
Abstract
Millions of Americans aged 65+ are socially isolated and millions more report feeling lonely. Social isolation and loneliness in older adults were compounded by stay-at-home orders and other COVID-19 prevention measures. Although many Americans experienced no difficulties transitioning to the use of electronic devices as their primary means of communication and connection, some older adults were not similarly able to espouse this shift. Our aim was to reduce the impact of social isolation on older adults, increase their comfort in expressing feelings of loneliness, and assist them in acquiring technology skills and accessing telehealth and community supports. Participants received wellness calls for conversation, resource access and technology-based support. Most participants reported decreased loneliness and increased connectedness after the calls; half reported increased ease in expressing their feelings. Programs that provide phone-based support for older adults may reduce loneliness and increase social connectedness.
Keywords
Introduction
According to a National Academy of Medicine (NAM) report, prior to the COVID-19 pandemic, 25% of adults aged 65+ were socially isolated, and 43% aged 60+ reported feeling lonely (National Academies of Sciences, Engineering, and Medicine [NASEM], 2020). Public health measures and shelter-in-place orders that were implemented in an effort to contain the COVID-19 virus further exacerbated social isolation in this population. Due to heightened vulnerability to and increased risk of severe illness and death, adoption of social distancing measures by older adults was imperative.
As many Americans adapted to social distancing guidelines and were able to stay virtually connected with friends and family through the use of digital video conferencing platforms, some adults over the age of 65 were unable to similarly adapt to these changes (Berridge et al., 2020; Rajasekaran, 2020; Shteinlukht, 2021). As in much of the country, North Carolina programs that provide food, medication, socialization, and resource referrals to the older adult population were designed for in-person service delivery and became effectually inoperative when lockdown measures began. Non-profit and county agency personnel across the state shifted programming where possible from on-site to remote delivery, and many began offering alternative services such as grocery and prescription delivery (North Carolina General Assembly, 2021) but consistent, statewide solutions and countermeasures for the social isolation that resulted from the mandatory restrictions did not exist.
The Social Bridging Project was formed as a response to concerns about the potential impact of social isolation on older adults as a result of the pandemic. The project’s aim was to provide older adults who were isolated or lonely with a source of social connection, technology support, and referrals to needed resources. Phase I of the evaluation assessed whether participants “felt better” after a call and included some additional tracking related to the number of conversations, call duration and length of project enrollment. Our hypotheses for Phase II of the evaluation were that project participants would report decreased feelings of loneliness, an improved sense of social connectedness and increased comfort expressing feelings of loneliness.
Methods
University of North Carolina Asheville (UNCA) and Mountain Area Health Education Center (MAHEC) partnered together for the Social Bridging Project (SBP). UNCA housed the project, provided in-kind staff and grant support, and served as a source for volunteers, while MAHEC provided in-kind staff support and served as a referral source. Some student volunteers attended other regional universities, including the UNC Gillings School of Global Public Health, the UNC School of Pharmacy and Mars Hill University. Project staff and student volunteers underwent five hours of training that included information about active listening, crisis intervention and several call scenarios related to technology, food access, medication management and medical/mental health emergencies. Callers were also required to complete mock phone conversations and were given information sheets about community resources. Once trained, the student volunteers called participants who had been referred to the project or had self-referred and who were at increased risk of social isolation, mental and emotional health challenges and reduced access to in-person medical care and community support. Students were matched based on their field of study and participant need and provided a social connection and resources to lower COVID-19 infection risk and to increase access to telehealth and community supports as appropriate. Students also met weekly with project staff for group “huddles” that served as debriefing sessions for issues that warranted peer and mentor discussion and for continuous program improvement.
The Phase I evaluation consisted of a survey (University of North Carolina Asheville’s institutional review board) to assess the breadth and impact of the project (Appendix A). Qualtrics was used to log the calls, and students completed the survey independently after each call. The instrument included eight closed-ended and two open-ended questions, some of which were not required.
