
Abstract
Introduction
Light-moderate alcohol consumption in old age has been associated with higher cognition and lower dementia risk (Peters et al., 2019). A meta-analysis of 15 prospective studies with a follow up of 2–8 years indicated that older adults who were ever alcohol drinkers had a 47% lower risk of any dementia when compared to nondrinkers (Anstey et al., 2009). Conversely, high alcohol consumption and binge drinking is associated with increased dementia risk (Kivimaki et al., 2020). An association between alcohol consumption over the life course and dementia risk has been found in older adult populations in the United States (Mukamal et al., 2003) and in several European countries including England (Sabia et al., 2018), Sweden (Handing et al., 2015), and Finland (Jarvenpaa et al., 2005).
Older adults who are light-moderate alcohol consumers tend to be in better health than abstainers and have a lower risk of health conditions associated with dementia such as diabetes (Polsky & Akturk, 2017) and cardiovascular diseases (Goel et al., 2018). Also, older adults often consume alcohol while in social settings (Nicholson et al., 2017), which may have benefits for cognitive functioning (Penninkilampi et al., 2018). Finally, while not reported in all studies (Paul et al., 2008), older adults who consume light-moderate amounts of alcohol have, on average, larger hippocampal volume (Downer et al., 2015) and less brain atrophy (Enzinger et al., 2005) than abstainers.
Most evidence on the relationship between alcohol consumption and dementia is based on older non-Hispanic white adults and less research has considered older Hispanic populations in the United States. The Hispanic population is the fastest growing population in the US with over 55 million people, of which nearly 10% are over the age of 65 (Noe-Bustamante et al., 2019). Most Hispanics living in the US are of Mexican descent (36.6 million) (Noe-Bustamante & Flores, 2019). Overall, the percentage of Hispanics who report drinking alcohol is similar or lower than non-Hispanic whites and other racial and ethnic groups (Caetano et al., 2014; Delker et al., 2016). However, among current drinkers, Hispanics are more likely to report heavy alcohol consumption and binge drinking than other racial and ethnic groups (Caetano et al., 2014; Delker et al., 2016).
About 12% of older Hispanic adults are diagnosed with the dementia, the highest proportion among different ethnic groups in the US. Alcohol consumption among older Hispanics has been associated with dementia risk. An analysis of 1,634 participants of the Sacramento Area Latino Study on Aging indicated that having two or more drinks per week and less than two drinks per week was associated with 0.55 and 0.64 lower risk for dementia, respectively compared to never drinking (Zeki Al Hazzouri et al., 2011).
Given that Mexican-Americans have longer life expectancy than other racial and ethnic groups (Markides & Eschbach, 2005), it is expected that a large proportion of this population will reach an age that puts them at a high risk of developing dementia. The objective of this analysis is to examine the association between late-life alcohol consumption and 10-year incident dementia among older Mexican-Americans. Our hypothesis is that late-life alcohol consumption will be associated with lower dementia risk when compared to life-long abstainers.
Methods
Data and Sample Selection
This is a longitudinal analysis of waves 5 (2004/05) – 8 (2012/13) of the Hispanic Established Populations for the Epidemiologic Study of the Elderly (H-EPESE) (Markides et al., 1997). The H-EPESE is a cohort of older Mexican-Americans residing in the southwestern US. The baseline wave was completed in 1993/94 and included a cohort of 3,050 participants that were representative of Mexican-American adults aged 65 and older living in Texas, New Mexico, Colorado, California, and Nevada. Participants have been re-interviewed approximately every two to 3 years. At wave 5 (2004/05) a new, representative cohort of 902 participants aged 75 and older was recruited into the H-EPESE. The most recent observation wave (Wave 10) was completed in 2020/21.
