
Abstract
The objective was to analyze predictive variables for falls in older community-dwelling adults who needed walking aids or home help service, to describe the circumstances and consequences of falls and fall injuries, and to describe the activities preceding falls, n = 175, mean age 83 years. Falls were self-reported monthly in a fall calendar and were followed up by a telephone interview. A logistic regression analysis was performed to investigate predictive baseline variables for falls. Injuries were reported in 82 of the 185 fall events. Previous falls and a high level of education had a significant association with falls odds ratios 1.9 (95% CI 1.3–2.7), and 2.7 (95% CI 1.4–5.3). Activities preceding the falls were classified according to the International Classification of Functioning (ICF). Falls and fall injuries were most common while moving around within the home and rising from sitting to standing.
Keywords
Introduction
Accidental falling in the older population is a threat to health, autonomy, and well-being (Rubenstein, 2006) and falls are the main cause of unintentional injuries among older adults (Peel, 2011; Stevens et al., 2008). The consequences of falls are often more devastating for older adults than for younger people because of a higher susceptibility to injuries due to, for example, osteoporosis and slowed protective balance reactions (Rubenstein, 2006). Most falls cause no severe injuries, but in general, approximately 10% of falls result in serious injuries, such as head injuries and fractures (Peel, 2011). The most common injuries are of a minor type (swollen joints, bruises, abrasions) (Milat et al., 2011; Nachreiner et al., 2007). The reasons why older people fall are complex and are the result of numerous, interacting risk factors unique to the individual in interaction with the environment (Tinetti & Kumar, 2010). Well established risk factors for falls are previous falls, female gender, and old age (Ambrose et al., 2013). In a cohort of community-dwelling individuals aged 75 years or older, use of a walking aid or receipt of municipal home support was associated with falls (Hellström et al., 2013). Frailty as a fall risk factor has been confirmed (Cheng & Chang, 2017) but factors associated with the sub group of pre-frail community-dwelling older people who need walking aids or home help service have been sparsely studied.
The circumstances and consequences of falls in community-dwelling older adults (aged 75 years or older) with some degree of frailty have been studied (Hill et al., 2013; Nachreiner et al., 2007). Nevertheless, fall circumstances, including activities executed immediately before the fall event irrespective of injury, as well as the consequences of falls in community-dwelling adults ≥75 years of age who need walking aids or home help service, have been only sparsely investigated. Behavioral strategies for fall prevention originating from the specific circumstances surrounding the fall event can be used as a basis to reduce falls (Nachreiner et al., 2007). Increased knowledge regarding which activities are linked to the fall injuries that most often occur in older adults with walking aids or home support could be a valuable contribution to the prevention of fall injuries in the older population.
One framework for the standardisation of activities is the World Health Organization International Classification of Functioning, Disability and Health (ICF) (World Health Organization, 2001) which so far has been used to a limited extent in descriptions of falls (Pohl et al., 2015; Saverino et al., 2015). The ICF is a holistic classification system for the description of health reflecting aspects of bodily function and structures, activities and participation, the environment, and personal factors (World Health Organization, 2001). It offers a structure and a common language for describing activities, and it enables better understanding across different professions. The ICF framework has previously been used to relate concepts of fear of falling to components of the ICF model in community-dwelling older men and women (Pohl et al., 2015). To our knowledge, in only one previous study, has the ICF classification been applied to describe the activity at the moment of a fall (Saverino et al., 2015).
A randomized controlled fall prevention trial (n = 175) was conducted in a sample of community-dwelling older adults who received walking aids, security alarms and/or home help service, from the year 2012–2016. The within and between-groups results as well as fall rate and injury rate have been presented previously (Tuvemo Johnson et al., 2021). The present study was based on the same sample, but the aim of this study was to analyze predictive factors for falls. The study objective was also to describe the circumstances and consequences of the occurred falls in the study sample (baseline to 12 months).
Methods
Design
This study had a longitudinal, descriptive design.
