
Abstract
This investigation aimed to identify parameters of reduced functionality that are responsible for variations in the normal gait cycle. Sixteen older adults (55–85 years; nine males) and eighteen young adults (18–40 years; eight males) were enrolled. Assessments included walking trials, questionnaires, and assessed maximal and submaximal dorsiflexors (DF) and plantar flexors (PF) force. Multiple relationships were found between the muscular capabilities of the ankle and gait variability in older adults. For both the DF and PF muscles, the older adults produced significantly lower maximal force production and higher levels of force variability than younger adults; physical activity (PA) level was also significantly correlated. The reduction in muscular strength was concurrent with increased force variability and deficits in spatiotemporal gait parameters, suggesting an age-related worsening of the central motor control. Our results found that PA engagement could preserve gait quality and independence. These are essential considerations for further research on the cause and reduction of falls in older adults.
Introduction
Healthy control of walking is an essential component of living safe, independent lifestyles (Fielding et al., 2011). Unfortunately, research has found age-related declines in gait performance (Martin et al., 2002; Owings & Grabiner, 2004; Skiadopoulos et al., 2020). Older adult gait is characterized by reduced speed, shorter stride length, wider stride width, and increased stride and step time. Additionally, increased gait variability has been reported in older adults (Boripuntakul et al., 2014; Brach et al., 2005; Callisaya et al., 2010). There are several consequences of gait variability that negatively affect mobility in older adults, including reduced stability and increased fall risk (Boripuntakul et al., 2014; Brach et al., 2005; Hausdorff et al., 2001). The increased fall risk and declining gait performance threaten the health and independence of older adults.
While walking, the muscles of the lower-extremity play essential roles in body support, propulsion, and stability (Sadeghi et al., 2001). Therefore, it is reasonable to speculate that relationships exist between muscular deficits, imbalances, and gait variability. Investigation of joint behavior could provide evidence for a more accurate understanding of the mechanisms that contribute to increased gait variability. The primary ankle muscles, the plantar flexors (PF), and the dorsiflexors (DF) have been examined for their contributions to the performance of almost all activities of daily living, including postural support (Laughton et al., 2003), gait initiation, and gait (Skinner et al., 2015). Therefore, the age-associated increase in force variability in the ankle could impair older adults' function during day-to-day activities and the ability to modulate force to changing environmental demands (Tracy, 2007a).
Physical activity (PA) may also play a pivotal role in gait performance, including aerobic and resistance exercise and everyday PA. Exercise, walking, and increased PA have all been shown to improve health and gait performance in older adult populations (Fielding et al., 2017; VanSwearingen et al., 2011). However, it is unclear if PA would affect the underlying mechanisms contributing to age-related gait performance changes (Brach & Vanswearingen, 2013).
Muscular weakness (Perry et al., 2007), force variability (Barbosa et al., 2020), gait variability (Callisaya et al., 2010; Hausdorff et al., 2001), and low PA (Fielding et al., 2017; Gregg et al., 2000) have been identified as independent factors related to falling in older adults. Despite the potential connection between these factors, there is a need for aging studies to comprehensively examine the relationships between these multiple factors and gait performance. A good understanding of these relationships may inform the development of specific interventions to prevent age-related decline in gait performance. Such data would also provide clinicians with an evidence base for community-based programs designed to maintain mobility and independence.
The present study aimed to examine the relative contribution of multiple factors to age-related declines in gait performance. Additionally, we sought to examine the relationship between PA and the multiple factors that influence gait performance. We hypothesized that older adults would have reduced muscular capabilities and increased force variability compared to younger adults, and these deficits would be related to decreased gait performance. Further, we hypothesized that increased PA would positively affect gait performance across age groups.
Methods
Participants
In this study, thirty-four individuals, sixteen healthy older adults (55–85 years; nine males), and eighteen healthy young adults (18–35 years; eight males) participated. These groups were chosen because previous literature has used older and younger adults as a method of studying aging (Sombric & Torres-Oviedo, 2021; Yee et al., 2019). Inclusion criteria included the following: being independently ambulatory; no history of neurological or musculoskeletal disorders; no report of using medications impairing postural control or gait stability; no prior history of falling; and no more than 300-minutes of weekly, moderate physical activity. The University Institutional Review Board approved all procedures, and all participants provided written informed consent before testing.
