
Abstract
Keywords
Introduction
Effective communication about behaviors to minimize risk and facilitate early treatment of infectious diseases is a critical public health mission. This is especially underscored by the COVID-19 pandemic which, as of this writing, is associated in the United States with nearly 90 million infections and one million deaths (https://covid.cdc.gov/covid-data-tracker/#trends_dailycases). An online survey (Geldsetzer, 2020) in February-March 2020 evaluated knowledge of COVID-19 symptoms and procedures to minimize infection in nearly 3,000 residents of the United States or United Kingdom. In both countries, common symptoms such as fever and cough were recognized by >95% of respondents, whereas the effectiveness of ways to prevent the disease such as wearing a mask was reported by <50%. Another online survey (Pagnini et al., 2020) in Italy conducted during the last week of February-the first week of March 2020 found that of 2,813 respondents, 17% said it was either false or they did not know whether the virus could be transmitted from person to person, and 13% said it was either false or they did not know whether someone suspected of having the virus should wear a mask around other people.
Adults ≥50 years are at high risk for adverse COVID-19 outcomes including severe illness and death, and thus represent an important demographic segment to target in public health campaigns. As of Spring 2022, compared with 18- to 29-year-olds, the rate of hospitalization is three times higher in individuals 50 to 64 years, five times higher in individuals 65 to 74 years, and eight times higher in those 75 to 84 years old. Death rates follow an increasing trend as well, with higher rates, compared to 18- to 29-year-olds, of 25, 60, and 140 in persons ages 50 to 64, 65 to 74, and 75 to 84 years, respectively (https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html).
One potential confound that may interfere with acquisition and retention of health-related knowledge is co-existing cognitive impairment since older adults are at increased risk for mild cognitive impairment (MCI) and dementia (Hale et al., 2020). Alsan et al. (2020) observed that knowledge about COVID-19 symptoms and surface contact disease spread was greater in older adults ages 55 to 64 years compared to persons <30 years. However, the possible impact of cognitive status was not investigated in their study. In contrast, Babicz et al. (2021) found that lower cognitive functioning is associated with poorer knowledge of COVID-19 symptoms. These investigators conducted a telephone-based survey of COVID-19 symptom and preventive knowledge in individuals with a mean age of 35 years (range = 18–77). Study participants were also administered a battery of telephone-based cognitive measures. Greater accuracy was predicted by better memory and executive functioning performance, after controlling for education, estimated premorbid ability, and health literacy.
In the current study, we focused on an older group of individuals (range = 50–89 years) to examine the effects of cognitive status on knowledge of COVID-19 symptoms, risks, and protective strategies. Cognitive status was assessed via a screening measure, the Montreal Cognitive Assessment (MoCA) (Nasreddine et al., 2005), which is commonly used in geriatric primary care settings. We predicted that higher scores on the MoCA would be associated with more correct responses reflecting the current state of knowledge about COVID-19, and that MoCA Index scores of memory and executive functioning would be associated with greater accuracy.
Methods
Design
This study used a cross-sectional design.
Participants
Data were collected from study participants who were prospectively enrolled in the Cognitive Empowerment Program (CEP), a comprehensive lifestyle program representing a research collaboration between the Neurology Department of Emory University School of Medicine and the School of Interactive Computing and the School of Architecture at Georgia Institute of Technology. The CEP is aimed at empowering individuals to address modifiable risk factors associated with cognitive impairment symptomatology via cognitive, physical, social, functional independence, education, and wellbeing activities. Members are referred by clinicians in Emory’s Cognitive Neurology Clinic, where they have received assessment of their cognitive functioning and instrumental activities of daily living, laboratory tests, and neuroimaging. Program partners are engaged in the CEP as well and are invited to attend classes with the members. The CEP protocol is approved by the Emory Institutional Review Board, and all members and care partners sign informed consents allowing researchers to access their records. The research was completed in accordance with the Helsinki Declaration.