Participants
Data for the current study were collected as part of a randomised, controlled trial (RCT) (trial nr XX) conducted in Sweden from 2012 to 2016. The results from the main RCT follow-up have been presented elsewhere (Tuvemo Johnson et al., 2021). Community-dwelling older adults were recruited for the study by physiotherapists or occupational therapists when walking aids were prescribed or by care managers when the older adults applied for home help service or security alarms, which indicated some degree of frailty in the sample. The inclusion criteria for the RCT were individuals 75 years or older, living in their own homes, with the ability to walk independently indoors, and with the ability to understand written and oral information in Swedish. Individuals with scores less than 25 on the Mini Mental State Examination (MMSE) (Folstein et al., 1975), those receiving ongoing physical therapy treatment due to illness or injury, and those receiving terminal care were excluded. Altogether, 335 individuals were assessed for eligibility, and 175 were finally included (122 women and 53 men, M 83.2 ±4.6 years) (Figure 1) after oral and written consent. Of the 175 older adults (122 women, 53 men), 74 individuals (42.3%), 50 women (41%) and 24 men (45%), fell during the first year (±30 days) after inclusion in the RCT (fall rate 1.06/person). Of the participants, 86.9% had a walking speed of <0.8 m/s or ≤ 10 points in the Short physical Performance Battery (SPPB) measure (Abellan van Kan et al., 2009; Apóstolo et al., 2017). The 175 participants’ characteristics are shown in Table 1. Selection and study process. Baseline characteristics and baseline test outcomes of the 175 study participants; Individuals who encountered no falls, n = 101 and one or more falls, n = 74 from baseline to 12 months. Numbers, (%), Outcomes, mean ±SD/median [IQR]. Abbreviations: FES (S) = Falls Efficacy Scale, Swedish version; EQ-5D VAS = EuroQuol 5 Dimensions Visual Analogue Scale.

Procedures
The RCT was three-armed with two intervention groups and one control group. One intervention group received the Otago exercise program (OEP), which is a home-based individualised exercise program that includes balance training, strength training and outdoor walks (Gardner et al., 2001) and the other intervention group received OEP and motivational interviewing (MI), which is a method used to start and support behavioral changes (Rollnick et al., 2008). The participants in the RCT were followed for 12 months with fall calendars to identify falls and with telephone interviews to collect data about the circumstances and consequences of the falls. The study was approved by the Regional Ethics Review Board of Anonymised, Sweden (Nr XX). The participants received no compensation for their participation.
Measurements
The baseline questionnaire included background data and self-reported fall frequencies for the previous 12 months. The participants were asked to rate their level of physical activity, home help utilisation, and level of education. Questions about the use of walking aids, fall events the previous year, and housing and living arrangements were also included, as well as the Falls self-efficacy (FES (S)) (Hellstrom & Lindmark, 1999) and EuroQol 5 Dimensions (EQ-5D) (Rabin & de Charro, 2001). The Short Physical Performance Battery (SPPB) (Guralnik et al., 1994), the mini-BESTest (Franchignoni et al., 2010), the Geriatric Depression Scale (GDS) (Gottfries et al., 1997), the Mini Nutritional Assessment (MNA) (Guigoz, 2006), as well as the above mentioned measurements were completed in the participants’ homes or at a health care center by experienced physiotherapists who were not involved in the interventions. All of the tests and measurement scales used at baseline have been reported to have sound psychometric measures (Franchignoni et al., 2010; Freire et al., 2012; Gottfries et al., 1997; Guigoz, 2006; Hellstrom & Lindmark, 1999; Rabin & de Charro, 2001).
A fall was defined as “an event in which a person unintentionally comes to rest on the floor or ground, regardless of the cause and the consequences of the fall” (Jensen et al., 2002). Fall frequencies were collected via daily reports from the older people in calendars for falls (Lamb et al., 2005) over the 12 months from baseline. The fall calendars and return envelopes were provided to the participants in conjunction with the base line measurements and were mailed monthly to the researchers. If a calendar was not returned on time, the participant was contacted by telephone by a research-team member. Reported falls were followed up monthly by research-team members via structured telephone interviews with questions about the circumstances surrounding the fall (when, where, perceived cause, and activity immediately before the fall), and the consequences of the fall (injured or not, injury location, type of injury and treatment). The answers received were written down in forms.