A total of 2,069 participants were interviewed at wave 5 (our baseline). Figure 1 presents the selection of the final sample. We excluded 591 participants who we classified as having dementia at baseline (see Measures). Among the 1,478 participants without dementia at baseline, we excluded 223 participants with missing information for one or more of our variables of interest. Our final sample size was of 1,255 participants with a mean of age of 81 years. Of the 223 participants excluded for missing information, 161 were only missing on household income. We repeated the analyses without considering income, which increased the sample size to 1,416 participants. The results from these sensitivity analyses were very similar to the main analyses (results available upon request). Flow chart of the selection of participants from the hispanic established populations for the epidemiologic study of the elderly.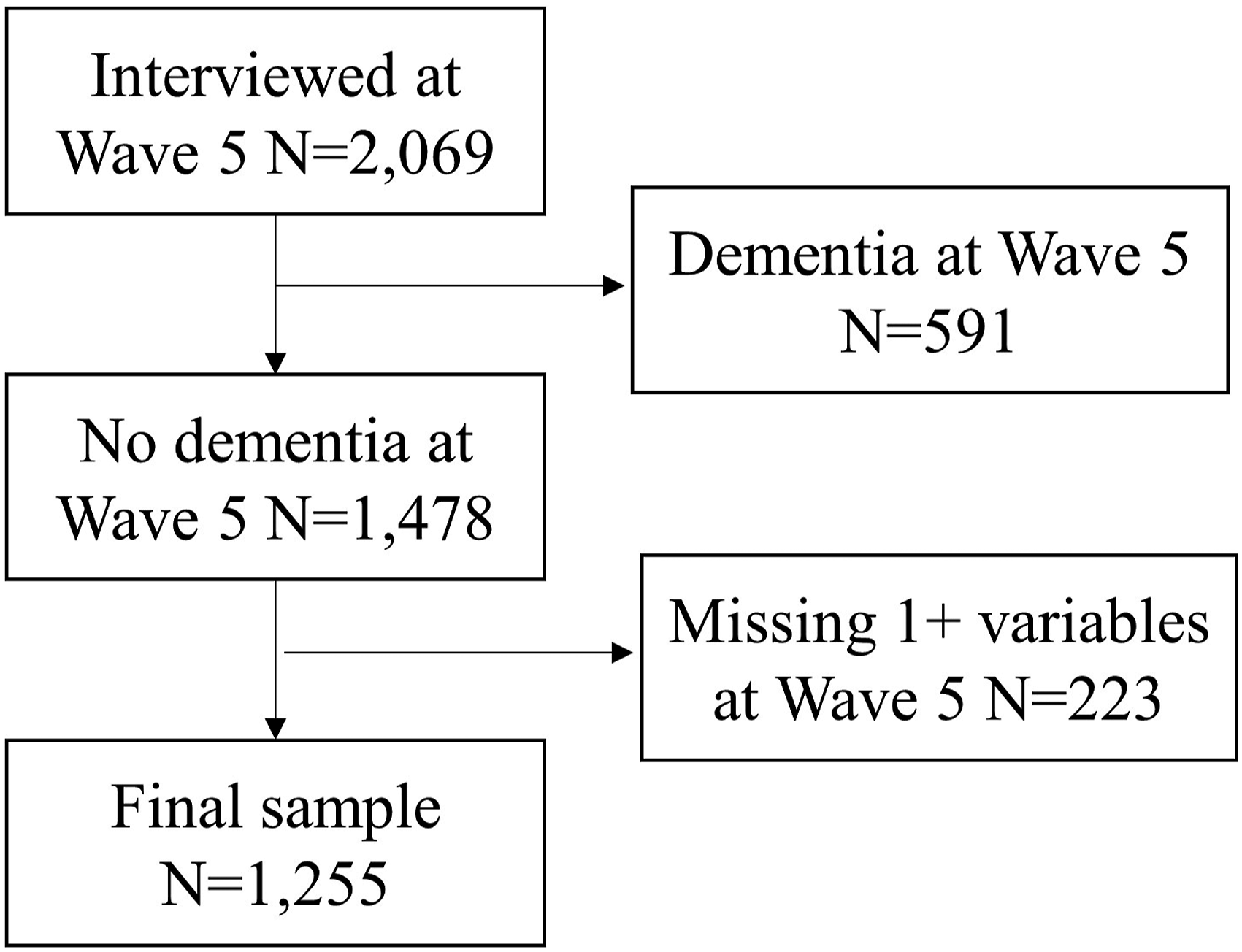
Measures
Late-Life Alcohol Consumption
H-EPESE participants are asked questions about their past and current alcohol consumption. Participants are first asked “Have you ever drunk any type of alcohol (beer, wine, liquor) in your entire life?” Participants who respond “yes” are then asked, “In the past month, have you had any beer, wine or liquor?”. We used these two questions to categorize participants as life-long abstainers, former drinkers, and current drinkers.