IRB approval for Phase II of the evaluation was received in June 2021. Phase II consisted of an expanded confidential participant survey evaluation component that included three modified items from the NIH Emotional Support and Loneliness Fixed Form Scales and eight additional items developed by project staff (Appendix B). Response options for closed-ended questions were Yes, No, Not Sure and Not Applicable. The tool was administered over the phone via a Google form without personal identifiers. Wellness callers described the survey to all active participants (41) and obtained preliminary consent from 19 participants to receive a survey call. A dedicated evaluation caller who had had no previous contact with project participants contacted those who had given preliminary consent. Of those 19 participants, six requested to remain in the program but declined the survey. Verbal informed consent was obtained from the remaining 13 participants before conducting the survey.
Results
From August 11, 2020 to June 30, 2021, 905 calls were made to 77 older adults in a five-county catchment area, 59.2% of whom reported living alone. Although participant age was not required or reported for most calls, the age range of participants who volunteered their age was 50–95. Of the 905 calls, 446 (49%) resulted in a conversation, and 459 (51%) did not result in a conversation or were incomplete. Completed calls ranged in length from 1 to 170 minutes. Average call length was 31 minutes; median call length was 22 minutes. A little over half (57%) of the participants had four or fewer conversations, while the remaining 43% (33) had as many as 27 conversations. Of the 33 participants with more than four conversations, 42% (14) remained active for eight to ten months, and 16% (5) remained active for more than ten months. Some participants stayed in the program until they had acquired technology skills or other needs were met, while others remained for continued social contact.
Primary Topic of Conversation.

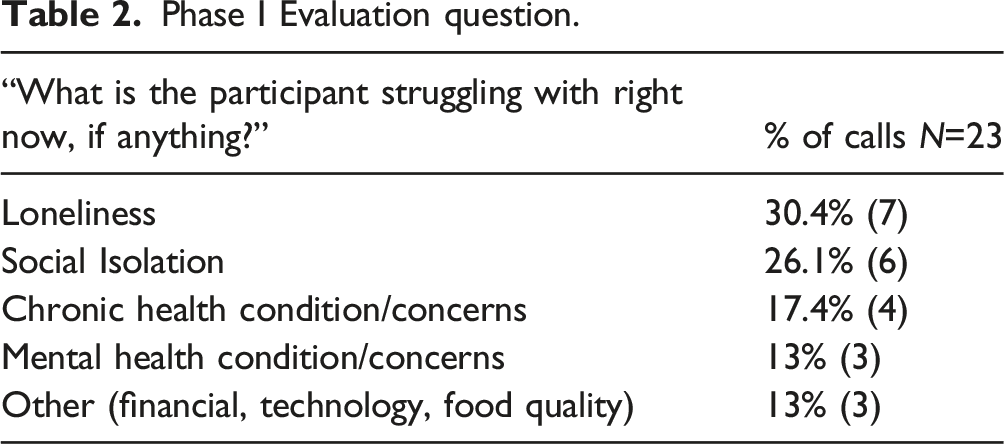
Phase I Evaluation question.
Phase II confidential survey: closed-ended and open-ended responses.

Open-ended responses: how the program eased participants’ loneliness or increased their sense of connectedness.

Open-ended responses: normalization of feelings, participants’ ease in confiding and how the project impacted their feelings of insignificance.

Open-ended responses: feedback related to tech support.

Open-ended responses: intergenerational and reciprocal aspects of the program.

Open-ended responses: health benefits of the program.

Open-ended responses: program improvement (student turnover and poor relationship initiation and termination).

