
Abstract
Effective, scalable mental health programs are greatly needed for older adults. In this study, Mood Lifters—a peer-led, community-based program promoting mental well-being—was adapted to more specifically address the needs of older adults. Two groups completed the 14-week program via Zoom. A total of 24 participants enrolled (Mage = 72 years), with 20 (83%) completing the program. Compared to baseline, program completers showed significant improvements in depression symptoms (p < .01), perceived stress (p = .04), sleep quality (p < .01), physical activity (p < .01), and brain health behaviors (p = .01), with improvements maintained at 1-month follow-up. No significant changes were reported in participants’ anxiety, loneliness, or resilience. Participant ratings of program satisfaction were very high (M = 4.75/5). Results suggest Mood Lifters for Seniors is feasible to disseminate and acceptable to older adults, with preliminary evidence of benefits in several mental health domains. Future randomized trials with larger, more diverse samples are needed to confirm program benefits.
What This Paper Adds
• This paper describes the development and initial evaluation of a new, innovative community-based group psychoeducation program to promote mental health in later life.
• The intervention described in the paper represents a novel approach to enhancing mental wellness among older adults.
Applications of Study Findings
• Preliminary results suggest the program has promise as an effective approach that can be widely disseminated to address growing mental health service needs among older adults.
• If future studies with larger, more diverse populations show similar results, the program could be offered for wider use in community settings.
Introduction
Mental health problems are relatively common among older adults, with high rates of clinical depression, depressive symptoms, and anxiety (Haigh et al., 2018; Wolitzky-Taylor et al., 2010). Compared to other age groups, older adults are more likely to report sleep disturbances and social isolation (Cudjoe et al., 2020; McLay et al., 2021; Miner & Kryger, 2017), especially during the COVID-19 pandemic (Creese et al., 2021; Gerlach et al., 2021; Kotwal et al., 2021). In addition, mental health challenges often accompany the health problems and physical limitations associated with later life (Wilson-Genderson et al., 2017). Although older adults often possess wisdom and coping skills from their life experiences and demonstrate resilience in the face of adversity (MacLeod et al., 2016), many could benefit from help and support for a wide range of mental health challenges (Houtjes et al., 2010).
Although several evidence-based mental health interventions have been developed for older adults (Niclasen et al., 2019), the majority of those in need do not seek or receive treatment (Bor, 2015). Several factors contribute to this problem. First, mental health services are often expensive and/or not covered by Medicare or other insurance plans (Byers et al., 2012; Gunja et al., 2022). Second, mental health services are not easily accessible, particularly for those residing in low income or rural areas (Brenes et al., 2015). Finally, many older adults are not interested in traditional mental health services, often because they are not aware of the benefits, perceive help-seeking as potentially stigmatizing, or prefer other forms of support (e.g., via family, community, and religious groups; Nair et al., 2020).
Several strategies have been considered to expand the reach of mental health services designed to meet the specific needs of older adults. Group programs may be cost-effective (compared to individual sessions with professionals) and especially appropriate because they also offer peer support (Thombs & Carboni-Jiménez, 2021). Service delivery by paraprofessionals in community-based settings may be especially appealing to older adults, for whom stigma of mental health care may be a deterrent to help-seeking, particularly among members of racial and ethnic minority groups (Conner et al., 2010).
Although designed for a general adult population, Mood Lifters is one program that has combined these approaches to address common barriers to mental health care and to improve mental health among its participants. It is an evidence-based, manualized psychoeducation program that can be delivered by trained peers either in person or online. Participants attend 15 weekly, 1-hour meetings led by a paraprofessional who has previously completed the program and leadership training. Meetings focus on biopsychosocial topics that have been shown to impact mood and quality of life (e.g., sleep, negative thoughts, and interpersonal relationships). Group leaders use a structured curriculum and program manual to cover these topics. Participants are encouraged in group meetings to ask questions and discuss barriers and facilitators to making progress. Between meetings, members practice skills taught in group sessions and track them through a point system (e.g., 30 minutes of aerobic exercise counts as one point). In the original trial of the program, participants reported statistically significant improvements in anxiety, and those who completed more points or homework also reported statistically significant reductions in depression and perceived stress (Votta & Deldin, 2022). In the current study, we describe our adaptation of the Mood Lifters program for older adults.
