
Abstract
The COVID-19 pandemic has disrupted lives globally but disproportionately affected older adults due to their increased vulnerability to severe illness and higher mortality. To protect older adults from infection, community members in rural Kenya have ensured enhanced adherence to COVID-19 containment measures. However, while restricted social contact is highly recommended in the control of COVID-19 infection, limited research exists on its effect on the psychosocial wellbeing of older adults. This study therefore assessed the relationship between community adherence to COVID-19 containment measures and the overall wellbeing of older adults. Nyeri County in Central Kenya was selected for the study and all adults aged 70 years and above targeted. Snowball sampling was used to collect data from a sample of 360 respondents. Both descriptive and inferential statistics were used in data analysis. The study established a significant inverse relationship between the level of community adherence to COVID-19 protocols and the wellbeing of older adults. Furthermore, the wellbeing of most older adults had deteriorated during the pandemic, with older married women with higher incomes being less affected. The study concluded that although the COVID-19 pandemic had affected everyone, effective containment is a multi-dimensional issue that requires targeted interventions.
Introduction
Research has established that the severity of COVID-19 complications is related to age and other underlying health conditions (Adhikari et al., 2020; Yi et al., 2020). According to Bajaj et al. (2021), aging causes numerous biological changes in the immune system, which are linked to age-related illnesses and susceptibility to infectious diseases. Hence, due to their advanced age and weakened immunity, older adults are more likely to experience severe complications or even death if they contract COVID-19. Restricted social contact is among the safest measures against COVID-19 as it limits transmission between people (Quaife et al., 2020). However, overall wellbeing is multi-dimensional and requires not only physiological health but also social, psychological and financial wellbeing (Thuku, 2016). Furthermore, other factors including socio-demographic characteristics could intervene in the relationship resulting in varying levels of wellbeing among older adults of different ages, gender, marital status, education and income (Bender, 2004; Donaldson et al., 2010; Nzabona, 2014; Wong & Earl, 2009). Protecting the older adults from the COVID-19 infection while ensuring their overall wellbeing therefore demands much more than physical distancing, emotional support by significant others and appropriate policy decisions.
Like most developing countries, modernization and urbanization has moved many young people in Kenya to urban areas in search for jobs, leaving behind many older adults in rural areas where kinship bonds are still quite strong. Hence, when the first COVID-19 infection case was reported in Kenya and stringent containment measures that restricted social contact between persons were introduced (Ministry of Health [MoH], 2020; Tyce, 2020), social life for older adults may have been affected. This is because, the COVID-19 control measures required community members to restrict physical contact amongst themselves and be extra careful in the presence of older adults in order to protect them. Consequently, the containment measures not only lead to a reduction in physical contact but could also have created a perception of emotional distance between the older adults and community members.
As advanced by prior research, the overall wellbeing of older adults is positively related to the quality of social support, health and economic conditions (Maina & Mugenda, 2013; Ondigi & Mugenda, 2011; Thuku, 2019). However, the restricted social contact required in the containment of COVID-19 pandemic imply that individuals must ensure physical distance from the older adults in order to protect them. Yet, both psychosocial and health wellbeing are critical for the overall wellbeing of older adults. According to World Health Organization (WHO, 2020), prolonged periods of isolation could have serious effect on the mental health of older persons. In addition, Lekamwasam and Lekamwasam (2020) observed that some COVID-19 policies and containment measures may have profound negative effects on the mental health of older populations, an indicator that overall wellbeing could be affected. As explained by Macdonald and Hülür (2021), social distancing measures during COVID-19 presented a major stressor for older adults’ wellbeing. However, Birditt et al. (2021) found that older people reported less pandemic-related stress than younger ones, an indicator that research on the effect of COVID-19 on the mental wellbeing of older adults is inconclusive. As Quaife et al. (2020) noted, limited research exists on the effects of COVID-19 on social contacts, hence a need for more studies. This study therefore assessed the relationship between community adherence to COVID-19 containment measures and the wellbeing of older adults in rural Kenya. To achieve this, the study was guided by the following specific objectives: i. To examine the level of adherence to the recommended COVID-19 containment measures by community members in Nyeri County, Kenya ii. To assess how the wellbeing of older adults was affected by community members’ adherence to COVID-19 containment measures iii. To examine the extent to which the wellbeing of older adults during the pandemic was related to their socio-demographic characteristics
Methodology
This study is a cross-sectional survey utilizing a mixed method approach. Nyeri County in Central Kenya was purposively selected for the study due to her high percentage of older adults (Thuku, 2019).
