
Abstract
Introduction
Dementia is a major public health concern in the world, including in China. The World Alzheimer Report 2018 indicated that the global number of people living with dementia was estimated at 50 million, which number will triple by 2050 (Patterson, 2018). In China, dementia was estimated to affect about 5% of its aging population (Jia et al., 2020), and the estimated total annual costs of dementia in China increased from 0.9 billion United States dollars (US$) in 1990 to US$47.2 billion in 2010 and were predicted to reach US$ 69.0 billion in 2020 and US$ 114.2 billion in 2030 (Xu et al., 2017). The burden of dementia might become exacerbated with the large internal migration, as fewer young adults available to provide continuing care to the millions of older people with dementia, which is particularly problematic in rural regions (Zhang, 2017). There are no drugs so far to cure dementia or to modify its clinical course, and symptomatic medication has only modest effects (Cummings, 2004; Kaduszkiewicz et al., 2005; Livingston et al., 2020). Approaches for dementia focus on the early detection and treatment, underlining the importance of the prodromal phase of dementia, such as the mild cognitive impairment (MCI).
The concept of mild cognitive impairment represents an intermediate stage between normal aging and dementia. This is especially useful in the early stages of Alzheimer’s disease (AD), where individuals have a cognitive impairment beyond that expected for age and education yet do not have dementia (Petersen, 2011; Petersen et al., 2001, 1999). Several studies indicate that MCI can be regarded as a risk factor for dementia(Burns & Zaudig, 2002; Flicker et al., 1991; Gauthier et al., 2006; Morris et al., 2001; Petersen, 2004), as the conversion rate of MCI to dementia has been estimated to be 12% at 1 year, 20% at 3 years, and 50% at 5 years (Radler et al., 2020; Solfrizzi et al., 2004), and some even find that patients with MCI progress to dementia at a rate of 60% to 100% over 5 to 10 years (Hebert et al., 2003). In the absence of any effective therapy for dementia, identification of risk factors for the development of MCI may hold the best promise for preventing or delaying the progression from early cognitive dysfunction to clinical dementia (Boo et al., 2021; Roberts et al., 2008).
Risk factors related to cognitive impairment have been identified in several studies. A recent review article (Xue et al., 2018) reported that demographic characteristics like age, sex, and region of residence were associated with the incidence of MCI. Clinical characteristics, like depression (Richard et al., 2013), hypertension (Santisteban & Iadecola, 2018), diabetes (You et al., 2021), and other common physical and mental conditions, were also indicated to contribute to the incidence and progression of cognitive impairment. In addition, recent studies have tried to link sleep to the development of neurocognitive disorders, though current evidence for this relationship is conflicting (Rozzini et al., 2018; Stephens et al., 2022; Wams et al., 2017).
Several studies have reported the situation of MCI in China. Ding et al. (2015) reported the prevalence of MCI in Shanghai older residents aged 60 or more was 20.1%; Rao’s group found that 14.2% of elderly individuals aged 65 or more were affected by MCI in Guangzhou (Rao et al., 2018); F. Ma’s et al. (2016) research concluded a prevalence of 11.3% among older adults aged 65 or more in Tianjin. However, most of these studies were conducted in urban areas. In a recent systematical review of 48 studies reporting the prevalence of MCI (Xue et al., 2018), only 17.7% of the analyzed samples were recruited from rural areas, which limited the comprehensive understanding of the disease burden in the left-behind area in China.
In general, mild cognitive impairment (MCI) is considered to be a preclinical transitional state of dementia (Petersen et al., 1999) for which targeted interventions may be feasible. Identifying the prevalence of MCI in China is crucial for assessments of potential disease burden and therefore the need for interventions to prevent or slow progression of decline to dementia. However, few studies have reported the prevalence of MCI in rural China. In the present study, we investigated the prevalence of MCI in a rural town of Zhejiang Province, China, and analyzed its associated risk factors.
Methods
Setting and Participants
The study was conducted from April to November, 2019, in a rural town of Zhejiang Province, China. Eight out of 24 villages in the town were randomly selected, with population aged 60 or more registered in the electronic medical record (EMR) system was 3375. All these older adults were potential participants of the research, and the participant procedure was shown in Figure 1.

Participant procedure.
After the randomization and identification, 10 trained primary care physicians (PCPs) employed by the research group accessed these older residents whether in the primary care clinics, senior citizens activity centers, or their homes, introducing the research, inviting them to participate, evaluating for eligibility and making the study interview. The interview content included the participants’ demographic characteristics, comorbidity information and cognitive assessment, and it took about 30 minutes to complete the interview. All participants provided written informed consent before participation.