Data analyses
Categorical data are presented with frequencies and percentages, n (%). Ordinal variables are presented with medians (Md) and inter quartile ranges (IQR) and continuous variables with means (M) ± standard deviations (SD). According to the type of data, Pearson’s chi-square test and the independent t test were used to examine differences in gender and age between fallers and non-fallers. To analyze differences in the distribution of falls resulting in injurious falls or non-injurious falls in the ICF-classified activities, Pearson’s chi-square test was used. Statistical significance was set at p < 0.05, and statistical analyses were performed using IBM SPSS statistics software, Version 24 (SPSS Inc, Chicago, IL, USA).
Variables entered on step 1 in the logistic regression model.

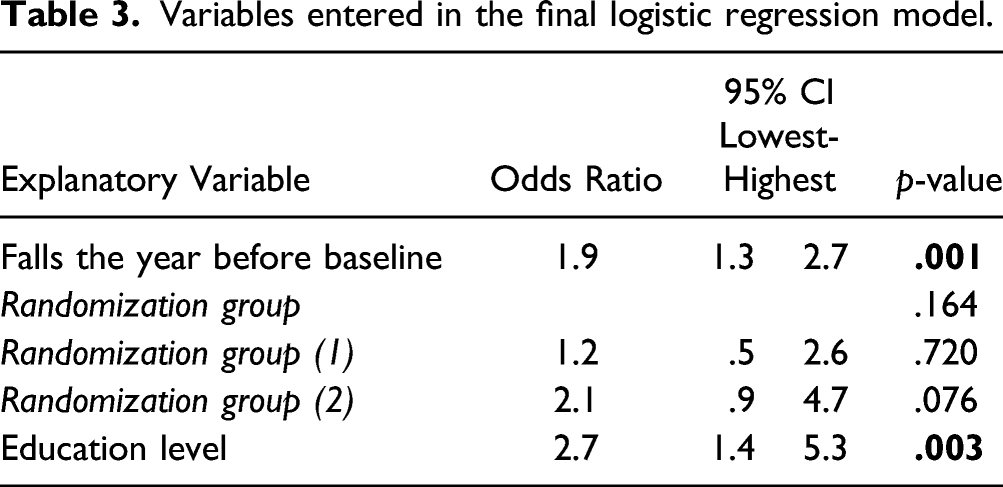
Variables entered in the final logistic regression model.
Circumstances of 185 fall events in 74 study participants. Places of the falls and perceived causes of the falls.
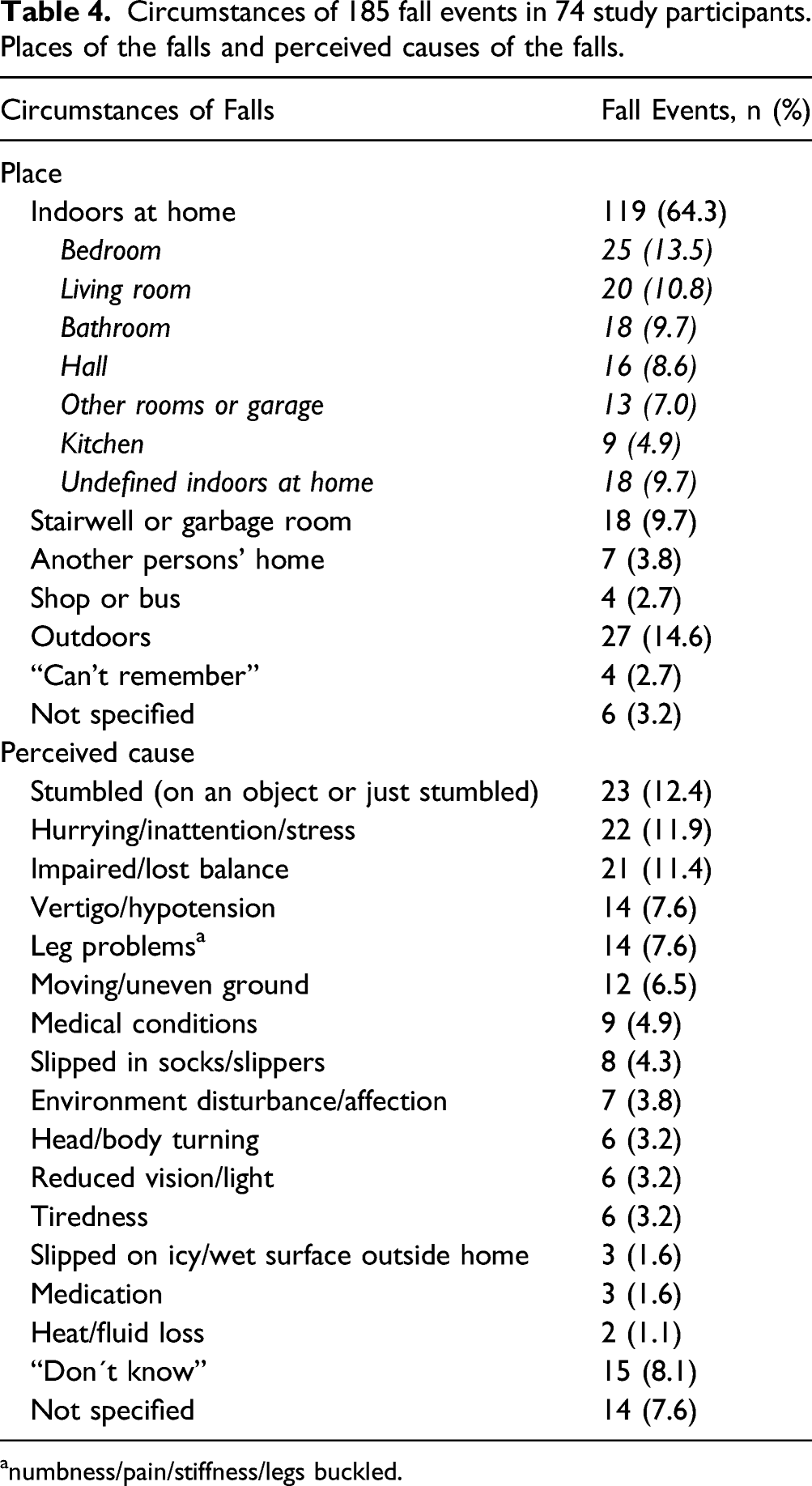
anumbness/pain/stiffness/legs buckled.
ICF classified activities in 185 fall events in 74 study participants and the events involving injuries and no injuries, respectively. Frequencies and percentages of all fall events.

Difference in the ICF classified activity distribution between injurious and non-injurious falls, p value = 0.403.
Consequences of 185 fall events in 74 study participants.

The structured classification of the ICF (World Health Organization, 2001) was used to classify activities in fall situations. The ICF consists of 1454 categories (World Health Organization, 2001). Each category is assigned a unique code containing a letter representing each of the components’ body functions (b), body structures (s), activity and participation (d), and environmental factors (e). The letter in the code is followed by digits representing the first, the second, or the third level in the classification. The following example shows the structure of the ICF: “d – Activities and participation” (component)
“d4 – Mobility (first level)
“d460 Moving around in different locations” (second level) “d4600 Moving around within the home” (third level).
The written answer to a telephone-delivered question about “activity immediately before the fall” was coded according to the third level of the ICF by the first author. If two or more codes were applicable for the same fall event, the most physically demanding activity was coded. In one complex case, the first and last author discussed the coding until consensus was achieved. If sufficient data for coding were not provided, the activity was classified as “not specified”.