Experimental Protocol
A cross-sectional research design was utilized. All participants provided consent before the assessments. Participants completed the Simple Physical Activity Questionnaire (SIMPAQ) and Activities-specific Balance Confidence Scale (ABC) to gauge self-reported physical activity and balance levels. The SIMPAQ, a 5-item questionnaire, is a reliable and valid tool to assess PA levels across several populations (Rosenbaum et al., 2020; Schilling et al., 2018). The SIMPAQ questionnaire considered time spent in bed overnight (Q1), time sedentary, including napping (Q2), time spent walking (Q3), time spent exercising (Q4), and time engaged in incidental activity (Q5), averaged over the past seven-day period. At the beginning of the assessment, participants were given verbal instructions on the testing procedure. Thirty-nine passive retroreflective markers were placed over participants' bony landmarks using the Vicon Plug-in-Gait AI full-body marker system used for motion analysis. Participants performed ten over-ground walking trials at a self-selected walking speed. Kinematic data were collected using an 8-camera motion capture system (VICON, Oxford, UK) collected at 120 Hz. Ground reaction forces were collected at 360 Hz using three force platforms (Bertec Corp, Columbus, OH) embedded within an 8-m walkway. Participants were given a rest period at the end of the gait assessment, and fatigue was assessed.
Maximal force production and submaximal force control of the ankle dorsiflexors (DF) and plantar flexors (PF), chosen because of their direct contribution to stability and propulsion during walking (Loudon et al., 2008), were assessed via a HUMAC NORM system (Isokinetic Extremity System, Computer Sports Medicine Inc, Stoughton, Massachusetts). Once familiarized with the testing procedure, participants removed their shoes and their ankle was placed at a standardized joint position similar to standing vertically. Participants performed three isometric maximum voluntary contractions (MVC) of DF and PF bilaterally. Afterward, participants performed an isometric contraction at three submaximal force levels (5%, 10%, and 20% in a randomized order) relative to their MVC value. The intensity levels were selected based on similar protocols, which suggested these values represent many activities of daily living (Skinner et al., 2019; Tracy, 2007a). Participants were asked to maintain each submaximal intensity for 20 seconds, three separate times, with a 30-second rest interval between each attempt. This process was repeated at random on both the left and right legs.
Data Processing
Dynamometer data on torque, position, and velocity were retrieved from the Humac NORM system (Humac2007, v.7.5.0, CSMi, Stoughton, MA). The MVC trial was quantified as the average of the ten force values surrounding the peak force produced during a single continuous isometric contraction. This value was used to analyze and formulate relative intensities for the submaximal force trials. Strength asymmetries were calculated as the percentage difference in maximal strength between legs. Offline processing was performed between 5 and 19 s to allow for a 14-second submaximal force signal. This period was chosen to allow subjects time to acquire the target force and avoid any alterations in force output, as subjects tend to release force prematurely near the force trajectory. These time series represent the steady-state phase of the force production task. The force data were low-pass filtered using a Butterworth filter at 20 Hz (fourth-order dual pass) and detrended to remove any drifting. Force steadiness was defined as the coefficient of variation (CV). CV of force was computed as the standard deviation (SD) of force/mean force output × 100.
Linear measures of gait, including stride length, step time, step width, and walking speed, were averaged across the trials and calculated using standard definitions according to an algorithm programmed in a custom MATLAB program (Mathworks Inc, Natick, Massachusetts). Marker data were filtered using a fourth-order low-pass Butterworth filter with a cutoff frequency of 10 Hz to provide a unitless measure of gait variability within the trial; CV was determined for each gait measure. CV for the force measures was calculated in the same way.
Statistical Analysis
Descriptive statistics were used to characterize the demographics and measured variables. The sample size was based on a priori power analysis utilizing force measures from pilot data investigating force steadiness in older adult populations and its relationship to variability during stepping tasks. An alpha level was set at 0.5, and beta was set at 0.2, and the effect size of interest was set at 0.5 for sample size determination. Paired t-tests were used to determine whether subject characteristics (e.g., mass, activity level, strength asymmetry) were similar between the younger and older adults. The differences of continuous variables between younger and older adults were compared using one-way ANOVA tests. Correlation between strength (maximal isometric PF and DF force), force variability (5,10, and 20% CV of maximal isometric PF and DF force), and spatiotemporal gait variables were assessed using the Pearson coefficient. Pearson’s correlation was also used to determine the association between self-reported PA and the measures of gait and strength.
Results
Demographic Characteristics of Young and Old Adults.