Sampling
The study targeted all residents of Nyeri County who had attained age 70 and lived among other community members. Age 70 years was selected because it qualifies the members for the financial stipend for older adults (Tanui, 2017). Since the monthly stipend is released through selected local banks at specific dates, beneficiaries from the same locality usually communicate through word of mouth or telephone calls to update each other on the issue. Hence, after the researcher and research assistant identified the first few potential respondents through the assistance of local religious leaders, other respondents were reached through referrals by those who had been interviewed. Thus, Snowball sampling was an appropriate and effective sampling technique.
To ensure gender representation, the target population was stratified into male and female. According to the Kenya National Bureau of Statistics (KNBS, 2019), Nyeri County has 42,212 persons aged 70 years and above, with females constituting about 60% of the target population. A sample size of 360 was determined based on Boomsma and Hoogland (2001) and the Sample Size Table. The ratio of 3:2 for female to male was observed, giving 216 female and 144 male respondents.
Measures
The outcome variable was ‘wellbeing of older adults’ while predictor variables were: i. Community adherence to COVID-19 Containment Measures ii. Socio-demographic characteristics (age, gender, marital status, education, income).
Socio-demographic data was collected quantitatively using closed-ended questions. Data on community adherence to COVID-19 protocols was collected qualitatively using open-ended questions while ‘wellbeing’ was measured both quantitatively using a Likert scale and qualitatively using open-ended questions, as described below:
Community Adherence to COVID-19 Containment Measures
Respondents were asked to describe the measures that the community members they regularly interacted with usually undertook to ensure their protection from COVID-19. Ranking was then done based on how many adherence measures were generally observed. In this case, those respondents whose community members generally undertook no extra measures (compared to the pre-COVID-19 period) were awarded a score = 1; those who observed one measure (score = 2); two measures (score = 3), three (score = 4) and four or more measures (score = 5).
Wellbeing
To determine subjective change in wellbeing, respondents were required to answer questions on a Likert Scale indicating whether various aspects of their wellbeing had improved, remained the same or deteriorated during COVID-19 pandemic. Scores were awarded as follows: improved = 3; unchanged = 2; deteriorated = 1. Respondents were also required to explain how their wellbeing in the financial, social, psychological, spiritual and health domains had been affected.
Socio-Demographic characteristics
Age was measured at categorical level and coded as follows: 70-74 = 1; 75-79 = 2; 80-84 = 3; 85-90 = 4; 90-94 = 5; 95 and above = 6.
Gender: male was given a code of ‘1’ and female coded ‘2’
Marital status: Initially coded as married = 1; single (never married) = 2; separated = 3; divorced = 4; widowed = 5. This was later recoded to married (currently living with spouse) = 1, and single (widowed + divorced + separated + never married) = 2, after finding out that the sample had zero respondents in the divorced, separated and never married categories.
Education was measured by asking the respondents to indicate the level of formal education reached. It was coded as follows: none = 1; primary = 2; secondary = 3; middle-level college = 4; university = 4.
Income was measured by asking respondents to estimate their average monthly income from all sources (in Kenya shillings) and was coded as follows: 10,000 and below = 1; 10,001-20,000 = 2; 20,001-40,000 = 3; 40,001-80,000 = 4; above 80,000 = 5
Data Collection Instruments
Interview schedules with both open and closed-ended questions were utilized. The interview schedule had three sections. The first section collected socio-demographic data through closed-ended questions. The second section had a Likert Scale while the third section had open-ended questions examining how the COVID-19 Pandemic had affected various domains of respondents’ wellbeing, and measures taken by community members in the control of COVID-19.
To ensure validity and reliability of the instruments, a pilot study was conducted on 20 older adults from Nyeri County who were not included in the actual study. Face and content validity of the data collection instruments was established through consultation with other researchers. After the piloting phase, a few statements were rephrased to enhance validity. Cronbach’s alpha was used to determine the internal consistency of items in the Likert Scale. An Alpha coefficient of 0.78 showed that the instrument was reliable.