Results
Prediction of falls
Factors independently associated with falls were level of education and one or more falls the year before baseline. A high level of education was the most predictive factor for a period of 12 months with an odds ratio = 2.7 (95% CI 1.4–5.3), Table 3. In addition, previous falls was also significantly predictive: odds ratio = 1.9 (95% CI 1.3–2.7), Table 3. The final model accounted for between 15.3% and 20.6% of the variance in falls.
Fall events
Over a period of 12 months in the RCT, 40 participants (22.8%) reported one fall, 18 (10.3%) reported two falls, and nine persons (5.1%) reported three to four falls. Eight (4.6%) of the participants experienced five or more falls, and one of them encountered 28 falls within the 12-month period. Neurological disorders were overrepresented (4/8) in the sub-group who fell five times or more in 12 months, and of the three participants who fell 10 times or more, all of them had Parkinson’s disease. Eight of the fallers were followed for less than 12 months due to death (n = 4), severe diseases or other personal reasons for leaving the study (n = 4). The within and between-groups results as well as fall rate and injury rate have been presented earlier (Anonymised for Review # 1).
Circumstances of falls
Approximately 75% of the falls occurred in the morning or in the daytime, and 17% of the falls took place in the evening (9.7%) or at night (7.5%). In 8% of the falls, the time point of the fall was not specified. Most of the falls in this group of older adults occurred indoors at home (64.3%) in the bedroom or in the living room. The perceived causes of the falls were often stumbling, hurrying/inattention/stress, perceived balance deficits or unknown (Table 4).
In the reported fall events, 27 different activities on the third level of the ICF were identified. These activities were linked to 12 categories, according to the ICF’s second level. The ICF categories on the second level are presented in bold font (Table 5). The most common activities connected with the falls were moving around within the home (d4600) and changing body position (d410), especially when rising from sitting to standing (d4104).
Consequences of falls
Of the 74 participants who had fallen, 53 participants (71.6% of fallers) were injured due to a fall at least once in 12 months. Injuries were reported in 83 (44.9%) of the 185 accidental fall events, of which seven falls (3.8% of falls) resulted in fractures. Based on the 175 participants in the RCT, injury rate over the 12-month period was 0.47/person. Injury treatment was stated in 30 (16.2%) of the falls, of which outpatient care was required after 16 falls (8.6%), and seven falls required a hospital stay (3.8%). The most reported injuries were bruises, contusions and abrasions, and the lower limbs were most often injured (Table 6).
Discussion
The literature frequently demonstrates previous falls as a risk factor for falls which, once again, was confirmed in this sample of relatively frail older adults. A consistent association between falls and socioeconomic factors such as educational level is not yet confirmed in the literature (Alamgir et al., 2015; Bloch et al., 2010) but some studies have identified high education as a protective factor for falls (Busch Tde et al., 2015; Nascimento et al., 2018). However, in our study, a significant association between high education level and falls was found. High education as a fall-risk factor in older people in Sweden, has to our knowledge, not been identified earlier but has been seen in India where a sedentary life style was the main cause reported (Pitchai et al., 2019). A higher education level is well known to be associated with increased occupational sitting time (De Cocker et al., 2014; Piirtola et al., 2020; Wallmann-Sperlich et al., 2014) which during a whole working life might, but not necessarily may, influence muscle strength and balance reactions. We suggest further studies on the influence of the life-span activity level on falls.
The 185 falls which occurred within 1 year from baseline in the main study were examined. There was no significant difference in distribution between injurious and non-injurious falls in the ICF-classified activities performed at the time of the falls. Moving around within the home (d4600) and rising from sitting to standing (d4104) represented the activities when most of the injurious (and non-injurious) falls occurred, indicating that special attention on these activities might be of importance in fall prevention for older community-dwelling people who need walking aids or home support. According to the ICF classification, moving around within the home includes “walking or moving around in one’s home, within a room, between rooms, and around the whole residence or living area” (World Health Organization, 2001). Previous research has identified “while walking” as one common activity related to falls (Berg et al., 1997; Boye et al., 2014; Duckham et al., 2013; Nachreiner et al., 2007; Talbot et al., 2005). The concept of “walking” has been defined in some studies as indoor or outdoor walking (Boye et al., 2014; Duckham et al., 2013) but in other studies walking has been unclearly defined (Berg et al., 1997; Nachreiner et al., 2007) or has been described as “ambulation” (Talbot et al., 2005). In the ICF classification, the broad concept of “walking” is separated into several categories. For instance, the ICF classification’s third level displays differences among walking shorter distances (d4500), walking longer distances (d4501), walking on different surfaces (d 4502), and moving around within the home (d4600). The ICF classification can provide more detailed descriptions of the activities, which could be valuable when comparing circumstances at the time of fall events in future studies and in clinical settings.