To be included in the current study, participants were required to be 50 years and older and to have completed the COVID-19 Knowledge Questionnaire and the MoCA.
Procedures
COVID-19 Knowledge Questionnaire
Questions were selected from those used in national surveys of residents of the United States, United Kingdom, and Italy during the pandemic (Alsan et al., 2020; Geldsetzer, 2020; Pagnini et al., 2020). Questions were from the World Health Organization’s “myth busters” Website (https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters) such as whether garlic or gargling with mouthwash can prevent COVID-19. Questions were eliminated that were no longer relevant such as the availability of a COVID-19 vaccine (“There is currently no effective cure for COVID-19”) or that remained controversial at the time (“Eating or contacting wild animals would result in infection”). There were 22 questions requiring true or false responses, 11 of which enquired about COVID-19 symptoms and transmission, and 11 about recommended protective behaviors.
Program participants were sent a HIPPA compliant zoom link between August 2020 and May 2021. Instructions were, “Please answer the following questions either True or False. You must answer every question, so if you’re not sure that’s okay, just go with your best response.” Cohabitating respondents were sent separate links and asked to independently complete the questionnaire.
Cognitive measure
The MoCA (Nasreddine et al., 2005) is a cognitive screening instrument ranging from 0 to 30 points, with higher scores signifying better performance. The MoCA (https://www.mocatest.org/the-moca-test) is a reliable and validated instrument for the detection of cognitive impairment in older adults, surpassing the Mini-Mental State Examination in discriminating between those with normal versus mild cognitive impairment (Pinto et al., 2019). In addition to the total score, we derived scores on six MoCA subdomains based on the item combinations used by Julayanont et al. (2014). These include the following: (1) Memory Index Score: Number of words recalled in delayed free, category-cued, and multiple choice conditions, multiplied by 3, 2, and 1 respectively (0–15 points); (2) Executive Index Score: Trail-Making, Clock, Digit Span, Letter A Tapping, Serial 7 Subtraction, Letter Fluency, Abstraction (0–13 points); (3) Visuospatial Index Score: Cube Copy, Clock, Naming (0–7 points); (4) Language Index Score: Naming, Sentence Repetition, Letter Fluency (0–6 points); (5) Attention Index Score: Digit Span, Letter A Tapping, Serial 7 Subtraction, Sentence Repetition, Words Recalled in Both Immediate Recall Trials (0–18 points); and (6) Orientation Index Score: Orientation Items (0–6 points).
Analyses
Categorical data are presented as frequencies and percentages. Distribution normalities were evaluated for the MoCA and the COVID-19 Knowledge Questionnaire using the Kolmogorov-Wilk statistic, which confirmed statistically significant deviations from normality. Therefore, Spearman non-parametric correlations were performed to examine the association between the number of total correct responses (out of 22 possible) to the COVID questionnaire and the total score and the indices of the MoCA. Significance was set at p < .05, two tailed. Analyses were performed using SPSS v. 24.
Results
The final sample included 99 participants with complete COVID-19 Knowledge Questionnaires and MoCA scores. The mean age of the sample was 72.6 years (SD = 7.6, Range = 50–89). Six (6%) had high school degrees, 12 (12%) had some college education, 41 (41%) had college degrees, and the remaining 40 (40%) had advanced degrees. Forty-eight respondents were female. All but five of the respondents self-identified as White/Caucasian.
Table 1 shows the accuracy in answering the COVID-19 questions. The mean accuracy was 19.8 (SD = 2.0), with a range between 12 and 22 correct responses. More than 90% of respondents answered 14 of 22 questions correctly. Of the remaining questions for which the overall accuracy was present in fewer than 90% of respondents, 62% knew that compared to a cold, the symptoms including a stuffy nose, runny nose, and sneezing were common. Eighty one percent of respondents knew that a mask was not the only way to prevent infection, and 85% knew that social distancing rules do not state that individuals should be 4 ft apart. In terms of recommended protective behaviors, 72% of respondents knew that a vaccination for pneumonia was not recommended as protective, and 79% knew that gargling with mouthwash was not protective. Sixty-six percent of respondents knew that use of a hand dryer was not protective, and 87% knew that regularly rinsing one’s nose with saline was not protective. Finally, 85% of respondents knew that taking antibiotics was not recommended as protective.
