
Abstract
We aimed to clarify the association between social activity and the development of dementia in older adults by hearing-impaired (HI) status. We applied a community-based prospective cohort study over 6 years as part of the Japan Gerontological Evaluation Study. The study included 53,549 participants aged 65 years and older who did not require long-term care. A baseline questionnaire survey was conducted; explanatory variables included physical and social activities, and the objective variable was dementia onset assessed by standardized protocol. Cox regression models were used to calculate hazard ratios (HRs) for dementia stratified by HI status. During the follow-up period, 6013 (11.2%) participants developed dementia. Analyses revealed increased dementia risk for participants with HI who participated in the following activities less than once a month: sport groups (HR 2.17, 95% CI 1.53-3.08), hobby groups (HR 1.70, 95% CI 1.34-2.17), going out (HR 2.19, 95% CI 1.51-3.17), and meeting with friends (HR 1.27, 95% CI 1.06-1.53). HI and lack of social activity increase the risk of dementia. The study results indicate that there is an association between low social activity and the development of dementia in people with HI; the strongest associations were found for low participation in sports and hobby groups.
Introduction
Hearing impairment (HI) is one of the risk factors for dementia (Livingston et al., 2017). HI, even when mild, increases the long-term risk of developing dementia (Daniele et al., 2018). Among the preventable risk factors for dementia, HI has been identified as the most important modifiable risk factor (Livingston et al., 2017).
In addition to dementia, HI can lead to depression (Li et al., 2014), apathy (Sugawara et al., 2011), and limited participation in daily activities due to reduced stimulus input, negative impact on family relationships and social interactions (Servidoni & Conterno, 2018), social isolation due to impaired communication (Strawbridge et al., 2000), and adverse effects on the degree of social interactions (Ogawa et al., 2019). The possibility of a causal relationship between the inhibition of social interaction, depletion of cognitive reserve, social isolation, environmental changes, and a combination of these factors with dementia has also been reported (Ives et al., 1995).
Recently, the importance of social participation in the cognitive functioning of older adults has been widely highlighted. Social participation has been defined by various other researchers (Putnam, 1995; Berkman, 1995). Previous studies have shown that social activity among older adults is associated with reduced risk for long-term care and death (Kanamori et al., 2014; Murata et al., 2017; Saito et al., 2019; Aida et al., 2011; Kawachi et al., 1996).
Older adults with high social participation have higher cognitive function than those with low social participation (Barnes et al., 2004; Holtzman et al., 2004), and social participation suppresses the decline of cognitive function (Uchino, 2006). The strength of social networks, such as social activities and socializing with friends and family, is associated with cognitive functioning and prevents dementia (Holtzman et al., 2004). Decreased social participation increases the risk of developing dementia (Saczynski et al., 2006), and people with fewer social networks have a higher risk of cognitive impairment (Nemoto et al., 2017). Moreover, living alone and having no personal connections doubles the risk of developing dementia in 3 years (Fratiglioni et al., 2000). However, to our knowledge, no study has revealed the relationship between the type of social participation and dementia among older people with HI. In this study, we used large-scale longitudinal data over 6 years to clarify the association between activities performed by older adults with HI and the risk of developing dementia in Japan.
Methods
Study Design and Participants
The study design was a community based prospective cohort study from the Japan Gerontological Evaluation Study (JAGES). The baseline survey was conducted from August 2010 to January 2012 by distributing questionnaires to 95,827 randomly-selected older adults who had not been certified as requiring support or long-term care and resided in 13 municipalities in seven prefectures in Japan.
We excluded 7889 people who had missing sex or age information on the self-administered questionnaire, whose answers were inconsistent with the list received from the municipalities, who returned the personal identification code detached from the questionnaire, and who did not give consent for the use of their data for research. Therefore, valid data at baseline was 54,537. We further excluded 153 people with reduced activities of daily living (ADL) who reported difficulty in caring for themselves. We followed up with these people using the “data on the certification of the need for long-term care” that included the onset of dementia and the “data on the levy of long-term care insurance” that included mortality for 6 years to determine the presence of dementia or the need for long-term care.