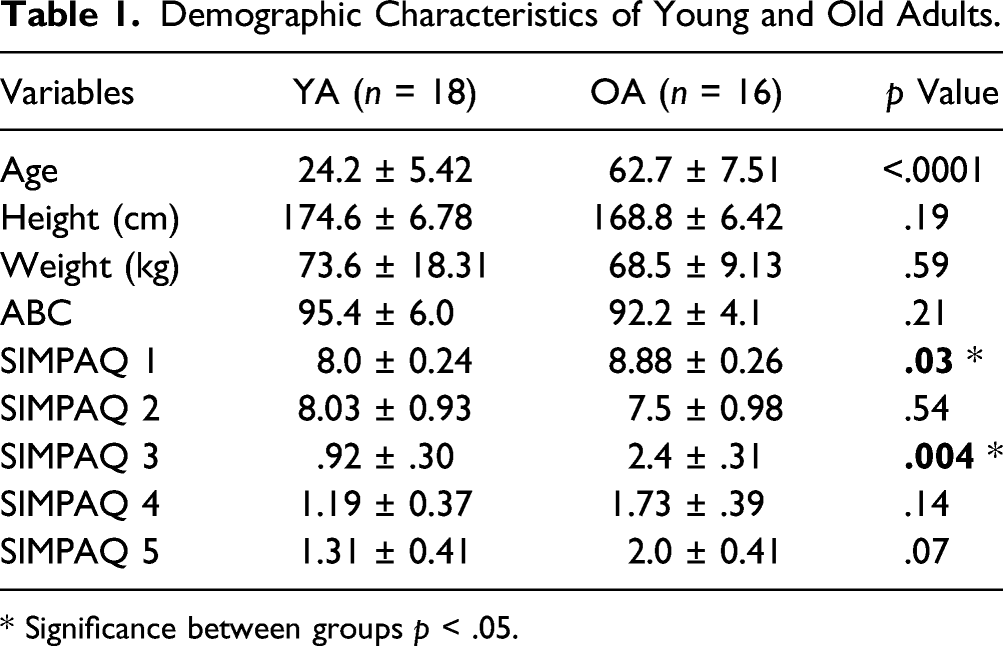
* Significance between groups p < .05.
Self-Reported Physical Activity and Balance
Regarding the SIMPAQ questionnaire, there were no significant differences between questions 2, 4, and 5. However, older adults reported significantly greater time spent in bed overnight and walking than younger adults. There were no differences in self-reported balance confidence. More information can be found in Table 1. (insert Table 1.)
Maximal Force
The maximum isometric force was significantly lower across both muscle groups in older adults than younger adults (p < 0.05). On average, older adults produced 43% less PF force and 28% less DF force than younger adults. Examination of strength asymmetry (Figure 2) found no significant differences between lower extremity strength asymmetry between groups for PF (29% older adults vs. 20% young adults, p = .14) and DF (19% older adults vs. 20% younger adults, p = .87). (insert Figure 2)
Submaximal Force
For the PF muscle groups, there was a significant difference between older and younger adults [F (1, 32) = 6.40, p < 0.05], indicating that the older adults produced higher levels of force variability at 5% MVC than younger adults. Similar findings were found at 10% MVC [F (1, 32) = 9.97, p < 0.05] (Figure 1). No statistically significant difference was noted at 20% MVC [F (1, 32) = 4.04, p > 0.05]. For the DF muscle groups, there was a significant difference between groups at 5% MVC [F (1, 32) = 6.16, p < 0.05]. Again, similar results were found at 10% MVC [F (1, 32) = 7.59, p < 0.05], but not 20% MVC [F (1, 32) = 3.56, p >.05]. Force steadiness (coefficient of variation) of submaximal MVC. *Significance between groups.
Gait
Differences in Spatiotemporal Gait Variables between Younger and Older Adults.

*Significance between groups p < .05.
Gait Variability
Analysis of spatiotemporal gait variability revealed that older adults exhibited higher cadence [F (1, 32) = 6.25, p < 0.05], step width [F (1, 32) = 5.89 p < 0.05], and step duration [F (1, 32) = 8.01, p < 0.05] variability than the younger adults. (insert Table 2.)
Correlation between Force Measures
For strength measures, significant, negative, high-strength correlations existed between max PF strength and 5% MVC (r = −.71, p = .04) and 10% MVC (r = −.79, p = .01). Additionally, significant, negative, high-strength relation existed between max DF strength at 5% MVC (r = −.71, p = .03) and a moderate association between 10% MVC (r = −.52, p = .15).