Dementia
Participants’ cognitive functioning is assessed using the Mini-Mental Status Examination (MMSE). The MMSE measures orientation, attention, memory, language, and visual-spatial skills (Folstein et al., 1975). The H-EPESE survey does not include a proxy measure of cognitive functioning, but the proxy interview does ask if the participant has ever been diagnosed with dementia by a physician. We defined dementia as scoring 18 points or lower on the MMSE or a proxy-reported diagnosis of dementia by a physician (Downer et al., 2019).
Covariates
Selected covariates included demographic characteristics and self-reported health conditions. The demographic variables were age, sex, years of education (none, 1–5 years, or 6+ years), yearly income ($0–14,999 or $15,000+), and language of interview (English or Spanish). We also created a variable that indicated if a participant was U.S.-born or migrated to the US in early (age ≤19), mid (age 20–49), or late (age ≥50) life.
Self-reported health conditions included diabetes mellitus, stroke, and hypertension. Participants with a previous diagnosis of diabetes mellitus were also asked if they currently use insulin. Insulin use can be a proxy for diabetes severity (Campbell, 2009). Diabetes mellitus was categorized as no diabetes, diabetes but not using insulin, and using insulin.
Statistical Analysis
The demographic and health characteristics according to late-life alcohol consumption status were described using chi-squared tests and analysis of variance for categorical and continuous variables, respectively.
The association between alcohol consumption status and dementia risk was assessed using Cox proportional hazards models. Participants who were never classified as having dementia by the time of their last observation wave or after 10-years were censored. Visual inspection of the scaled Schoenfeld residuals according to follow-up time indicated that no variables in our analyses violated the proportional hazards assumption.
We first modeled the unadjusted association between alcohol consumption and incident dementia. Model two adjusted for demographic characteristics. Model three adjusted for demographic and health characteristics. The analyses were done using Stata/SE version 15 and R (R Core Team, 2021).
Results
Demographic and Health Characteristics of Mexican American Adults Aged 75 and Older According to Late Life Alcohol Consumption Status.

*p-values based on analysis of variance for continuous variables and chi-square tests for categorical variables. Percentages are based on the column totals for the number of participants.
Cox Proportional Hazards Regression Models For The Unadjusted And Adjusted Association Between Late Life Alcohol Consumption Status And 10-Year Dementia Risk Among Mexican American Adults Aged 75 And Older.

*p<0.05; **p<0.001. HR (hazard ratio); CI (confidence interval).
Model three also shows statistically significant associations between older age, no education, low income and completing the interview in Spanish with higher risk of dementia. Women had 27% lower risk of dementia compared to men (HR = 0.73 95% CI = 0.57–0.93). Participants with diabetes mellitus who used insulin had a 1.71 times higher risk of dementia when compared to those without diabetes mellitus (HR = 1.71 95% CI = 1.15–2.55).
Discussion
Our objective was to estimate the 10-year risk for dementia among Mexican-Americans aged 75 and older who were current alcohol consumers and former alcohol consumers compared to life-long abstainers. Current alcohol consumers had a significantly lower risk for dementia over a 10 year period than life-long abstainers. The difference in dementia risk between former alcohol consumers and life-long abstainers was not statistically significant. Our findings are consistent with evidence from other older adult populations that alcohol consumption in late life is associated with lower dementia risk.