To reduce the effect of the reversal of causality, we excluded 835 individuals whose follow-up period was less than 365 days. Deaths within 365 days were also excluded. Finally, 53,549 participants (24,534 men and 29,015 women) were included in the analysis. The follow-up status of the participants is shown in Figure 1. Flow of participants for analytic sample.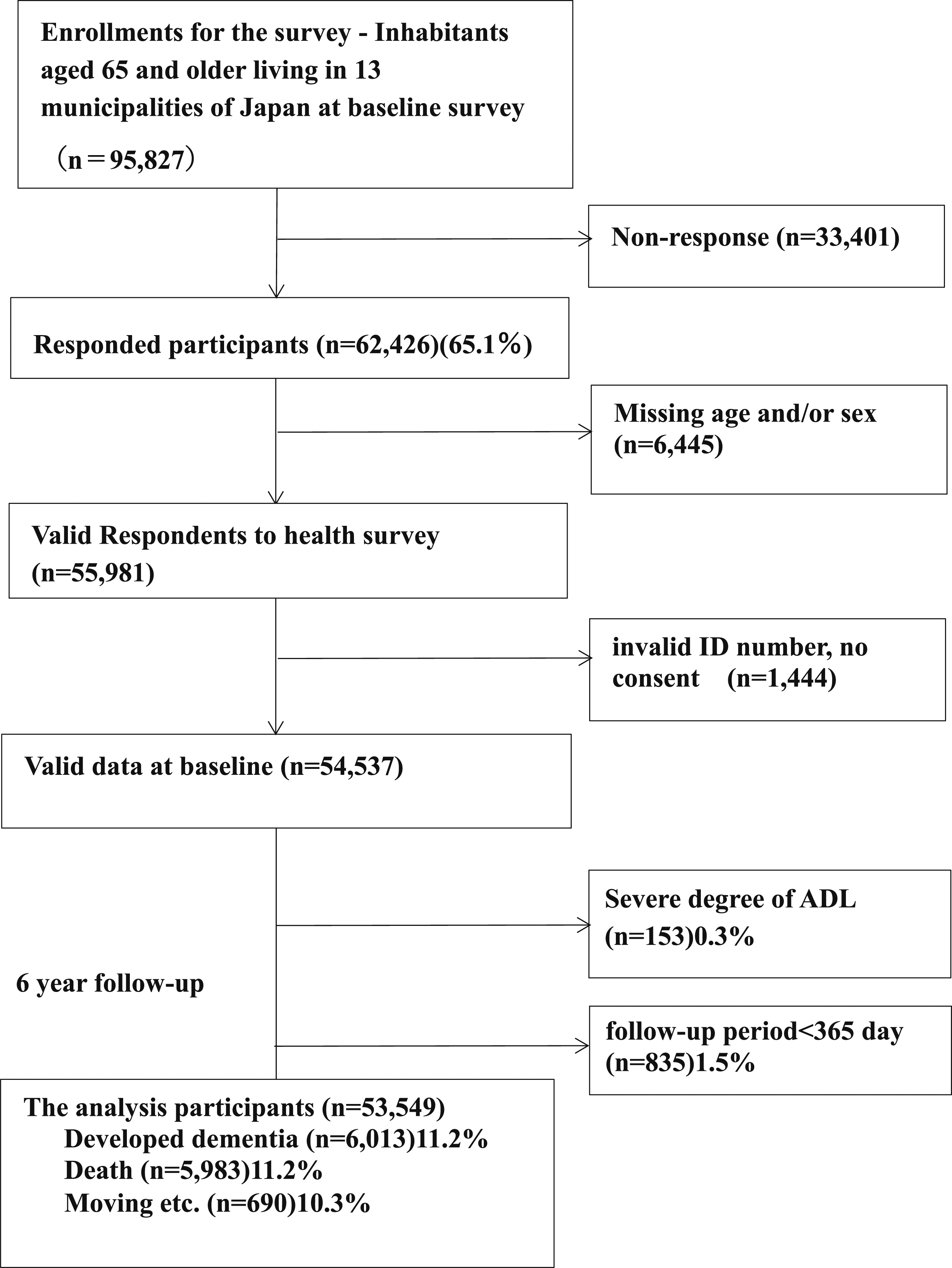
Variables
Outcome Variable
HI was defined as those who selected self-reported HI as a disease under treatment during the baseline survey.