Methods
Program Development
Mood Lifters for Seniors was adapted from an existing mental wellness program developed by two study co-authors (PJD and CMV). The original Mood Lifters program was developed iteratively through reviews of best practices in behavior change, positive psychology, and clinical interventions (e.g., cognitive-behavioral therapy [CBT] and dialectical behavior therapy), along with several pilot groups and revisions that culminated in a randomized control trial (Votta & Deldin, 2022). The Mood Lifters program consists of 15 weekly, hour-long peer-led meetings, with a focus on peer support and accountability for at-home practice of skills learned during group meetings. In the meetings, trained layperson graduates of the program serve as group leaders and instruct participants on evidence-based, biopsychosocial approaches toward improved mental health.
The program covers a variety of topics in multiple domains: behavior (e.g., behavioral activation), body (e.g., exercise), mind (e.g., cognitive restructuring), mood (e.g., emotional regulation), sleep (e.g., sleep hygiene), and social (e.g., relationship repair). In between meetings, participants are encouraged to complete mentally healthy behaviors they learned in the group session. For each behavior they accomplish in between sessions, they earn one point. Participants are encouraged to engage in enough behaviors to reach a preset behavioral point goal that they determine for themselves. At the beginning of each meeting, participants check in individually with their group leaders and complete a brief questionnaire that measures their mood, thoughts, and behaviors. They also submit the “points” that were earned that prior week (i.e., skills practiced). This process continues cumulatively throughout the program, with participants learning and practicing the skills that impact them the most.
The development team for the Mood Lifters for Seniors (MLS) program consisted of an interdisciplinary group with expertise in mental health and aging. Team members included experts in clinical geropsychology, geriatric psychiatry, adult development and aging, health communication, and health behavior change. This team met weekly to develop the MLS curriculum and design a plan for program implementation and evaluation. We formed a Community Advisory Board that met monthly during the initial phase of the program to provide feedback on potential program revisions. Board members included older adults who had completed the original Mood Lifters program, as well as those with ties to community organizations (e.g., senior centers) that could disseminate the MLS program. We also drew on survey responses of prior Mood Lifters program participants over age 65 that indicated preferences for session topics, activities, and program format. Based on the feedback received, we revised the original program in the following ways:
• Extended the length of meetings from 60 to 75 minutes
• Shortened the program by 1 week
• Tailored existing modules to be more relevant to older adults
• Created new modules of special interest to older adults, including brain health, loss and transitions, physical changes, and purpose
• Combined several existing modules in order to allow time for new content
• Included new practice options
• Increased the number and variety of activities in each meeting
• Redesigned the visual appearance of the participant manual with input from a graphic designer; changes included adaptations for an older audience (e.g., larger font size, more spacing) and addition of diverse images of older adults
• Revised the facilitation guide for meeting leaders
• Provided tech-support as needed before and during Zoom sessions
In creating both new and revised material for the program manual, we applied principles of health education to make content clear to readers regardless of their health literacy level. For example, we used plain language instead of jargon, deleted unnecessary words and content, and highlighted important information with frequent use of tables, figures, and bulleted lists. After extensive review and revision by the development team, we tested the new modules (e.g., brain health, coping with physical changes) via role play with the Advisory Board to ensure that content was clear and relevant to the target audience and that material could be adequately covered in a 60 to 75 minute session. Table 1 provides a summary of each session’s content.
Mood Lifters for Seniors (MLS) Program Overview.

Note. SMART = specific, measurable, attainable, relevant, and time-bound; ABCDE = activating event, beliefs, consequences, dispute, and exchange; W-PAGER = wisdom, positivity, acceptance, growth, engagement with life, and resilience.