Discussion
A considerable body of evidence has demonstrated that social isolation presents a substantial risk for increased morbidity, premature mortality and dysregulation of health biomarkers (blood pressure, C-reactive protein and cortisol levels) comparable to the risk associated with obesity, hypertension or daily tobacco use (National Academy of Sciences, Engineering, and Medicine [NASEM], 2020) and is also associated with mental health morbidities such as depression, anxiety and dementia (Hawkley & Cacioppo, 2010; Holt-Lunstad et al., 2015; Stickley & Koyanagi, 2018). The NASEM (2020) report also noted that social isolation is associated with 50% increased risk of dementia, 29% increased risk of heart disease and 32% increased risk of stroke. Loneliness is the term used to connote the discrepancy between actual and desired amounts of social contact and is “characterized by impairments in attention, cognition, affect, and behavior that take a toll on morbidity and mortality through their impact on genetic, neural and hormonal mechanisms” (Hawkley & Cacioppo, 2010, p. 224). It is associated with higher rates of depression, anxiety and suicide and, among heart failure patients, is “associated with a nearly four times increased risk of death, 68% increased risk of hospitalization, and 57% increased risk of emergency department visits” (NASEM, 2020, p. 20).
Social isolation is not unique to the United States; there is an abundance of literature from the international scientific community reporting a growing body of evidence that social isolation and loneliness are impacting health and health outcomes around the world. Two international literature reviews were recently completed in the United Kingdom and in Finland. The Centre of Excellence for Public Health at Queen’s University in Northern Ireland reviewed the social isolation interventions of 33 studies conducted in 21 countries (Fakoya et al., 2020) and Tampere University in Finland reviewed those of 23 studies conducted in 13 countries (Latikka et al., 2021). Both reviews included studies from four continents, and both found that the amount of research on this topic has increased significantly during the past decade.
In the United States, North Carolina (NC) ranks 30th in risk of social isolation for adults aged 65+ (America’s Health Rankings, 2021) and 26.5% of NC residents aged 65+ live alone (North Carolina Division of Aging and Adult Services, 2021). NC also ranks higher than the national average on four of the six most common risk factors for social isolation in older adults, disability, divorced/separated/widowed, independent living difficulty and living below the poverty level (United Health Foundation, 2021).
Although technology use in the older adult population increased 55% from 2000 to 2016, one third of them report never using the internet and rates of smartphone ownership in adults aged 65+ remains 42% lower than that of adults aged 18 to 64 (Anderson & Perrin, 2017). This same study found especially low rates of access and use among adults aged 80+ (Anderson & Perrin, 2017). Anderson and Perrin (2017) also found that adults aged 65 to 69 are much more likely (82% vs. 44%) to report ever going online or to have broadband at home (66% vs. 28%) and roughly four times as likely to say they own smartphones (59% vs. 17%) as their counterparts aged 80+. Challenges in this population related to telehealth and other synchronous digital activities have been reported by many including Shteinlukht (2021) who found that 60% of older adult respondents reported difficulty utilizing digital platforms for virtual appointments. In addition to access and technology usage issues, hearing loss and impaired vision, common in the older adult population, can further complicate digital service accessibility (Graham, 2020).
This excess burden of vulnerability and “digital divide” is further compounded by challenges unique to rural areas. The western North Carolina region has a 44% higher proportion of persons age 65+ than North Carolina as a whole (U.S. Census Bureau, 2021), and, of the 23 counties in the region, 19 (83%) are classified as rural (North Carolina Office of State Budget and Management, 2021). Henning-Smith et al. (2019) found that older rural adults were more than 10% more likely to report feeling left out “often” or “at least some of the time,” and 5% of them reported having no friends at all. In a 2020 study, (Henning-Smith, 2020) found that older rural adults may experience structural barriers to connecting. Notwithstanding the presence of larger social networks than their urban area peers, older rural adults reported higher levels of loneliness.
The disproportionate impact of the digital divide on older adults in rural areas has also been well documented. A Pew Research Center report by Perrin (2019) demonstrated persistent discrepancies in the rates of device ownership (smartphone, computer and tablet) and in the rates of access to broadband internet at home in rural adults (two-thirds) versus urban adults (three-quarters). Rural adults who do have internet access are often unable to participate in synchronous activities such as video-conferencing for telehealth or social calls due to slower speeds and poor connectivity caused by low bandwidth access (Kaur, 2020). Thus, older rural adults were more likely to be left out of any technology-based solutions to meet social and other needs during the pandemic (Henning-Smith, 2020).