The outcome variable of the development of dementia was determined if a participant was certified as requiring support or care and classified as IIa (Hisano, 2009; Noda et al., 2018) or higher for “level of independence in daily living for the elderly with dementia” defined by the Ministry of Health, Labor and Welfare. The IIa level is assigned when symptoms, behaviors, or difficulties in communication, related to dementia, that interfere with daily life are observed; the person can be independent if someone pays attention to them. Symptoms of dementia include frequently getting lost, noticeable errors in shopping, office work, money management, and other things that were previously possible. This dementia index is strongly correlated with the Mini-Mental State Examination (r = −0.74) (Hisano, 2009). The dementia scale was an effective indicator for the clinical diagnosis; reported sensitivity and specificity were 73% and 96% for rank II dementia, respectively (Noda et al., 2018).
Explanatory and Covariates Variables
Explanatory variables about social activities included the frequency of activities and the presence of leisure activities. The frequency of going out (twice a week or more, once a week to once a month or more, once a month or less), frequency of meeting friends, and participation in hobby and sport groups (once a month or more) were surveyed (Willie-Tyndale et al., 2016). Covariates to be adjusted included age, sex, self-rated health, ADL, depressive symptoms assessed by geriatric depression screening scale-15 (GDS) (Brink et al., 1982), smoking status, education, equivalent income, marital status, and living arrangement. Age was categorized into five groups: 65–69, 70–74, 75–79, 80–84, and 85 years and older. Self-rated health was categorized into good (very good, fair) and poor (not so good, poor). ADL responses were requested in the following categories: no assistance, partial assistance, and full assistance. Level of depressive symptoms was categorized using the GDS: 0–4 points as no depression, 5–9 points as mild depression, and 10–15 points as depression. Smoking status was categorized into non-smoking (never smoked, quit more than 5 years ago, and do not smoke now) and smoking (quit less than 5 years and do not smoke now, still smoking). Equivalent income was categorized into less than 2 million yen, 2–4 million yen, and 4 million yen or over). Equivalent income was calculated by dividing the total annual income of the entire household by the square root of the number of household members. Education was categorized by years of education: less than 10 years, 10 years or more.
Statistical Analyses
We described the distribution of each variable used in the analysis; the proportion of people who developed dementia by each attribute is expressed in the HI group and normal hearing group, and the chi-square test was used to compare the percentages by each attribute.
To examine the association between social activities and the development of dementia, hazard ratios (HRs) and 95% confidence intervals (95% CIs) were calculated using the Cox proportional hazards model after stratification into two groups: HI and normal hearing. The group with higher participation in each social activity was set as the reference in all the analyses. Samples with missing values in the covariates were included in the analysis by setting the missing categories, i.e. missing-indicator method.
Factors that were significant at the p < 0.10 level in univariate regression were used. In addition, we used factors whose explanatory variables have been suggested to be associated with hearing impairment and dementia in previous studies (Emmett & Francis, 2015; Kochkin, 2007; Yamada et al., 2011; Wayne & Johnsrude, 2015; Uchida et al., 2019; Panza et al., 2015; Amieva et al., 2018). Covariates of age and sex were included in Model 1, self-rated health, ADL, current smoking, and depressive symptoms, living arrangement, equivalent income, education, and marital status were included in Model 2. We performed analyses using IBM SPSS Statistics version 24. The statistical significance level was set at p < 5%.
Ethical considerations
The JAGES protocol was reviewed and approved by the Ethics Committee on Research of Human Subjects at Nihon Fukushi University (approval No. 1005) and the Ethics Committee of the Chiba University Faculty of Medicine (approval No. 2493).
Results
Characteristics of the Surveyed Participants.

The total number of participants is shown as a percentage. Comparisons were made using the chi-square test.
For missing values, missing categories were created and included in the analysis.