Data Collection Procedure
Data was collected between June and July 2020 mainly via telephone calls due to the stringency of COVID-19 containment measures. However, a few face-to-face interviews under strict COVID-19 guidelines were conducted in cases where respondents were uncomfortable with telephone interviews. The researcher and a trained research assistant conducted the interviews and adhered to the ethical considerations of anonymity, confidentiality and informed consent.
Data Analysis
Quantitative data were analyzed descriptively using frequencies and percentages. Correlation and Multiple Regression Analysis were conducted to determine whether relationships existed between the variables of interest. Relationships were considered significant if p ≤ 0.05. Analysis of qualitative data was done by organizing into themes and triangulating with quantitative findings. A few direct quotes from respondents enriched the quantitative findings.
Results
Socio-Demographic Characteristics of Respondents.

As shown in Table 1, more than 40% of the respondents were found in the lowest age category of between 70–74 years. Only 1.9% were aged those aged 90 years and above. This is not surprising considering that the percentage of older persons in any population decreases as age increases due to natural attrition. Notable also is that female respondents constitute 60% of the total sample, corresponding to the general situation among older adult population where females are usually more than male.
Table 1 shows that 71.9% of the respondents were married at the time of the study. The rest were widowed with none being separated, divorced or never married. This reflects the strong African traditional values of marriage and remaining in the union until death, unless in very exceptional circumstances. Approximately 31.1% of the respondents had no formal education. Most of those without formal education were older females who had never been taken to school as young girls because traditionally, girls were expected to get married soon after reaching puberty and become fulltime homemakers.
Income levels were quite low, with 38.1% of respondents earning 10,000 Kenya shillings (KES) and below per month. Considering that 1USD≈113.6 KES at the time of study, the implication is that 38.1% of respondents earned less than 88 US Dollars monthly. Only 1.7% had a monthly income of above 40,000 shillings. Since all the respondents were above the retirement age of 60 years, the few who were previously engaged in formal employment still received monthly pension income. However, majority had been peasant farmers all their lives and still owned pieces of land where they practiced subsistence farming which contributed to their food and some income. The monthly stipend for older adults and financial support from their children were key sources of income.
Community Adherence to COVID-19 Containment Measures
Soon after the first case of COVID-19 infection was reported in Kenya on 13th March 2020, the government imposed stringent measures, including a ban on all public gatherings, frequent hand-washing, wearing of facemasks in public places, and avoidance of handshakes among other social distancing measures to control community spread of the virus.
Community Adherence to COVID-19 Containment Measures.

As Table 2 shows, only 11.7% of the respondents reported COVID-19 adherence levels of 0 (zero) from their community members. However, 68.9% indicated a high degree of community adherence where members observed at least two extra COVID-19 containment measures. The COVID-19 containment measures described by respondents included; assistance in setting up hand-washing stations for visitors at entry points to the home, hand-washing with soap and running water while entering the compound, reduction in frequency of visits, wearing of face-masks, keeping a safe distance away, and avoidance of handshakes and embraces among others. Hand washing and refraining from body contact such as handshakes and embraces were the most common. Based on the findings, the level of community adherence was quite high with more than half (52.2%) of them observing three or more containment measures.
COVID-19 Containment Measures and the Wellbeing of Older Persons
Based on research, social and physical distancing remains the best protection against COVID-19. However, for older persons some of whom depend on other people for survival, social distancing implies reduced social support that could negatively affect their wellbeing. Furthermore, both psychosocial and health wellbeing are critical for the overall wellbeing of older persons. The study therefore examined the effect of COVID-19 on various aspects of the wellbeing of older persons and used the findings to compute the variable ‘wellbeing’.
Effect of COVID-19 on the Various Domains of Respondents’ Wellbeing.

As shown in Table 3, none of the respondents reported an improvement in the financial and psychological aspects. However, an improvement was reported by 1.9% of the respondents in their social and spiritual wellbeing, and by 3.9% in their health wellbeing. The spiritual wellbeing largely remained unchanged for majority of the respondents (81.1%). As one respondent argued: ‘Although we are currently barred from attending church worship, we believe that God does not reside in churches and shall continue to pray in our homes and trust Him to end this pandemic.’