The inclusion criteria were as follows: (i) community-dwelling residents registered to the village; (ii) aged ≥60 years; (iii) no severe problems with vision, hearing, or speaking reported by the resident or informant (i.e., families) or observed by the PCP; and (iv) willing to give written informed consent.
Among the 3,375 community residents, 1,156 were excluded because of the following: (i) 479 were unable to access; (ii) 233 refused to participate; (iii) 161 were screened with dementia; (iv) 283 were excluded for the other reasons. The total number of the participants completing the interview, therefore, was 2,219. After excluding 73 with missing data, 2,146 pieces of data were available for analyses.
Measurements
Demographic information was collected using a standardized form developed for the study, variables derived included age, sex, education and literacy level, marital status, living conditions, and employment status. Information of chronic diseases, including hypertension, diabetes, hyperlipidemia, coronary heart disease and stroke, was also collected.
The diagnosis of MCI was made according to the Petersen criteria defined as:
(1) Cognitive concern reflecting a change in cognition reported by patient or informant (i.e., families);
(2) Objective evidence of impairment in one or more cognitive domains. Cognitive impairment was evaluated by the Montreal Cognitive Assessment (MoCA), which is a widely used assessment tool for detecting cognitive impairment (Nasreddine et al., 2005) and has been validated in the setting of MCI. The Chinese version of MoCA has been tested with acceptable validity and reliability (H. Li et al., 2009), and the cut-off score adopted in the study was 19/20 (Dong et al., 2013) adjusting for age and educational attainment;
(3) Preservation of independence in functional abilities. It was assessed by the Activities of Daily Living Scale (ADL), which is a commonly used assessment tool for daily functions (Lawton & Brody, 1969) and has been examined with acceptable reliability and validity as a supplement for the diagnosis of dementia and MCI. The cut-off value in the study was 14/15.
(4) Not demented with Clinical Dementia Rating (CDR) < 1 (Morris, 1997).
Data Analysis
Descriptive statistics (counts and proportions for categorical variables and means [± SD] for continuous outcomes) were used to depict the characteristics of the sample (e.g., age, gender, physical and functional status). We compared basic characteristics (including disease information) between individuals with and without MCI using t-test (for continuous variables) and chi-square examination (for discrete variables), and calculated the prevalence of MCI in the whole sample and in each subgroup.
