower is better.
Figures 3 and 4 compare changes in PHQ-2 and HFS scores between short-term and long-term participants. Among short-term participants, average PHQ-2 scores increased from 1.8 to 2.0 between waves, whereas among long-term participants, average PHQ-2 scores decreased from 1.9 to 1.2. Conversely, among short-term participants, average HFS decreased from 3.1 to 2.9. between waves, whereas among long-term participants, the average HFS was constant across the two waves (2.9 and 2.9).
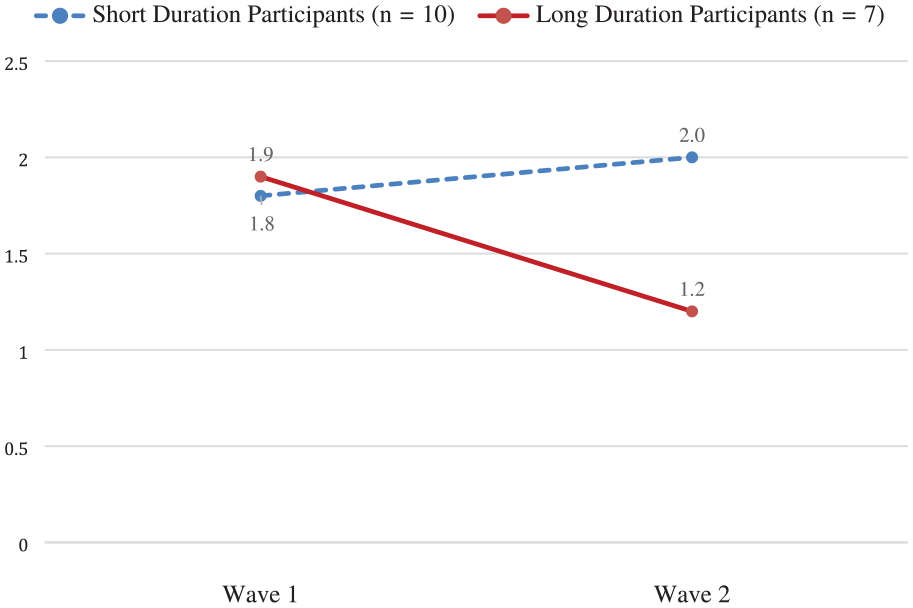
Comparing average PHQ-2 scores for short-term and long-term participants at Wave 1 and Wave 2.

Comparing average HFS scores for short-term and long-term participants at Wave 1 and Wave 2.
Among complete respondents, participants indicated that over the last 2 weeks, they felt stress due to COVID-19 “not at all” (7%), “occasionally” (61%), “about half the time” (7%), “often” (13%), and “almost always” (7%) in both Wave 1 and Wave 2 (data not in figures).
Participant Growth and Retention
Total participant numbers increased steadily throughout the study period. The number of active participants increased from 65 as of October 2020 to 109 as of July 2021. This represents a 68% increase in active participants over 9 months. Of the 65 active participants (receiving and answering calls from volunteers) from October 2020, 42 of these participants were still active in July 2021, resulting in a 65% retention rate of participants over the 9 months.
Satisfaction With Volunteers
Across both waves, the set of partial respondents indicated that most were either extremely satisfied or satisfied with their volunteer (Wave 1: 92%; Wave 2: 100%). Also in both waves, all respondents said they were either satisfied or extremely satisfied regarding call frequency (Wave 1: 84% received 1 call per week, 12% received 2 calls per week; Wave 2: 76% received 1 call per week, 24% received 2 calls per week), the length of calls (Wave 1: 22 minutes; Wave 2: 22 minutes), and the volunteer’s ability to listen.