Participants and Procedures
Eligible participants were community-dwelling, English-speaking adults aged 65 years and above who could participate in weekly group sessions held virtually. Participants provided written consent to participate in the study. Using brief validated measures, they were then screened for presence of neuropsychiatric symptoms and conditions (e.g., psychosis, cognitive impairment, and severe personality disorder) that might preclude meaningful involvement in, and/or prove disruptive to, group discussions (Brandt et al., 1988; Hirschfeld et al., 2000; Zanarini et al., 2003). We did not require a minimal level of depression or anxiety symptoms given that the Mood Lifters program is designed to benefit participants whether or not they are experiencing clinically significant mental health concerns. The primary referral source for study participants was a clinical research website hosted by Michigan Medicine. The study listing on this site generated considerable interest in the project such that recruitment goals were met in 2 weeks. All group sessions were held via Zoom, with participants receiving an orientation from study staff on how to use Zoom prior to the group’s first meeting. The first group took place from November 2020 to February 2021, while the second group ran from March to June 2021. Each group was facilitated by two group leaders.
Study Measures
Study measures included a set of validated questionnaires assessing psychological and behavioral outcomes administered via a Qualtrics online survey. Although most of these measures were used in the parent Mood Lifters program, we added others specific to an older adult population (e.g., depression and anxiety measures designed for a geriatric population). Data were collected at three timepoints: (1) within 2 weeks of the first group session; (2) within a week following the final group session; and (3) approximately 1 month after the second survey. Table 2 provides a summary of study measures and the timepoints at which they were administered):
Timing of Administration of Study Measures.

Participant characteristics
Standard self-report survey items assessed participants’ demographic characteristics, including age, gender, race/ethnicity, and years of education.
Program satisfaction
Participants responded to a series of statements about the quality of the program and asked to appraise each statement (1 = completely false to 5 = completely true). In addition, participants rated their overall group experience on a 5-point scale (1 = poor to 5 = excellent). We also asked participants to rate various program features, including session and program content, length, and pace (e.g., “just right” vs. “too short” or “too long”) and the quality of the program manual (“not,” “somewhat,” or “very helpful/easy to understand”).
Depression
The short form (15 items) of the Geriatric Depression Scale (GDS) was used to measure symptoms of depression commonly experienced in older adults (Brown & Schinka, 2005). Scores range from 0 to 15, where 0 to 4 = normal, 5 to 8 = mild depression, 9 to 11 = moderate depression, and 12 to 15 = severe depression.
Anxiety
The short form of the Geriatric Anxiety Scale (GAS) was used to measure anxiety symptoms commonly experienced in older adults (Byrne & Pachana, 2011). Scores range from 0 to 30 where 1 to 6 = minimal anxiety, 7 to 9 = mild anxiety, 10 to 11 = moderate anxiety, and 12 to 30 = severe anxiety.
Perceived stress
The Perceived Stress Scale (PSS) was used to measure perception and degree of stress across life situations (Cohen et al., 1983). Scores range from 0 to 40, where 0 to 13 indicates low, 14 to 26 indicates moderate, and 27 to 40 indicates high perceived stress.
Emotional regulation
The Emotional Regulation Questionnaire (ERQ) was used to measure respondents’ tendency to regulate their emotions in two ways: (1) Cognitive Reappraisal and (2) Expressive Suppression (Gross & John, 2003). Scores range from 6 to 42 for the Cognitive Reappraisal subscale and from 4 to 28 for the Expressive Suppression subscale, with higher scores indicating greater use of this regulation style.
Loneliness
The UCLA Loneliness Scale was used to measure subjective feelings of loneliness and feelings of social isolation (Russell et al., 1978). Scores range from 0 to 60, with higher scores reflecting more feelings of loneliness.
Resilience
The Connor-Davidson Resilience Scale was used to measure aspects of resilience, including flexibility, self-efficacy, emotion regulation, and optimism (Campbell-Sills & Stein, 2007). Scores range from 0 to 40, with higher scores suggesting greater resilience.