There are several plausible explanations for the protective association of late-life alcohol consumption on dementia. First, healthy older adults may continue drinking alcohol throughout adulthood whereas older adults with chronic conditions may limit or reduce their alcohol consumption (Britton & Bell, 2015). Socioeconomic factors may also contribute to the protective association of alcohol on dementia risk. Older Hispanics with high educational attainment and who are employed are more likely to consume alcohol than their lower socioeconomic status counterparts (Castaneda et al., 2019). However, our results showed the association between current drinking and lower dementia risk remained statistically significant after adjusting for socioeconomic factors. The context in which a person consumes alcohol may influence dementia risk. However, the H-EPESE and similar population-based cohort studies of aging do not include questions on the context in which a participant consumes alcohol. Our analysis could not determine if social engagement, drinking socially versus in isolation, and other contextual factors associated with both alcohol consumption and dementia explain our finding for lower dementia risk among current drinkers.
An important contribution of our study is that we were able to differentiate between late-life abstainers who previously consumed alcohol and life-long abstainers. We found that former drinkers had lower but non-significant risk for dementia. Other studies have reported that former drinkers are at greater risk for dementia compared to life-long abstainers (Mukamal et al., 2003). Data limitations that preclude identifying older adults who are former alcohol consumers may contribute to the protective association between current alcohol consumption, dementia, and cognitive decline (Roizen et al., 2013).
A limitation of our analysis is the H-EPESE survey does not ask participants about the frequency or amount of alcohol typically consumed. This prevented us from differentiating between current alcohol consumers who are light, moderate, or heavy consumers according to the number of days per week in which the person drinks alcohol or the number of drinks typically consumed. The H-EPESE survey also does not include separate questions for wine, beer, and liquor consumption. Using separate questions can contribute to more accurate reporting of alcohol consumption (Embree & Whitehead, 1993). Finally, the H-EPESE survey uses a 1-month reference period for alcohol consumption whereas other studies have used a 1-week reference period (Barnes et al., 2009; Britton et al., 2004). A 1-month reference period can more accurately reflect a person’s typical drinking behavior than when asking participants on alcohol consumption in the past week (Dawson, 2003), but longer reference periods are prone to recall bias (Greenfield & Kerr, 2008). A long reference period also does not allow for participants to be asked about the frequency, number of drinks, and types of alcohol consumed (Dawson, 2003).
A second limitation is that our classification of dementia was based on the MMSE or a proxy report of a dementia diagnosis. The MMSE has well known limitations for detecting dementia and cognitive impairment (Mitchell, 2009). Cultural biases in cognitive testing and in the diagnosis of dementia can contribute to Hispanic older adults to have a missed or delayed diagnosis of dementia (Manly, 2008). The stigma of dementia in Hispanic culture may also keep a person from reporting that their family member is living with dementia (Gray et al., 2009). These limitations may have resulted in our analysis under-estimating the incidence of dementia in our sample.
Finally, the H-EPESE only includes participants who are Mexican-American. This limits the generalizability of our findings to other Hispanic populations in the US due to demographic and social differences between Hispanic sub-groups. For example, Mexican-Americans tend to have higher rates of alcohol consumption compared to Cuban Americans and South or Central Americans (Caetano et al., 2009).
Conclusions
Our findings are new evidence for the association between late life alcohol consumption and dementia risk among Hispanic older adults. Consistent with findings from other populations, we observed that current alcohol consumers, but not former alcohol consumers had lower dementia risk compared to life-long abstainers. Continued research is needed to identify pathways that contribute to the potential protective association between late life alcohol consumption and dementia for Hispanic and non-Hispanic older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health, National Institute on Aging (P30AG024832, P30AG059301, R01AG010939, and RF1AG068988).