Although this paper does not explore in detail the effect of COVID-19 on specific indicators of each domain, the qualitative responses from the respondents implied some direct and indirect effects of the pandemic on their wellbeing. Among the common explanations for the deterioration in the financial wellbeing was that their children who supported them were having financial difficulties after losing their jobs or getting income reduction. Many said that it was also difficult for them as farmers to sell their farm products due to travel restrictions and fear of infection. Quoting from one respondent: ‘This pandemic has made some of my children lose their jobs in the city and others are unable to visit us due to travel restrictions. This has reduced the financial and material support they used to give us.’
Socially, many of them felt lonely due to reduced frequency of visits by their children and loved ones because of travel restrictions and/or financial constraints. In the words of one widowed respondent: ‘…We had to call off our annual family get-together that was scheduled for the Easter holidays due to COVID-19 restrictions. The get-together is very important for me and I always look forward to it. I have not met some of my children since COVID-19 struck. Nowadays even neighbours hardly come to visit and when they do, they cannot shake my hands or stay close to me…’
However, a few respondents felt more socially connected with their loved ones who had to work from home and called to check on them more regularly. Some reported that they had started using video calls to communicate with their children and grandchildren in urban areas. Citing a respondent in the lowest age category: ‘Although I have not had any physical contact with my daughter in Nairobi, she calls me more often than she did previously because she is now working from home. She has also bought me a smartphone which we sometimes use to video call each other. Seeing them on video calls makes me feel as if we are together.’
Psychologically, many respondents feared for their children in urban areas who were at the epicenter of COVID-19, or had lost their means of livelihood. Others were afraid of personally getting infected and thought about COVID-19 related deaths quite often. Those who had pre-existing medical conditions whose doctors were located in major cities had many of their medical appointments postponed due to travel restrictions and the need to avoid public places, making them worry about their health situation. One of the respondents explained: ‘Several of my medical appointments have been postponed and I am a bit worried about my health condition. My son who accompanies me for the check-up says it is better to avoid hospitals unless it is critical. However, a laboratory technician was sent here to take my blood samples. Although I was afraid of contact with someone from the city where the disease is spreading rapidly, I am relieved that my health condition is being monitored.’
In the health aspect, regular medical check-ups were not possible and they sometimes ran out of medication. Sometimes they had to bear minor medical issues silently for fear of going to hospital where they could contract COVID-19. However, some of them reported an improvement in their health due to the enhanced hygiene measures. One of the respondents reported that there were reduced cases of flu. Quoting his words: ‘It is as if coughs disappeared with the emergence of COVID-19. You hardly hear anyone coughing any more. I think frequent handwashing is good for us and should continue.’
Spiritually, faith in God remained unchanged for the majority of respondents. However, the inability to congregate in church due to closure of places of worship affected a few of them negatively and found themselves questioning God for the pandemic. A small percentage became more spiritual and prayed more often for the pandemic to end.
While it is understandable that strict measures were necessary to minimize the risk of older persons contracting the virus, it is probable that community adherence to containment measures may have had some effect on wellbeing. This is because most of the COVID-19 protection guidelines emphasize staying away from other people, some of whom are very essential to the wellbeing of older persons. Hence, the variable ‘wellbeing’ was computed to allow for statistical analysis.
Computing the Variable ‘Wellbeing’
The variable ‘wellbeing’ was computed by awarding scores to the respondents’ responses on whether their wellbeing in each of the five domains (financial, social, psychological, spiritual and health) had: improved, remained the same or deteriorated (refer to Table 3).
Distribution of Respondents based on their Wellbeing Scores.

According to Table 4, respondents’ scores across wellbeing measures ranged from 5–9, indicating that all respondents experienced deterioration in one or more dimensions of wellbeing. Although some level of deterioration in wellbeing would not have come as a surprise considering the reduced social contact and financial resources, the magnitude shown in Table 4 was not expected. The study therefore examined whether the deterioration in wellbeing could be related to COVID-19 containment measures.
Relationship Between Community Adherence to COVID-19 Measures and the Wellbeing of Older Adults
Correlation between Community Adherence to COVID-19 Measures and Wellbeing of Older Adults.

** Correlation is significant at the 0.01 level (2-tailed).
As shown in Table 5, the Pearson Correlation Coefficient was significant (p < 0.05) with a value of −0.284 implying a significant but inverse relationship. Although the relationship is a bit weak, the results indicate that an increase in community adherence to COVID-19 measures led to a deterioration in the wellbeing of older persons. As observed from qualitative findings, protecting the older adults from COVID-19 required that community members reduce their visits, observe recommended physical distance, and wear facemasks around them. This could have reduced social contact and the perception of social support, making the older adults feel socially isolated.