Hazard Ratios (HR) to Develop Dementia by Social Activities.

Model1:adjusting for age, sex.
Model2 further adjusting for self-rated health, activity of daily living, current smoking, and depressive symptoms as physical factorsliving arrangement, equivalent income, education, and marital status as social factors.
HR: hazard ratio, CI: confidence interval.
Discussion
In this cohort study, we revealed an association between social activities and the development of dementia in people with HI. This is the first study to show the association in older people with HI to the best of our knowledge. After adjusting for factors such as age, sex, physical factors, mental factors, educational background, and living conditions, there was an association between social interaction and social activities with the development of dementia in people with HI. Stronger associations were found for participation in sport and hobby groups, which involve deeper interaction and communication.
The crude incidence of dementia was more than twice as high. After adjusting for gender and age, the incidence was 1.28 times higher than in healthy subjects. The results were the same as in the previous study (Michalowsky et al., 2019). Preventing cognitive decline is very important for older people with HI.
Hazard ratio of people with HI were higher for those who participated in sports (HR2.17 vs. 1.28) and hobby (HR1.70 vs. 1.34) groups less than once a month compared with people with normal hearing. For other social activities, the difference between people with normal hearing and HI people was minimal. Leisure activities had a lower HR than hobby and sports groups. This is because leisure activities include pachinko, gardening, painting, and other activities that do not require communication and can be enjoyed individually. Dementia was not associated with participation in social activities once a month. Instrumental Activities of Daily Living (IADL) limitations were reported to be associated with a long-term risk of developing dementia (Bennett et al., 2006). A decline in ADL may be associated with dementia in older adults with HI. For the HI in Table 1, there was no association with living arrangement. Even if HI people live alone, having social activity opportunities and interaction may prevent dementia. Participation in socially interactive activities with others and physical activities is important in reducing the risk of dementia.
Hazard ratio of meeting with friends less than once a month was high in this study. HI, cognitive function, isolation, and depression are interrelated (Dawes et al., 2015). Therefore, social activities may prevent isolation and depression and prevent cognitive impairment for people with HI. Previous studies have reported that social networks prevent dementia in general older people (Levasseur et al., 2010), which is consistent with reports from longitudinal studies, which found that lack of social connections was associated with an increased risk of dementia (Uchino, 2006). Social networks may facilitate access to healthy behaviors for HI people, which in turn may help prevent dementia. In a study that analyzed the relationship between social relationships between HI people and older adults, the researchers found that HI people tended to have smaller networks, and HI was one of the factors associated with social relationships in older adults (Pérès et al., 2008). It is important for HI people to widen their social networks
Social activities in congenital HI and profound acquired HI are different. There are many reports on social activities in HI people with congenital HI (Moog et al., 2011; Bat-Chava et al., 2005). The use of cochlear implants at an early age has been reported to improve students’ participation in club activities, sports meetings, communication, and social skills. Many people with congenital HI who do not use cochlear implants have learned sign language and use it to communicate with others. They are often socially active within the community of congenital HI. On the other hand, it is difficult for people with profound acquired HI to learn sign language and join the community of HI. Limited communication at home and with friends has been associated with social introversion and loneliness (Knutson & Lansing, 1990). HI has many negative effects on daily life, including depression (Li et al., 2014) and apathy (Sugawara et al., 2011). Social networks have been associated with factors that affect brain function, such as stress and depression (Dori et al., 1994), and neuroendocrine measures of stress have been associated with dementia (Brice & Strauss, 2016).
Thus, social activities may be an effective way to maintain communication opportunities while covering the HI of older adults in the community. People should start social activities such as sport or hobby clubs early, from the time their hearing function was normal and should continue them even if hearing function declines. A longstanding relationship will be useful for mutual understanding in the club. Moreover, the use of hearing aids and consultations with audiologists will be effective for the HI to more deeply interact and communicate with others. Financial assistance for hearing aids and the development of better hearing aids should be promoted. It is also important to advise people on how to access these services.