The Social Bridging Project was a response to concerns about the potential impact of social isolation on older adults as a result of the COVID-19 pandemic and its concomitant safety measures. The project’s aim was to provide older adult members of the community who were isolated or lonely with a source of social connection, technology support and referrals to needed resources. Our initial hope was that project participants would report an improved sense of social connectedness and decreased feelings of loneliness. After callers reported that some participants expressed embarrassment about their feelings of loneliness, a question was added to assess the project’s impact on increasing participants’ comfort in expressing feelings.
Many studies have demonstrated the impact of the pandemic on rates of social isolation, loneliness, depression and anxiety. (Kotwal et al., 2021; Krendl & Perry, 2021; Luchetti et al., 2020; Peng & Roth, 2021; Shteinlukht, 2021; Tull et al., 2020). Although our survey did not assess participants’ loneliness as it related to the pandemic specifically, a few of the open-ended responses indicated that the program was a timely response during the pandemic: “It was wonderful during the pandemic…It could not have come at a more opportune moment.” Other qualitative feedback indicated that our program made participants feel more hopeful and that they had someone to talk to.
Several studies have examined the association between rates of depression and loneliness and high quality, in-person contact versus telephone or internet-based contact and the data have been fairly consistent. Teo et al. (2015) found that the likelihood of depressive symptoms increased as the frequency of in-person contact (not telephone, written or email) decreased, and Fingerman et al. (2021) reported that in-person contact may have benefits not available via telephone contact. Likewise, Choi et al., 2021 and Hamilton, 2015, found that, in older adults, the association between loneliness and in-person interactions is stronger than that of phone or online-based interactions.
Although there is greater evidence to suggest that high-quality, in-person contact is more strongly associated with depressive symptoms and loneliness, our results align with those of others who have found that phone and internet-based communication may impact rates of loneliness and may be an effective intervention for mitigating it. Hutto et al. (2015) found that engaging in specific types of user-generated social networking communication was associated with decreased rates of loneliness, and Kotwal et al. (2021) found higher rates of social isolation in nearly 4 out of 5 older adults who had minimal video interaction during the pandemic. Data on the effectiveness of phone and internet-based interventions are mixed, but some findings, consistent with those of this study, have indicated this type of intervention may be beneficial. Mohr et al. (2012) and Choi et al. (2014) reported that telephone-based social support interventions may be effective in individuals with depression, and Weinert et al. (2008) documented robust findings from a large randomized controlled trial which found that computer-delivered interventions can lead to reduced feelings of loneliness and depression and can enhance participants’ self-efficacy, computer literacy and chronic disease management. Our findings suggest that a phone-based intervention of this nature may be effective in decreasing participants’ feelings of loneliness and in increasing their sense of connectedness and their comfort in expressing their feelings of loneliness.
This project had notable strengths. The partnership between the university and an area health education center that was focused on primary care in rural communities was critical to the project. The health education center recruited more than half of the participants, many of whom may traditionally be excluded from studies. Both entities recruited students from multiple universities in the region which provided a diverse group of student callers with a wide range of academic pursuits. Our focus on the importance of active listening skills in the caller training was a strength alluded to by several participants: “they listen very well to you”, “she was willing to listen”, “she remembers my grandson’s name,” and “the fact that someone was actually listening.” Likewise, our commitment to providing phone support with few restrictions on the number of calls or on call duration was likely a strength.
There were also limitations. Although wellness callers were instructed to complete the Phase I survey instrument after each call, recall bias may have affected their responses and confirmation bias may have affected their responses to “What is the participant struggling with right now, if anything?” Some responses were not required and permitted callers to skip questions. The Phase II evaluation also had limitations, most notably the sample size. Recall and social desirability bias may have affected participants’ reports of wellbeing, though most of the surveys were completed within 48 hours of their preliminary consent in an effort to reduce the likelihood of recall bias.
Program improvement strategies were reported internally and were omitted from the scope of this paper.