Relationship Between Wellbeing and Socio-Demographic Characteristics
Multiple Regression Analysis on the Relationship between Wellbeing and Socio-Demographic Factors.
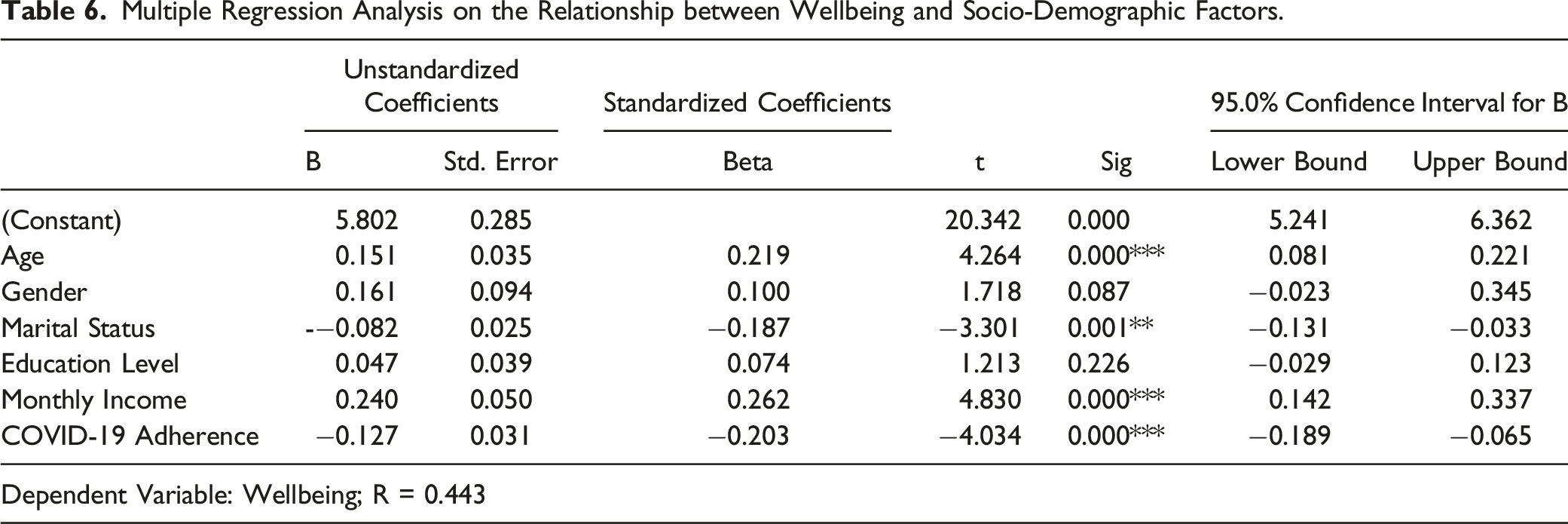
Table 6 shows that the wellbeing of older adults was positively related to their age, monthly income, and marital status. Community Adherence to COVID-19 Measures had a significant but inverse relationship with the wellbeing of older adults. However, gender and education were not significant predictors of wellbeing (p > 0.05).
As Table 6 shows, age was positively but weakly related to the level of wellbeing (p < 0.05), implying that the older one was, the less their wellbeing had deteriorated during the pandemic. This could be because the older one got, the easier it was to accept things beyond ones control and probably decided to live 1 day at a time.
Monthly income was also positively related to the level of wellbeing (p < 0.05), implying that the wellbeing of those with higher incomes deteriorated less than that of those with lower ones. This was probably because higher incomes enabled individuals to cater for their needs and even protect themselves better, hence giving them a sense of security.
Marital status was significantly related to the level of wellbeing (p < 0.05). A cross-tabulation conducted on the relationship between wellbeing and marital status showed that those who were married generally had a higher level of wellbeing than those who were single/non-married.
Relationship between Financial Wellbeing and Socio-Demographic Factors.