Our findings suggest that providing opportunities for social activities and interaction for the hearing-impaired older adult is a viable intervention to promote social participation among the elderly in Japan and may be effective in preventing the onset of dementia. Future research should investigate the types and details of social activities and interactions, such as sports and hobbies. This could contribute to the prevention of dementia in the hearing impaired.
Strengths
The strengths of this study include its cohort design, which provides more convincing evidence than a cross-sectional design. Another strength is the large sample size of more than 50 thousand total participants analyzed, and more than four thousand participants with HI. According to the large scale study, we revealed the relationship between social activities and the development of dementia in hearing-impaired older people.
Limitations
This study had several limitations. First, self-administered questionnaires were used as the data collection tool, which may have led to information bias. The HI was assessed based on a questionnaire survey that uses responses to whether HI is being treated. We were unable to exactly ascertain the severity of the HI in the participants, but we saw the HI level of participants as that which required treatment. There is a difference between the subjective assessment of hearing test results (Kamil et al., 2015) and the underestimation of HI (Uchida et al., 2003) in older adults. Second, information on the use of hearing aids and other devices that assist hearing function is missing. Among those receiving treatment for HI, it was not possible to discern who used hearing aids and other devices and who did not. Further research is needed to confirm these findings. Finally, this study did not consider factors in the community or the environment. Community-based intervention studies have shown that social capital effectively prevents the onset of disabilities and cognitive impairment (Hikichi et al., 2016; Hikichi et al., 2015). Community-level social capital has been associated with individual-level health outcomes (Tsuji et al., 2018; Tsuji et al., 2019; Fujihara et al., 2019). Urban areas, railroad tracks, airports, and highways are noisy, and the possibility of noise-induced HI cannot be ruled out (Chen et al., 2017). Environmental factors may also affect social activities, such as differences between urban and rural areas. In the future, it will be necessary to examine the differences between regions to determine how to address these issues at the community level.
In conclusion, this cohort study suggests that social interaction and social activities are related to cognitive function in people with HI. Maintaining opportunities for social communication and activities may help prevent dementia.
Footnotes
Acknowledgments
This study used data from the JAGES. We are extremely grateful to all the study participants for their personal data. We would like to express our deepest gratitude to everyone who participated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study used data from the Japan Gerontological Evaluation Study (JAGES), which was supported by JSPS(Japan Society for the Promotion of Science) KAKENHI Grant Number (15H01972, 18H03047, 19H03860, 20H00557, 21K02001,21K19635), Health Labour Sciences Research Grant (H28-Choju-Ippan-002), Japan Agency for Medical Research and Development (AMED) (17dk0110017, 18dk0110027, 18ls0110002, 18le0110009,21dk0310108h0002, 22dk0310108h0003), the Research Funding for Longevity Sciences from National Center for Geriatrics and Gerontology (29-42,21-20). Open Innovation Platform with Enterprises, Research Institute and Academia(OPERA, JPMJOP1831)from the Japan Science and Technology (JST).
Authorship
Kaori Kojima (1) Substantial contributions to the conception or design of the work, or acquisition, analysis or interpretation of data for the work; (2) Drafting the work or revising it critically for important intellectual content; (3) Final approval of the version to be published; (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Meeting these criteria should provide each author with sufficient knowledge of and participation in the work that he or she can accept public responsibility for the report. Eisaku Okada (1) Substantial contributions to the conception or design of the work, or acquisition, analysis or interpretation of data for the work; (3) Final approval of the version to be published; (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Meeting these criteria should provide each author with sufficient knowledge of and participation in the work that he or she can accept public responsibility for the report. Toshiyuki Ojima (1) Substantial contributions to the conception or design of the work, or acquisition, analysis or interpretation of data for the work; (3) Final approval of the version to be published; (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Meeting these criteria should provide each author with sufficient knowledge of and participation in the work that he or she can accept public responsibility for the report. Jun Aida (2) Drafting the work or revising it critically for important intellectual content; (3) Final approval of the version to be published. Yoshimune Hiratsuka (2) Drafting the work or revising it critically for important intellectual content; (3) Final approval of the version to be published. Katsunori Kondo (2) Drafting the work or revising it critically for important intellectual content; (3) Final approval of the version to be published.