Flourishing
This variable was assessed using a scale developed by Diener et al. (2010) to measure self-perceived success in areas such as relationships, self-esteem, purpose, and optimism. Scores range from 0 to 56, with higher scores representing greater psychological resources and strengths.
Sleep
The Pittsburgh Sleep Quality Index (PSQI) was used to measure quality and patterns of sleep across multiple domains (e.g., sleep duration and efficiency; Buysse et al., 1989). Scores range from 0 to 21, with higher scores indicating worse sleep quality (a score of 5 or greater indicates a “poor” sleeper).
Physical activity
The Physical Activity Scale for the Elderly (PASE) was used to assess engagement in the types of activities typically chosen by older adults including walking, recreational activities, exercise, housework, and yard work (Washburn et al., 1993). The scale uses frequency, duration, and intensity of activity over the previous week to assign a score, ranging from 0 to 793, with higher scores indicating greater physical activity. Due to an error in web survey programming, this measure was not properly administered in our first group and so results are from second group participants only (n = 11).
Brain health behaviors
This variable was assessed using portions of a questionnaire from the Health and Retirement Study to assess frequency of engagement in activities related to improving and maintaining brain health (Smith et al., 2017). The measure included 10 items assessing cognitive activities (e.g., reading, word games) and 9 items assessing social engagement activities (e.g., volunteering, visiting with friends and family), with each activity rated on a 7-point scale (1 = never done to 7 = done daily). Scores range from 19 to 133, with higher scores indicating greater engagement in brain health activities.
Diet
A brief (eight item), validated dietary assessment was used to assess respondents’ eating habits (Paxton et al., 2011). Scores range from 0 to 16, with higher scores reflecting a less healthy diet.
Data Analyses
Descriptive statistics were used to characterize the study sample and its ratings of the MLS program. Descriptive statistics were also used to summarize survey responses, including mean scores on validated study measures. Paired t-tests assessed whether mean scores on key outcome variables differed across the study timepoints: baseline, immediate post-group, and 1-month follow-up.
Results
Program Completion
A total of 24 older adults enrolled in the program, with 12 in each group. Of these, 20 (83%) completed the 14-week program. Three of the four non-completers dropped out due to significant health concerns (e.g., diagnosis and treatment of a serious medical condition). Demographic characteristics of those who completed the program were as follows: Mage = 71.6 years (range: 66–80); 50% male, 50% female; 90% white; and 85% with a college degree. Demographic characteristics did not significantly differ between participants in the two groups.