As shown in Table 7, financial wellbeing of older adults was positively related to their age and income, and inversely related to education level. Table 7 also shows that financial wellbeing was significantly related to gender. A cross-tabulation conducted on the relationship between gender and financial wellbeing established that female respondents generally had a higher financial wellbeing than the male ones. However, despite 96.1% of respondents having reported that their financial situation had deteriorated during the pandemic (refer to Table 3), the study did not find a significant relationship between community adherence to COVID-19 measures and financial wellbeing.
Relationship between Social Wellbeing and Socio-Demographic Factors.
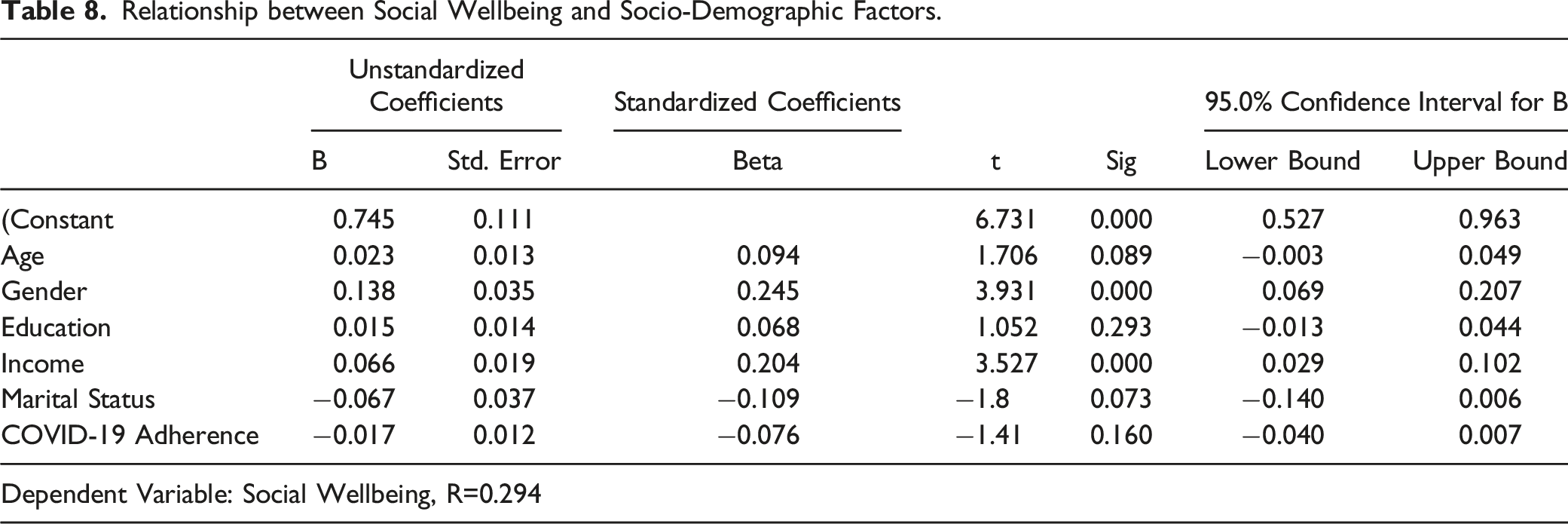
Table 8 shows that social wellbeing of older adults was significantly related to their gender and income. A positive relationship was found between social wellbeing and income while cross-tabulation results on gender and social wellbeing showed that female respondents generally scored higher than the male ones. Despite 98.1% of respondents reporting that their social wellbeing had deteriorated during the pandemic (Table 3), the regression analysis did not establish any significant relationship between community adherence to COVID-19 measures and social wellbeing.
Relationship between Health Wellbeing and Socio-Demographic Factors.

Relationship between Spiritual Wellbeing and Socio-Demographic Factors.

Table 10 shows a significant relationship between the spiritual wellbeing of respondents and their age, income, marital status and community adherence to COVID-19 measures. The relationship between spiritual wellbeing and both age and community adherence to COVID-19 measures was positive, while that between spiritual wellbeing and income was inverse. A cross-tabulation conducted to determine the nature of the relationship between spiritual wellbeing and marital status showed that married respondents generally had lower scores than the non-married.
It was not possible to conduct a regression analysis on the relationship between psychological wellbeing and socio-demographic characteristics because all respondents (100%) had reported a deterioration in their psychological wellbeing during the COVID-19 pandemic.