Conclusion
Most of the participants reported feeling “happier or more hopeful” after their calls and that the calls made them feel they had someone who listened to them when they needed to talk. Most also reported that the calls made them feel they had someone to turn to for suggestions about how to deal with a problem. More than half reported the calls made them feel less lonely and reported that, when they felt isolated or lonely, the calls made it easier for them to talk about their feelings. Open-ended questions provided rich data about perceived emotional, physical, technological skill-building, and intergenerational program benefits. Programs like the Social Bridging Project that foster and support intergenerational social relationships between students and older adults may reduce feelings of loneliness and increase social connectedness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mountain Area Health Education Center (MAHEC), The NC Policy Collaboratory and the UNC System Office.
Ethical Approval
This study was approved by University of North Carolina Asheville’s Institutional Review Board (Approval Nos. 1662848-1 and 1745640-1).
Appendix A
Social Briding Project Qualtrics Call Log 1. Caller Name 2. Participant ID 3. Date of Call 4. Did the participant answer? a.Yes and conversation b.Yes but no conversation c.No, no answer and left message d.No, no answer and did not leave message 5. Briefly describe what made the call unsuccessful 6. Are you going to try again? a.Yes b.Maybe c.No 7. Duration of call 8. Participant age a.Unknown b.Approximate age 9. County of residence 10. Participant’s living situation (if known) - select all that apply a.Lives alone b.Lives with 1 or more people c. Lives with person for whom participant is primary caregiver d. Lives in congregate housing (assisted living facility) e.Lives in a rural area f .Other 11. What is the participant struggling with right now, if anything? a. Chronic health condition/concerns b. Mental health condition/concerns c. Other homebound condition d.Social isolation e.Loneliness f. Other event (work accident, auto accident, etc.) g. Frequent falls/fear of falling h. Other, please describe: _____________ 12. If the participant is struggling with a mental health condition, please list it here if mentioned. __________ 13. Which of the following did you provide information about? Please select all that apply; leave blank if none of these. a. Use of technology b. Transportation c. Health care resources (e.g. in home medical equipment, appointment with physician, or where to get a flu shot) d. COVID-19 e. Medication management f. Access to food g. Other 14. Does the participant have reliable access to the internet at home? a. Yes b. No 15. Did you help the participant solve a problem? a. Yes b. No 16. Did you spend much of your time on this call providing some form of social/emotional support and/or just listening? a. Yes b. No 17. Did the participant report feeling better after your conversation? a. Yes b. No c. Unsure 18. Call summary, resource information given, planned follow-up actions, questions or notes: ___________ ________________ 19. If the participant offered any suggestions for improvement in the future, please describe. ______________ _____________
Appendix B
Script: Good morning/afternoon. My name is ___________, and I work with the X to evaluate the calls from our Social Bridging Project. I believe that
Social Bridging Project Participant Survey
Yes
No
Not Sure
N/A
1. Do the calls make you feel you have someone who listens to you when you need to talk? Notes:
Y
N
NS
N/A
2. Do the calls make you feel you have someone to turn to for suggestions about how to deal with a problem? Notes:
Y
N
NS
N/A
3. What do you like most about the calls from our program?
—
—
—
—
4. Do you feel comfortable telling your caller about things that you need to live more safely in your home? Notes:
Y
N
NS
N/A
5. Did the calls help you get any of the things you needed to feel more safe? Notes:
Y
N
NS
N/A
6. How do you think the conversations affected you?
—
—
—
—
7. Do the calls make you feel happier or more hopeful? Notes:
Y
N
NS
N/A
8. Do the calls make you feel less lonely? Notes:
Y
N
NS
N/A
9. If you ever feel isolated or lonely, do the calls make it easier for you to talk about your feelings? Notes:
Y
N
NS
N/A
10. Is there anything you think our program can do better?
Y
N
NS
N/A
11. If yes, what could the program do better?
Thank you very much for answering these questions to help us improve our program. If you have any questions about the survey, please call X at X [removed for blind review]. If you have questions or concerns about your rights as a research participant, you can call the X Institutional Review Board administrator at X [removed for blind review]. If you think of anything else you would like to tell me, my name is___________________________ and my phone number is _____________________.