Number (%) of Participants Providing Correct Answers to Questions About COVID-19 Symptoms, Risks, and Protective Strategies.

Relationship Between Accuracy and Cognitive Functioning
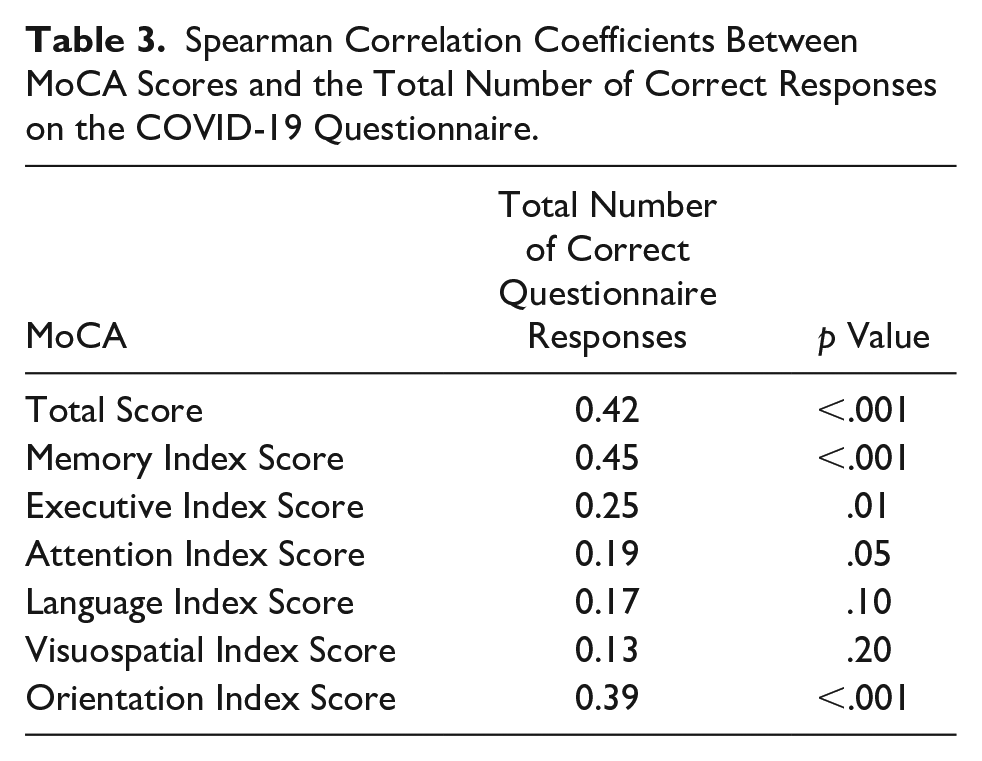
Scores on the MoCA are shown in Table 2, and the results of Spearman correlations between MoCA scores and number of correct responses on the Covid-19 Questionnaire are shown in Table 3. A higher number of correct COVID-19 Questionnaire responses was moderately associated with a higher total MoCA score. Higher scores on the Memory and Orientation Indices were also moderately associated with a higher number of correct COVID-19 Questionnaire responses, with a weaker association observed for the Executive Index score. In contrast, there were no significant associations with the Attention, Language, and Visuospatial Indices.
Montreal Cognitive Assessment Total and Index Scores.

Spearman Correlation Coefficients Between MoCA Scores and the Total Number of Correct Responses on the COVID-19 Questionnaire.