Discussion
This study assessed the relationship between community adherence to COVID-19 measures and the wellbeing of older persons. The findings of this study show that community members in Kenya had high adherence levels to the COVID-19 containment measures and seriously took the responsibility of ensuring adequate protection for older persons. However, the study established a significant inverse relationship between the level of community adherence to COVID-19 containment measures and the wellbeing of older persons. This may be an implication that while community members were trying their best to protect the older members, an unintended effect of their goodwill may have been a deterioration in the wellbeing of older persons. Although this study did not examine whether the deterioration in wellbeing was directly linked to community adherence to COVID-19 protocols, the findings concur with Macdonald and Hülür (2021) who reported that social distancing measures were major stressors for older adults’ wellbeing. Hence, a critical review on how to strike a balance between health and other needs of older adults during the COVID-19 pandemic may be necessary with the goal of enhancing overall wellbeing.
To enable targeted interventions, the study examined the relationship between wellbeing and socio-demographic characteristics and found that the effect of COVID-19 on the wellbeing of older persons was significantly related to their age, marital status and income. Although the relationship between age and wellbeing was rather weak, it was significant and positive. This implies that the older one was, the less their wellbeing had deteriorated during the COVID-19 pandemic. This was probably because as one got older, he/she found it easier to accept the challenges encountered in life and appreciate each day at a time. The findings concur with Mroczek (2001) who attributed higher emotional stability in old age to fewer negative emotions when compared to younger people. Birditt et al. (2021) also found that older people reported less pandemic-related stress than younger ones.
The amount of monthly income was positively related to the level of wellbeing. This was probably because higher incomes enabled individuals to cater for their needs, including COVID-19 protective measures better than those who earned less. The findings correspond with previous studies, which reported a significant positive relationship between income and life satisfaction among older adults (Donaldson et al., 2010; Wong & Earl, 2009).
Marital status was significantly related to the level of wellbeing. A cross-tabulation conducted on the relationship between wellbeing and marital status showed that those who were married had a higher level of wellbeing than those who were single (non-married at the time of study). This compares to findings by Birditt et al. (2021) who established that non-married individuals reported greater pandemic-related stress than married ones. Reduced deterioration in wellbeing among the married individuals may be due to the psychosocial support that spouses give each other despite the social distancing requirement for COVID-19 containment. Prior research had also established that married persons reported better mental health outcomes and happiness than unmarried ones (Kim & Moen, 2001; Maina & Mugenda, 2013; Nzabona, 2014; Wong & Earl, 2009).
Regression analysis conducted on individual measures of wellbeing found financial wellbeing to be positively related to respondents age and income, but inversely related to their education level. Financial wellbeing was also significantly related to gender where female respondents generally had higher financial wellbeing than the male ones. The higher financial wellbeing in older respondents with higher incomes points to the critical role of income on financial security and the resultant wellbeing. In addition, Birditt et al. (2021) had established that older adults reported less pandemic-related stress than younger ones. Hence the older one was, the easier it was to cope with any deterioration in finances during the pandemic. The study findings where female respondents had higher financial wellbeing than the male ones correspond to those by Liu et al. (2021) who reported that older adult women have lighter economic worries than men particularly if they are not the primary bread winners. An inverse relationship between education and financial wellbeing could probably be because those who were more educated may have been engaging in other income-generating activities that could have been negatively affected by the COVID-19 restrictions, hence higher deterioration in financial wellbeing.
Social wellbeing was found to be significantly related to income and gender where older female adults with higher incomes had a higher wellbeing than the male ones. This corresponds to prior research where older females have stronger social support networks than the male (Liu et al., 2021) hence higher social wellbeing (Bender, 2004). In addition, prior studies have established a significant positive relationship between income and life satisfaction among older adults (Donaldson et al., 2010; Wong & Earl, 2009).
Health wellbeing was positively related to respondents’ income and inversely related to community adherence to COVID-19 measures. A positive relationship between health wellbeing and income could be attributed to the enhanced ability of high income earning individuals to afford quality health-care including private access despite the challenges posed by the pandemic. As observed by Thuku (2016), even in cases where health challenges arise, those with adequate financial resources can afford medical care and live a more comfortable life than those without. High level of community adherence to COVID-19 measures could have negatively affected the health of older adults due to stress-related health complications and increased difficulty to access quality health-care. It is possible that the significant inverse relationship observed between community adherence to COVID-19 measures and overall wellbeing was mainly driven by the negative effect of community adherence on the health domain.