Program Satisfaction
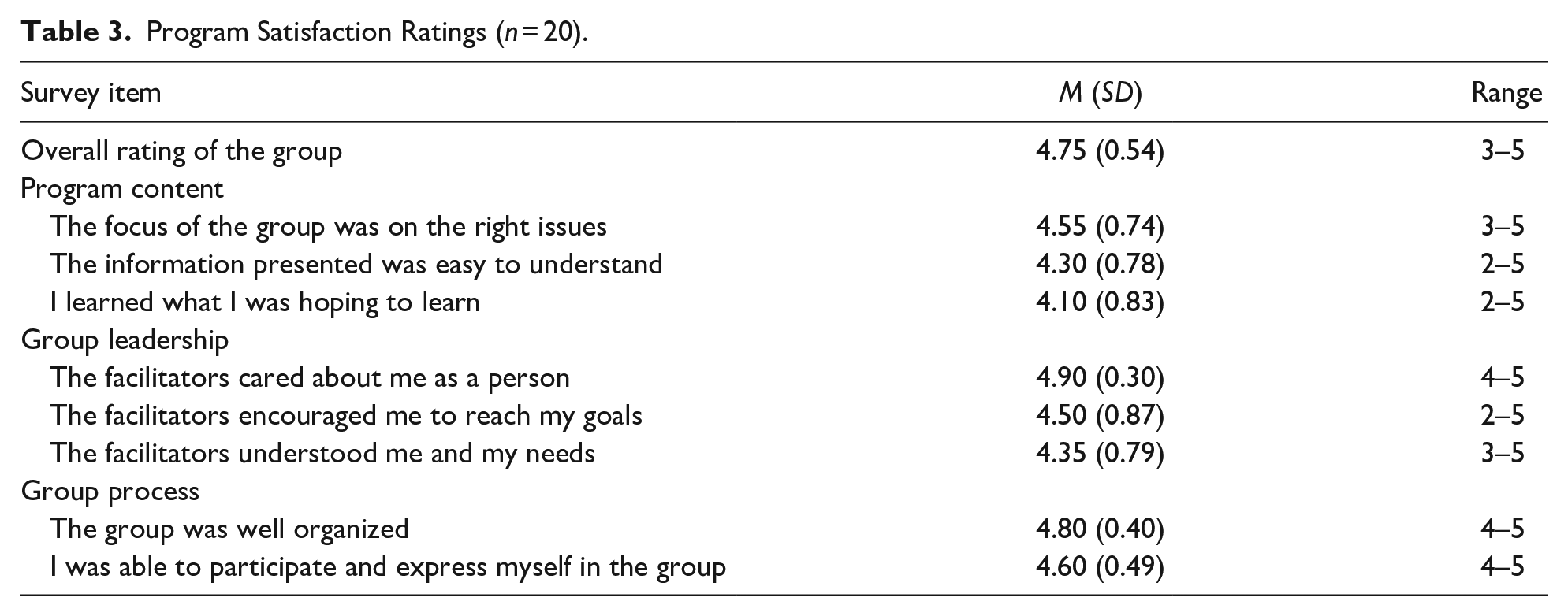
Participants rated the program highly, with a mean overall rating of 4.75 on a 5-point scale. Participants endorsed statements indicative of program strengths in terms of content, organization, and leadership, with each item having a mean of 4.1/5 or greater. The most highly endorsed items were “The facilitators cared about me as a person” (M = 4.9) and “The group was well organized” (M = 4.8), with the lowest rated item being “I learned what I was hoping to learn” (M = 4.1). A summary of survey responses in this domain is provided in Table 3. The vast majority of participants rated as “just right” the pace of group sessions (85%), the 75-minute length of sessions (90%), and overall program length of 14 weeks (75%). The vast majority of participants (19/20) found the program manual to be “somewhat” or “very helpful” and “somewhat” or “very easy to understand.”
Program Satisfaction Ratings (n = 20).
Psychological Outcomes
Participants reported a significant reduction in terms of depression symptoms, with mean scores on the GDS falling from 3.15 (SD = 2.78) at Time 1 to 1.8 (SD = 2.14) at Time 2 (
Participant Scores on Key Study Outcomes (n = 20).
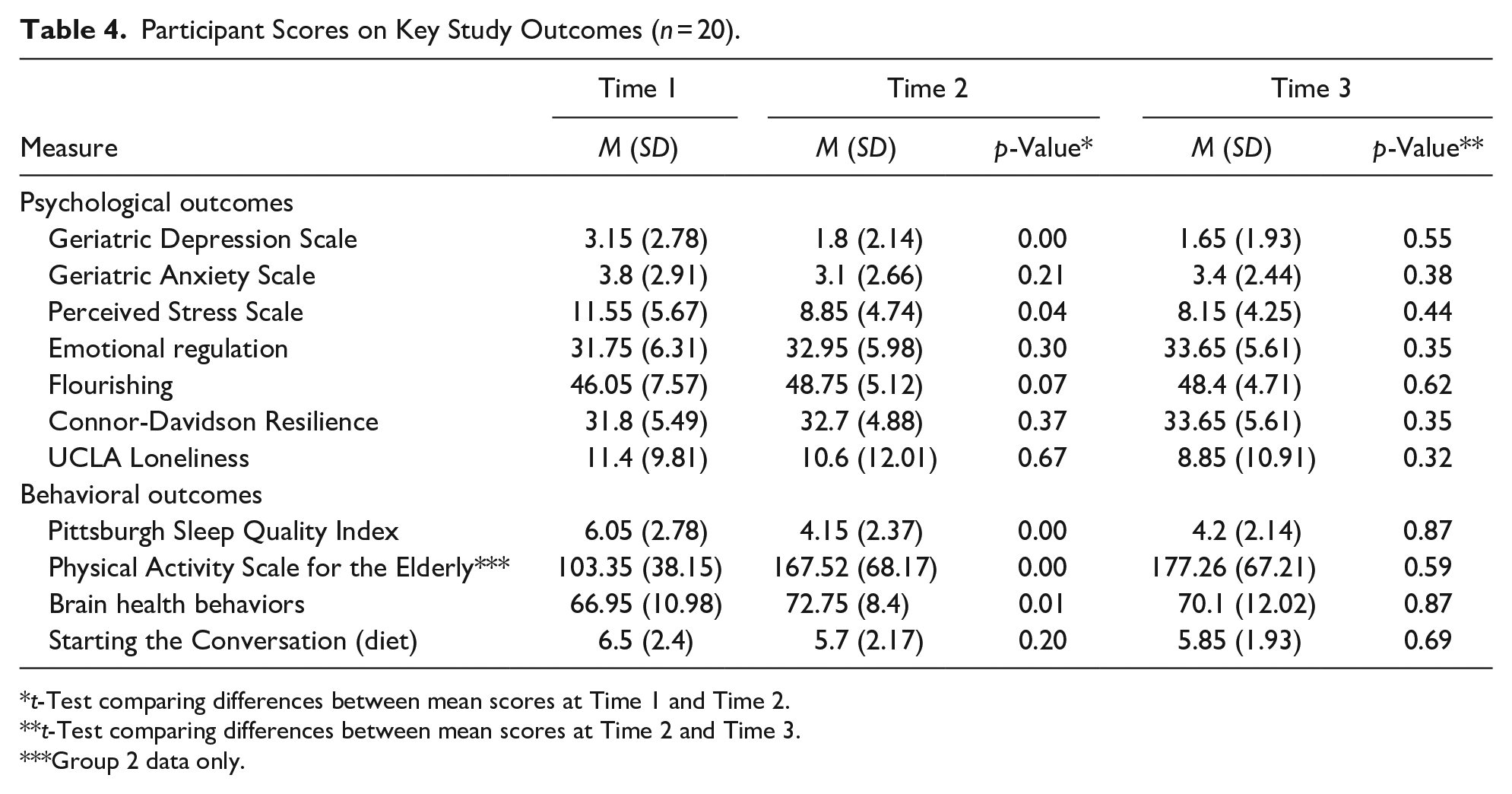
t-Test comparing differences between mean scores at Time 1 and Time 2.
t-Test comparing differences between mean scores at Time 2 and Time 3.
Group 2 data only.