Discussion
Studies in the United States measuring knowledge of COVID-19 symptoms and prevention behaviors have focused on minorities, with findings of racial/ethnic disparities in Blacks, Hispanics and Asians (Jones et al., 2020; Reiter & Katz, 2021). Our study extends this to older adults who represent another vulnerable group for poor outcomes. Over half of the COVID-19 questions were answered correctly, that is, reflecting the current state of public health information and recommendations regarding COVID-19, by >90% of all participants. However, there were also weaknesses, with ≤80% knowing the salient symptoms of COVID-19 compared to the common cold, or knowing the myths related to prevention including gargling with mouthwash, getting a vaccination for pneumonia, or using a hand dryer.
We observed that lower total MoCA scores and lower MoCA Index scores of Memory Orientation, and Executive functioning were associated with lower accuracy. These findings correspond with prior studies that show disease related knowledge of medical conditions such as diabetes, hypertension, and heart disease is associated with cognitive functioning (Levinthal et al., 2008; Morrow et al., 2006; Wykes et al., 2017). With respect to COVID-19 knowledge, our findings are consistent with Babicz et al. (2021) who found that greater accuracy was predicted by better memory and executive function. As noted by these investigators, an association with memory is intuitive since it is critical for encoding and retention of information. Likewise, it makes sense that being oriented is a necessary component of acquisition and retention. Intact executive functioning guides the initial organization of to-be-learned information and retrieval strategies (Babicz et al., 2021). More detailed cognitive testing may have revealed additional associations that were not appreciated in the current study.
A challenge is to promote public health messages that are tailored to provide older adults, including those with cognitive impairment, with effective education about disease risks. Compensatory strategies such as spaced retrieval and elaboration have been proposed as having possible value (Babicz et al., 2021) but have not yet been applied to acquisition and retention of COVID-19 knowledge. Another challenge is that health knowledge is necessary but not sufficient for translation into adherence behaviors. Adherence to COVID-19 protocols is especially pertinent to people with cognitive impairment as these recommendations tend to be complex and do not yield immediate reinforcement (e.g., perceivable lack of contracting the virus), making them less likely to be followed. Through our collaboration with investigators at the Georgia Institute of Technology, the CEP has installed sensors and is using other behavioral observations to correlate knowledge with adherence behaviors such as maintenance of social distancing recommendations and wearing a mask.
A strength of our study includes a focus on older adults who represent a segment of the US population that has been profoundly impacted by the COVID-19 pandemic. Advances in medicine have resulted in more individuals living into old age than previous generations. With age being the greatest risk factor for dementia, an increasingly older population will result in significant increases in the incidence and prevalence of dementia. Our findings of a relationship between cognitive status and knowledge of preventive strategies underscore the vulnerability and the importance of ensuring that older persons with cognitive compromise are protected. A limitation of our study is that our sample included persons who were well-educated and are not representative of the general population. It is possible that knowledge about COVID-19 recommendations, risks, and prevention strategies would be more compromised in persons with less education or health literacy (Manly et al., 2005). Further, our sample predominantly self-identified as White, and thus information related to the interaction of race, age, and cognitive status should be further explored. Finally, we do not have information available that could impact the responses to the questionnaire including whether the respondents had a personal history or a significant other with COVID-19, and whether “knowledge” translated into actual health outcomes such as not contracting the virus.
Conclusions
In summary, the COVID-2019 pandemic has wreaked havoc on the health and emotional well-being of millions of individuals, including older adults. Persons with associated cognitive impairment may be especially vulnerable and should be a priority of health care messaging to ensure acquisition, retention, and maintenance of knowledge and adherence to preventative recommendations.
Footnotes
Authors’ Note
This work was made possible by the Charles and Harriet Shaffer Cognitive Empowerment Program and the James M. Cox Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Cognitive Empowerment Program Protocol is approved by the Emory University Institutional Review Board (IRB00116995)