Stepwise logistic regression model was established to analyze the predictive factors of developing MCI, with basic characteristics included as independent variables and covariates. Age was treated as a continuous variable and the others were treated as categorical variables. For disease information, the answer “yes” was coded as “1” while “no” was coded as “0”, and “male” was coded as “1” while “female” was coded as “2”. Other categorical variables were coded in order as well. Box-Tidwell tests were applied to examine the linearity of age as a continuous variable in the logit fitting processes before establishing the model, and Hosmer and Lemeshow Tests were conducted to test the model goodness-of-fit (Draper & Smith, 1998).
All analyses were performed using the Predictive Analytics Software Statistics, version 18, and a two-sided p value less than .05 were considered statistically significant.
Results
Characteristics of the Participants
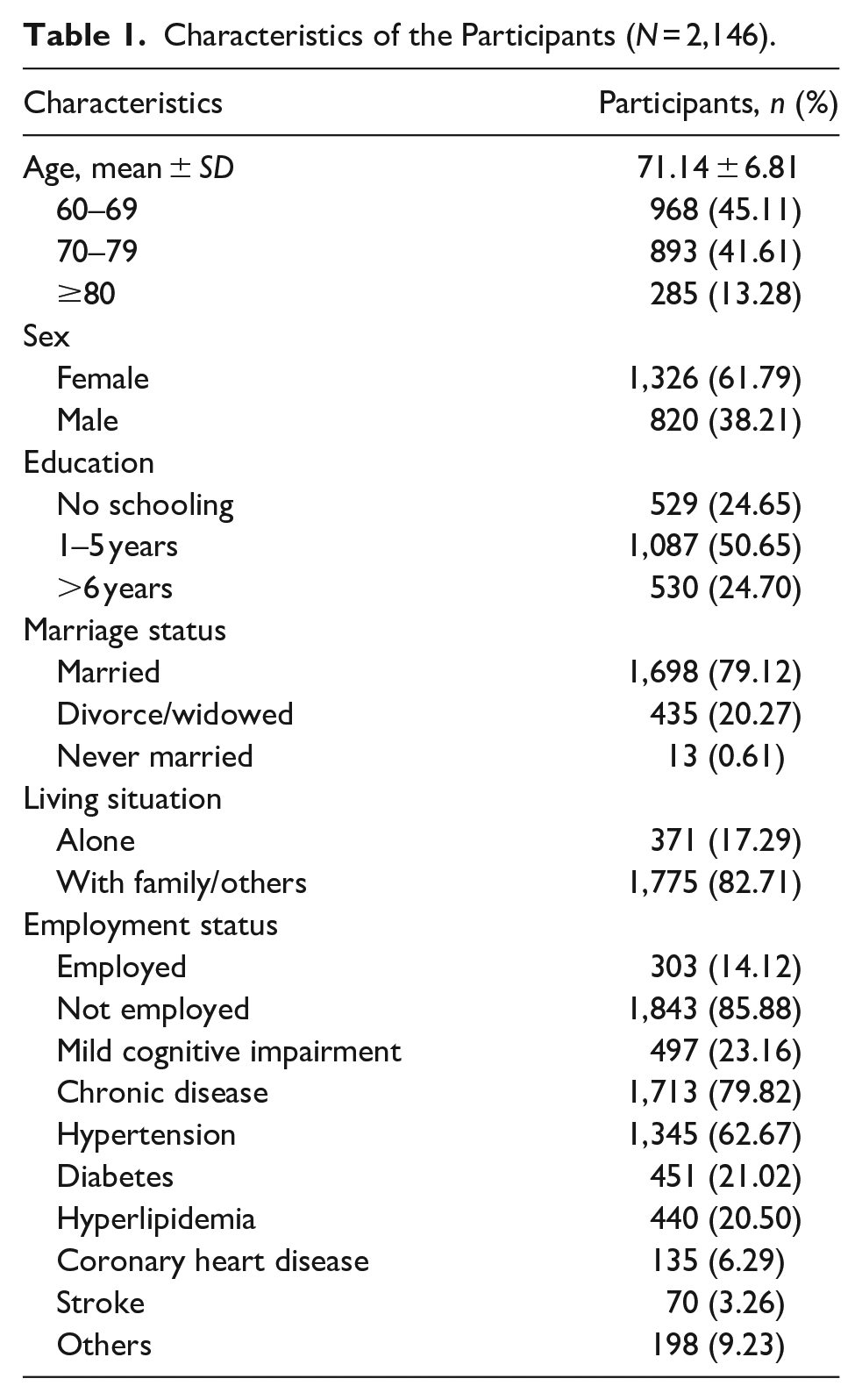
As depicted in Figure 1, a total of 2,146 participants were entered into the analysis. Table 1 indicates the demographic and clinical characteristics of the sample. Overall, their mean age (±SD) was 71.14 ± 6.81. Women constituted 61.79% of the sample, while 79.12% were married and 82.71% lived with family or others. 75.30% of the sample had fewer than 6 years of education, and the percentage of those who were not employed was 85.88%. Additionally, the prevalence of MCI in the sample was 23.16%, while 79.82% of individuals investigated had at least one kind of chronic condition.
Characteristics of the Participants (N = 2,146).
The Prevalence of MCI in Subgroups
The prevalence of MCI in subgroups was demonstrated in Table 2. 57.74% of those aged 80 or more had MCI, which rate was more than quadruple compared to that in the age group of 60 to 69. In addition, more than half of those affected by MCI had never received education, which proportion for those receiving at least 6 years of education was less than one-tenth. Furthermore, sex (χ2 = 18.56, p < .001), marriage status (χ2 = 62.55, p < .001), living situation (χ2 = 33.98, p < .001) and employment status (χ2 = 11.51, p = .001) were also significantly associated with MCI, and the prevalence in those with chronic conditions, except hypertension and hyperlipidemia, was significantly higher than in those without.
The Prevalence of MCI in the Sample and the Subgroups.

Note. MCI = mild cognitive impairment; CN = cognitive normal.
The Predictive Factors of MCI
Before doing the logistic regression analyses, the Box-Tidwell tests indicated acceptable linearity of age as a continuous variable in the logit fitting processes, which supported the linearity assumption of establishing the logistic regression model.
The Hosmer and Lemeshow Test for the goodness-of-fit of the logistic regression model had a χ2 = 13.30, df = 8, p = .102 > .05, indicating a good fitness of this model. Estimates from the logistic regression were listed in Table 3. Age, education, diabetes, coronary heart disease and stroke were significant predictive factors of MCI in the sample, while the significance of coronary heart disease was marginal. The odds ratios of the variables implied that individuals with diabetes, coronary heart disease and stroke were at 1.35, 1.50, 2.14 greater odds respectively of developing MCI compared to those without.
Estimates From Logistic Regression Modeling Mild Cognitive Impairment.