Discussion
Evidence from the COVID-19 pandemic has found that older adults are prone to declining mental health due to both externally-imposed and self-imposed social distancing measures (Krendl & Perry et al., 2021). Here, we evaluate a one-to-one, remote, multi-generational, volunteer-led social phone call intervention intended to reduce social isolation, loneliness, depression and anxiety during the COVID-19 pandemic. This intervention may also have broader applications to address social isolation, an growing societal problem, among older adults more generally. Results from the modified PHQ-2 and HFS showed modest but statistically insignificant improvement in scores.
Our study had several limitations. First, without a comparison group, we cannot assume a causal relationship between the intervention and the outcomes. Second, low response rates, particularly on the second survey, reduced statistical power. Third, to simplify a lengthy survey comprising of multiple scales, and selecting items conceptually linked to the intervention of interest, we modified the PHQ-2 scale and Hawthorne Friendship Scale, resulting in instruments that deviate from the validated instruments. Further, the voluntary nature of NEST Collaborative participant recruitment may have resulted in a study sample with low baseline levels of depression, social isolation, and anxiety, reducing the potential for significant changes in outcomes. External validity may have also been reduced due to underrepresentation of people of color among program participants (including Hispanic individuals, though we did offer services in Spanish when needed), and people who live in rural counties among those surveyed. A final limitation is the lack of data collected regarding the needs of older adults, which was beyond the scope of this study.
The PHQ-2 is validated as a first-step approach to inquiring about the frequency of depressed mood over a 2-week time frame (Löwe et al., 2005). Average PHQ-2 scores reported in this evaluation are below 3, suggesting participants, on average, are not candidates for additional diagnostic screening and that they are not likely to be experiencing any depressive disorder (Levis et al., 2020; Löwe et al., 2005).
The modest change in PHQ-2 and HFS scores noted in Figures 1 and 2 are notable in the context of the COVID-19 pandemic, which has resulted in people across all age groups having higher rates of depression and loneliness, with older adults experiencing the highest rates (Krendl & Perry, 2021; Lee et al., 2019). It is possible that, in the absence of the intervention, PHQ-2 and HFS scores would have increased (indicating poorer well-being), although without a comparison group, this cannot be confirmed. However, the downward trend of both depression and loneliness should be interpreted in light of the COVID-19 pandemic and its established negative impact on mental health (Sher, 2020). The NEST Collaborative leadership consider these results to be programmatically-meaningful outcomes.
The patterns in PHQ-2 and HFS scores observed among participants with comparable participation durations also merit further discussion. According to Figure 3, participants with less than 6 months in the program saw a slight increase in the PHQ-2 score while participants with more than 6 months in the program saw a modest decrease (i.e., improvement). This is consistent with the established notion that longer interventions tend to produce greater decreases in PHQ-2 scores (Löwe et al., 2005).
Conversely, Figure 4 illustrates a modest decrease (i.e., improvement) in HFS scores among participants with less than 6 months in the program, but the scores were constant for participants with more than 6 months in the program. This observation may reflect immediate benefits to developing a novel friendship; however, over time, due to the novelty of relationships wearing off, people in those relationships may adjust to the acquaintanceship, resulting in a leveling of HFS scores (Amati et al., 2018). Further, lack of statistically-significant improvement, while certainly attributable to the small sample size and statistical power considerations, may also be due to limitations of phone call-based interventions (Gorenko et al., 2011).
Kahlon and colleagues’ study of 240 participants receiving daily empathy-based social support telephone calls found statistically-significant improvements in the UCLA Loneliness Scale, PHQ-9, and Generalized Anxiety Disorder scale (Kahlon et al., 2021). Their intervention involved more frequent calls then the NEST Collaborative social calls, where participants report an average of one call per week. While noting that the frequency of calls was determined by the participants, it may be that more frequent calls are the key to significant change in the outcomes. However, without a larger study, we cannot conclude whether or not the comparatively low resource-intensive NEST Collaborative did or did not impact the outcomes of interest. Still, the pilot data reported here lend credence to future study of similar remote-support programs to more fully document the potential impact.