Spiritual wellbeing was found to be positively related to age and community adherence to COVID-19 measures. The positive relationship between age and spiritual wellbeing concurs with prior research which shows that older adults tend to be more religious and spiritual than younger ones and that religiosity can increase with age (Bengtson et al., 2015; Malone & Dadswell, 2018). The positive relationship between community adherence to COVID-19 measures and spiritual wellbeing could be attributed to enhanced search for divine intervention to end the COVID-19 pandemic. As observed by Mackinlay (2015), spirituality is supportive in coping with the challenges associated with ageing.
The observation where spiritual wellbeing was lower for married older adults with higher incomes than other categories may be explained by Malone and Dadswell (2018) who found that spirituality promoted positive ageing during challenges through intrinsic coping mechanisms. Hence, those experiencing challenges such as low income and lack of spousal support are likely to become more spiritual in the search for divine strength, comfort and hope thus the higher spiritual wellbeing.
Conclusion
The findings show that the overall wellbeing of all older persons in Nyeri, Kenya had deteriorated during the COVID-19 pandemic. The inverse relationship between community adherence to the COVID-19 containment measures and the wellbeing of older adults is a significant observation with important policy implications. It means that while community members were trying their best to protect the older members, one unintended consequence of their goodwill could have been a deterioration in wellbeing. Social distancing measures, where significant others were required to avoid physical contact with older adults may have negatively affected older adults’ wellbeing. The study findings imply that this significantly affected the older adults’ health negatively thus contributing to deterioration in their overall wellbeing. Hence, these findings imply a critical review on how to strike a balance between health and other needs of older persons including psychosocial and financial, with the goal of enhancing their overall wellbeing.
In addition to the extent of community adherence to COVID-19 measures, socio-demographic factors (age, marital status and income) were found to be significantly related to the deterioration in wellbeing. The findings show less deterioration in wellbeing among married, older persons with relatively higher incomes compared to other categories. Hence, there is need for targeted interventions particularly focusing on the younger adults who were single (widowed, divorced, separated, and never married) with low income since their wellbeing was at a higher risk of increased deterioration during the COVID-19 pandemic. However, as previous studies had established, wellbeing is a multi-dimensional and complex issue and safeguarding against its deterioration during the pandemic requires a critical review of its influencing factors.
Analysis on individual domains of wellbeing found that COVID-19 affected the various domains of wellbeing differently. However, income and age featured prominently as common factors that positively predicted wellbeing in most domains. As a coping strategy to deal with challenges, older adults seemed to have sought divine intervention as shown by the increasing spiritual wellbeing among those with low income and no spouses for support. However, more research is needed for an in-depth analysis of community adherence to COVID-19 measures on each domain of wellbeing
Limitations of the Study
One of the major limitations of this study was the use of snowball sampling in sample selection. Hence, the findings may not be appropriately generalized as elements in the target population were not given an equal chance of being selected into the sample.
Another limitation was that the study was a cross-sectional survey, making it challenging to determine the level of wellbeing of older adults prior to COVID-19. Hence, the study measured subjective change in wellbeing.
Although control variables were included in the regression, it is possible that other variables beyond the scope of this study may have impacted the results. Further investigation is therefore required to examine any other micro and macro impacts of adherence.
Since the interview schedule was in the English language and some respondents could not communicate well in the language, translation to the local Kikuyu language and/or Kiswahili was done for effective communication. Hence, although training on translation had been done, there may have been words whose meaning was slightly altered during translation.
Supplemental Material
Supplemental Material - The Relationship Between Community Adherence to COVID-19 Containment Measures and the Wellbeing of Older Adults in Rural Kenya
Supplemental Material for The Relationship Between Community Adherence to COVID-19 Containment Measures and the Wellbeing of Older Adults in Rural Kenya by Pauline Thuku in Gerontology and Geriatric Medicine
Footnotes
Acknowledgments
The author gratefully acknowledges the contribution of Mr Timothy Mwago for his assistance in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The author declares that ethical considerations of confidentiality, anonymity and informed consent were adhered when conducting the study. Permission to conduct research was granted, and informed consent verbally sought from each respondent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.