Discussion
As the health of the rural population improved and life expectancy lengthened, the burden of mental health increased. Nearly 5% of rural residents aged over 60 in China had a diagnosis of depression (Zhong et al., 2020), and the lifetime prevalence of suicidal ideation and attempt in the population was found to be 28.9% and 5.3%, respectively (Chiu et al., 2012). Moreover, the disability rate in rural older population was 10.9%, more than two times higher of 4.7% found in urban area (L. Ma et al., 2017). However, very few studies have been conducted on this left-behind area.
The purposes of the present study were to investigate the prevalence of MCI in older adults aged over 60 in rural China, and identify its associated risk factors. The principal finding of the study is that 23.16% of the investigated group had MCI. This rate is significantly higher than that reported in urban area of about 13% to 14% (Deng et al., 2021; Xue et al., 2018). Although the situation in rural area is serious, medical resources here is insufficient and the health care system is not adequately prepared to screen, identify and manage the cognitive disorder. More studies focusing on the cognitive conditions in this population are recommended and efficient approaches should be provided to bridge the gap.
In addition to the high prevalence, we also found that women, those with older age, lower education, never married, living alone, and not employed were more likely to develop MCI. These characteristics highlighted were consistent with what reported in previous studies (X. Li et al., 2013; Ren et al., 2018), and the finding would be helpful to deliver targeted services for individuals at risk of neurodegenerative diseases.
Although nearly all the demographic and clinical characteristics collected were significantly associated with MCI, results of the stepwise logistic regression model indicated that only age, education as well as the diabetes, coronary heart disease, and stroke were significant predictive factors of MCI in the sample, while the significance of coronary heart disease was marginal. Hypertension, which was traditional believed as an important associated factor of cognitive disorders, was tested with no significant association with MCI. Benefit from the reform on chronic disease management in China, the cardiovascular effect of hypertension on neurodegenerative disorders is supposed to be narrowed as most older adults with hypertension currently are under standard management and regularly taking anti-hypertension drugs.
Several studies have suggested chronic medical conditions as crucial risk factors of cognitive impairment (CI). Actually, estimated more than 80% of older adults aged over 65 have at least one chronic condition, and almost 80% of deaths in China in people aged 60 years are from chronic non-communicable diseases (Yang et al., 2013). A previous study demonstrated that chronic kidney disease is associated with elevated risk for dementia in elderly people with poor executive function, cognitive function, memory and language ability (Kurella et al., 2005). Singh and colleagues’ study found that a diagnosis of chronic obstructive pulmonary disease is associated with an increased risk for MCI, particularly non-amnestic MCI (Singh et al., 2014). In the present study, we found that rural older adults with chronic medical conditions are at 1.35~2.14 greater odds of developing MCI compared to those without, after controlling for sex, age, and other associated variables.
As a prevalent mental illness in the elderly, MCI commonly co-occurs with chronic medical illnesses and would interact in complex ways to increase the severity, impede treatment, and worsen the outcomes of both disorders. Faced with the challenge, integrated care approaches to manage MCI and comorbid medical conditions simultaneously in primary care settings are recommended. Evidence suggests that patients may be more engaged when mental illness is integrated into care for physical health than other forms of care provision (Katon et al., 2010), and effectiveness of such approaches have been extensively tested in Western countries (Katon et al., 2006; Smith et al., 2007), but rare studies were conducted in low and middle-income countries, including China, to examine the validity and feasibility of the integrated care. The outcomes of our study support the need to integrate the management of MCI into chronic disease management in rural China.
The strengths of the study include the large sample investigated and standard procedure and criteria of diagnosis. However, the study has limitations. The sample was from one town in rural Zhejiang Province, so our findings may not be generalizable to urban or other rural areas. The data in this study were cross-sectional, which limited the analysis of the long-term associations between demographics, comorbidities and MCI. Longitudinal studies would help to sort out the relationship between these conditions. Finally, we did not have data about prescribed treatment or adherence to treatment for diseases, and cognitive performance could be influenced by the use of those drugs. We acknowledge that medication use can potentially confound the results.
In conclusion, our investigation adds new evidence to the literature on the burden and risk factors of MCI in rural China. The prevalence of MCI in this group is high, and the prevalence of MCI was significantly higher in women, those with older age, lower education, never married, living alone and not employed. Age, education and chronic diseases were significant predictive factors of MCI in the sample, while the significance of hypertension was marginal.
Footnotes
Acknowledgements
We thank all the participants in the study, and we are also grateful to primary care physicians and research assistants who participated in the study for their assistance in research coordination and data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the China Postdoctoral Science Foundation, grant number: 2020TQ0265, and the Natural Science Foundation of Zhejiang Province, China, grant number: LGF21C090002.
Ethical Statement
The study was approved by the Academic Review Board of Zhejiang University Department of Psychology, approval number: [2021]027.