Data from this evaluation were shared with The NEST Collaborative Advisory Team over a 2-hour interactive session led by the Director of the Sanford Center for Aging. A qualitative summary from this meeting noted that the evaluation data boosted volunteer, program staff, and social service partners’ morale. Current volunteers expressed that noting improved social isolation and depression outcomes and universally high satisfaction data among program participants encouraged their continued engagement. In response to this discussion, the Support Team asked each volunteer to ask their program participants, once again, if they would like to receive phone calls once or twice per week, or more. The overwhelming majority of program participants confirmed that they only wanted to be called once per week, and so the NEST Collaborative supported that preference. Additionally, the demographic data proved to be highly valuable for the Advisory Team. As shown by the data, there are very few participants from rural areas of Nevada. This type of information informed further outreach efforts.
Given the programmatically-meaningful outcomes of the NEST Collaborative in reducing loneliness and depression during the highly-stressful context of the COVID-19 pandemic, there are several policy and practice implications worth noting. First, aging policy should identify new opportunities and resources to expand the availability and reach of telephone-based, intergenerational, volunteer-led, empathy-based social support for isolated older adults. As previously described, while the pandemic was a universally-isolating experience, a high percentage of older adults regularly experience social isolation, and thus there is the potential for related negative health outcomes even beyond the pandemic context. With the relative low-cost nature of offering empathy-based telephone social support, new state and federal funds could be designated to expand and replicate this type of intervention.
Second, with the potential for expansive geographic reach of a telephone-based support program such as the NEST Collaborative, a review of current funding restrictions may be warranted to ensure that funders enable service delivery across state lines. Many state-supported program grants are limited to service delivery in their own geography, but many additional older adults could be served if funds were available to support “regional hubs” covering a broader territory.
Expanded access to remote social support programs might also be possible through existing healthcare infrastructure. For example, hospitals may be able to identify older adults in need of social support, and could potentially train and organize volunteers already involved in hospital operations into volunteer social call roles. This may be a cost-effective way to reduce the burden of health conditions associated with social isolation. Offering this program through a healthcare organization well known in the community may increase visibility and thus reach a wider audience. However, aligning social supports with medical organizations may be counterproductive in including older adults who associate medical providers with the mistreatment of people of color and thus have a mistrust of medical institutions.
Finally, there is a need for additional intervention design and comparative analysis to consider the relative impacts of telephone, Internet, hybrid and in-person social support programs. This is particularly relevant to exploring the programmatic delivery modality that not only achieve its intended outcomes, but is most readily accessible to and adopted by the highest number of isolated older adults, including those in Black, Immigrant, and Indigenous communities.
Conclusion
This study reports promising trends in improvement for outcomes associated with social isolation in older adult participants of a remote, multi-generational, volunteer-led social support intervention. Although this initiative originated as a rapid response to the increased incidence of homebound older adults due to the COVID-19 pandemic, the infrastructure this program provides will continue to be used for homebound populations even after many older adults in Nevada become fully vaccinated. For the benefit of homebound elders, more studies such as this one should explore the outcomes of remote, multi-generational, volunteer-led interventions. Ensuring availability of robust, widely available, easy-to-access social support programs is a need that will continue to be relevant for the foreseeable future, and programs such as the NEST Collaborative represent innovative ways to extend program reach as aging services agencies fulfill that need.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214221125357 – Supplemental material for Exploring the Impact of The NEST Collaborative’s Remote Social Intervention on Feelings of Depression and Isolation
Supplemental material, sj-docx-1-ggm-10.1177_23337214221125357 for Exploring the Impact of The NEST Collaborative’s Remote Social Intervention on Feelings of Depression and Isolation by Ryan W. Nolan, Sarah Friedman, Jennifer Carson, Zebbedia Gibb, Casey Acklin and Peter S. Reed in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The IRB determined this study to be exempt and HIPAA identifiers are not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.