This current study, as well as other studies on fall circumstances in similar, but not identical, cohorts of older adults (Boye et al., 2014; Hill et al., 2013; Nachreiner et al., 2007), showed that most of the falls occurred in or around the home. Based on these findings, we recommend placing priority on indoor fall prevention when the targeted group is similar to the sample in our study. Others have also suggested that fall-preventive actions should be tailored to indoor respectively outdoor fallers (Boye et al., 2014; Kelsey et al., 2010, 2012).
In this current study, the participants’ participation in a fall prevention study might have influenced the number of fallers and the total number of falls. However, the number of fallers over a period of 12 months (74/175 = 42.3%) was close to (Rubenstein, 2006) or even higher than those reported in similar age groups (Milat et al., 2011), which might be explained by the high occurrence of balance problems in our study population, in which 92% of the participants used walking aids at base line. In this study, 58% had suffered one or more falls during the year prior to baseline, indicating that these individuals were at increased risk for future falls (Chu et al., 2005; Deandrea et al., 2010).
The limitations of this study refer to the possibility of generalisation of the results. Since all the participants had chosen to participate in a fall prevention study, they were probably not representative of all community-dwelling older adults at risk for falling, and the results should consequently be generalised with cautiousness. In addition, two thirds of the RCT participants were expected to regularly accomplish home exercises, which might have had an impact on falling. However, no between group differences in falls were seen in the main study (Tuvemo Johnson et al., 2021). As inclusion criteria we used “pre-frail community-dwelling older adults who needed walking aids or home help service”. A formal frailty measure could have refined the included target population. However, 86.9% of the participants had a baseline walking speed of <0.8 m/s or ≤ 10 points in the SPPB. A gait speed of <0.8 m/s has been identified as a predictor of adverse outcomes and future disability in activities of daily living in community-dwelling older people (Abellan van Kan et al., 2009; Apóstolo et al., 2017), and ≤ 10 points in SPPB indicate an increased risk of mobility disability (Vasunilashorn et al., 2009), and all-cause mortality (Pavasini et al., 2016). This shows that most, but not all, of the included participants matched the target population. More thorough instructions given to the telephone interviewers about what to report if the respondent did not have an answer to the question could have reduced the amount of incomplete data. The coding of activities into the ICF format was performed by one author, except in one complex case. Two or more coders would have strengthened the trustworthiness of the results.
Our results indicated that a high education level is associated with falls. This association should be further studied in a life-span activity-level perspective. Our results also indicated, that in fall prevention for older community-dwelling people, aged 75 years and older, who have balance problems or need home help service, special attention should be paid to fall prevention actions connected to the activities of moving around within the home and rising from sitting to standing. We suggest that the examination of the performance and movements in these activities should be executed in the person’s own home to detect specific possible difficulties and obstacles in the specific activity. Based on the findings of the examination, suitable individual interventions could be planned and performed. The ICF classification provides a useful structure and a common language for describing activities preceding accidental falls, which, if used, could be valuable when comparing circumstances at the time of fall events in future studies and clinical settings.
Footnotes
Acknowledgments
The authors acknowledge the physiotherapy teams in Uppsala, Västerås and Eskilstuna who contributed to the conducting of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Municipality of Uppsala, the Regional Research Council in Uppsala and Örebro and the Uppsala County Council.
Ethical Approval
The study was approved by the Regional Ethics Review Board of Uppsala, Sweden (Dnr 2012/147). The participants received no compensation for their participation.