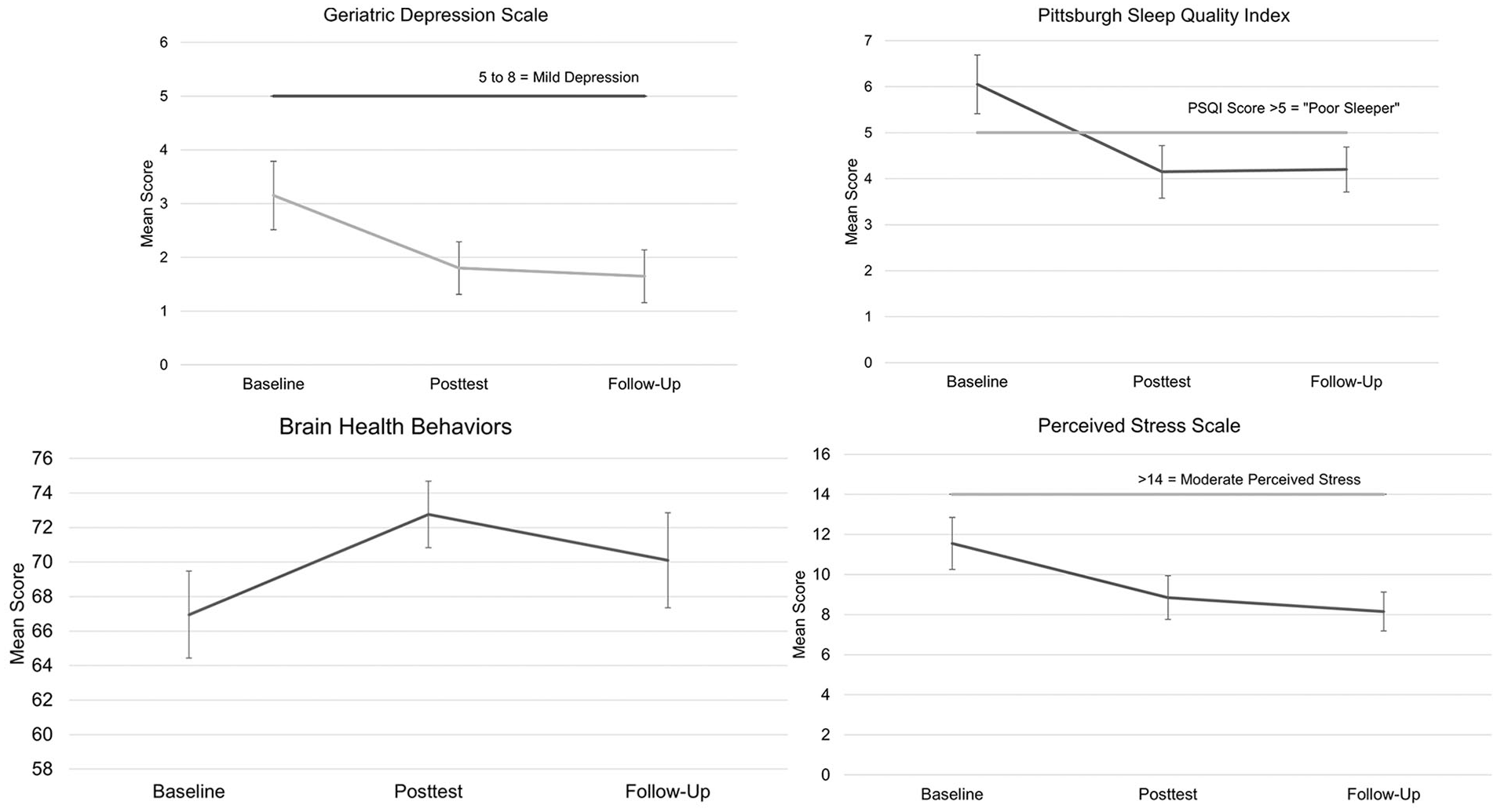
Changes in selected study outcomes following program participation.
Behavioral Outcomes
Participants reported significant improvements in terms of sleep quality, with mean scores on the PSQI falling from 6.05 (SD = 2.78) at Time 1 to 4.15 (SD = 2.37) at Time 2 (
Discussion
Study results suggest that the adaptation of the Mood Lifters program for older adults was successful in term of community interest, program completion rates, and levels of participant satisfaction. In addition, the adapted program resulted in significant participant improvement in multiple domains related to mental health and wellness. Results indicate that the program was acceptable to participants and feasible to implement. The vast majority of participants (>80%) completed all sessions of the 14-week program, with attrition unrelated to the program (e.g., significant health problems). Participants rated the program highly across all domains assessed, including group leadership, group process (e.g., pace and content of sessions), and information provided. Although delivering the program in an online format was not our original intention (and required participants to have reliable internet access), the remote format offers advantages in terms of program reach and accessibility. For example, the format is preferable for participants with transportation barriers, mobility limitations, and/or scheduling restrictions and in settings where reserving requisite meeting space might be challenging or costly (Weinberg, 2021).
Program participants showed improvements in several key psychological outcomes. For example, they reported lower levels of depressive symptoms and perceived stress following the program, with gains sustained at the 1-month follow-up survey. These improvements may be due to the focus in multiple MLS group sessions on strategies to elevate mood and manage stress. For example, the Thinking Traps session covered proven techniques from CBT to identify and change thinking patterns that create and sustain depressive symptoms (Thoma et al., 2015). Other sessions highlighted ways to regulate negative emotions and enhance positive emotions, such as distraction, radical acceptance, mindfulness, and cognitive reappraisal. Significant changes were not observed on all study psychological outcomes. For example, participants did not report statistically significant improvements in anxiety, loneliness, emotional regulation, resilience, or flourishing.
Program participants also reported improvements in key behavioral outcomes, including improved sleep quality. Gains were sustained at the study’s 1-month follow-up survey. Sleep was the explicit focus of one of the early group sessions, with group leaders and the program manual providing information on the sleep cycle, sleep changes commonly associated with aging, and factors influencing sleep (e.g., room temperature, caffeine intake). After that session, participants were asked to practice good sleep hygiene on a weekly basis, with points awarded for behaviors such as maintaining consistent sleep and wake times and avoiding stimulating activities before bedtime. Such strategies have proven to be effective in enhancing sleep quality (Chung et al., 2018). Participants also reported significantly greater engagement in physical activity and other brain health behaviors following program participation. Practice options in the Brain Health module reinforced behaviors highlighted in the national Alzheimer’s Association “10 Ways to Love Your Brain” campaign (Alzheimer’s Association, 2022), such as engaging in cognitively stimulating activities and maintaining social connections. Participant scores on a validated measure of dietary habits stayed relatively stable over the course of the study. Changes in this domain may require interventions more intensively focused on diet, given that sustained behavior change in this area is relatively difficult to achieve (Middleton et al., 2013).
There are several limitations that should be kept in mind when interpreting study findings. First, results are based on a small sample, relatively lacking in diversity in terms of racial/ethnic and educational background and socioeconomic status. It is unclear whether study results would generalize to larger groups more representative of the general older adult population. Second, the study lacked a comparison or control group, meaning that improvements observed on key outcomes may be attributed to factors unrelated to the study intervention. Finally, some ceiling and floor effects may have occurred because participants were eligible to participate even if they did not report depressive symptoms or anxiety at baseline. In addition, the small sample size limited the power to detect statistically significant changes from baseline across study domains. The use of brief (vs. longer form) symptom inventories as outcome measures might have also constrained power to detect intervention effects.
In conclusion, our results suggest that the Mood Lifters for Seniors program was feasible to implement in an online format and that content was acceptable and helpful to participants. Pilot testing suggested numerous benefits for participants in multiple domains related to mental health and wellness. In addition, the peer-led, online format fosters scalability and sustainability. Future studies with larger, more diverse samples will be necessary to confirm program benefits and potentially refine program content and procedures. Comparing in-person versus online group offerings would also be of interest; although we have already noted benefits of the latter approach, the former may be more useful in addressing outcomes such as loneliness and social isolation. Such research would ideally use a randomized clinical trial design and follow participants beyond program participation to determine whether and how program benefits persist over time.
Footnotes
Acknowledgements
The authors would like to thank members of our Community Advisory Board for their helpful feedback on the development and revision of program content; these members include Elizabeth Hammer, Venkat Lakshminarayanan, Maurine Nelson, and Monica Prince.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Deldin is the founder and Chief Executive Officer of Mood Lifters LLC. Dr. Votta is the co-founder and Chief Scientific Officer of Mood Lifters LLC. Ms. Porte was formerly the Director of Clinical Operations for Mood Lifters LLC. The other authors declare no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Michigan provided funding for this project through both its MCubed program and the Eisenberg Family Depression Center.
Ethical Approval
Approval was obtained for this study from the University of Michigan Health Sciences and Behavioral Sciences IRB (HUM00169614).