Correlation between Force Measures and Gait Performance
Correlation Coefficients (r) Between Muscle Force Control and Spatial and Temporal Gait Variability.

*A significant correlation (p < 0.05).
**A significant correlation (p < 0.01).
Correlation between Physical Activity Levels and Force Measures and Gait Performance
Correlation Between Physical Activity Levels and Force Measures and Gait Performance.

*A significant correlation (p < 0.05).
**A significant correlation (p < 0.01).
OA = Older Adult; PF = plantar flexor; DF = dorsiflexor.
No significant correlations were observed in the younger adults.
Discussion
The purpose of the current study was to examine how aging affects 1) maximal force and force control during ankle plantar flexion and dorsiflexion, 2) spatiotemporal gait performance, and 3) the relationship between force control and gait performance in healthy older adults. Reduced joint torque and increased force variability across submaximal intensities at the ankle were observed in older adults compared to younger adults. Older adults' gait performance was impaired compared to younger adults. Lastly, there were several significant relationships between the muscular capabilities of the ankle and gait performance, and several of the muscular and gait variables had significant relationships with PA. To our knowledge, this is the first investigation to examine the relationship between muscular variables and gait performance and how they are related to physical performance in older adults.
Reduced Muscular Capabilities in Older Adults
Reduced muscular capabilities in older adults are related to impaired lower extremity function (Tracy & Enoka, 2002), mobility limitations (English & Paddon-Jones, 2010), and poorer health-related quality of life (Halaweh, 2020). Understanding these limitations and which muscle groups they affect is imperative for adults 65 years and older to preserve functionality and independence. Our investigation examined the muscles surrounding the ankle because of their substantial role in walking, specifically PFs involvement generating forward acceleration (Meinders et al., 1998) and DF involvement during heel strike upon initiation of the stance phase and throughout the swing phase (Capaday, 2002). Our investigation found that older adults produced significantly less isometric force during PF and DF. In agreement with our findings, Thelen et al. found that maximal isometric PF strength in the older adults was 24–32% smaller than the younger adult group, and maximal isometric DF was 14–21% smaller than the younger adults (Thelen et al., 1996). Tracy et al. investigated ankle PF and DF strength and observed reduced ankle strength in the older adults (Tracy, 2007b). However, in their investigation, the ankle impairments were limited to the PF. Our findings are consistent with Tracy and other prior literature; muscle strength and force fluctuations during low-force contractions are impaired in ankle plantar flexors, but not dorsiflexors (Christou & Carlton, 2001; DeVita & Hortobagyi, 2000). However, there is a lack of agreement in the existing and current research on the magnitude, degree of impairment, and which muscle groups are most impacted by aging (Anderson & Madigan, 2014; Carabello et al., 2010).
Our investigation also examined the percentage difference in strength for a specific muscle group on the right and left sides. Strength asymmetry has been identified as an independent predictor of falling (Perry et al., 2007) and has also negatively impacted gait speed (Laroche et al., 2012) and functional tasks (Carabello et al., 2010). Strength asymmetry exists in both older and younger adults; however, older adults' asymmetry can be 10–15% greater (Carabello et al., 2010; Laroche et al., 2012; Perry et al., 2007). We reported no difference in strength asymmetries between groups for PF or DF (Figure 2). Additionally, our results suggest that self-reported time spent walking was related to decreased strength asymmetry in the older adults, suggesting that increased time spent walking prevented the physiological deconditioning present in those with more sedentary lifestyles. Force asymmetry from maximal isometric force testing.
The age-related increase in force variability has been observed in the low force range. It has been observed across multiple muscle groups for the first dorsal interosseus (Vaillancourt et al., 2003), elbow flexors (Prodoehl & Vaillancourt, 2010), knee extensors (Christou et al., 2003; Tracy & Enoka, 2002), and ankle plantar and dorsiflexors (Prodoehl & Vaillancourt, 2010). Investigations have reported force variability in relative MVC during isometric and dynamic tasks. Vaillancourt et al. observed more variable force contractions in older adults at 5, 10, 20, and 40% of their MVC in isometric and dynamic (sine wave) tasks than younger adults control subjects (Vaillancourt et al., 2003). An essential finding of the current study was that the observed reductions in maximal PF and DF forces were accompanied by increased force variability across the lower submaximal intensities at or below 10% of MVC for older adults. Similarly, Tracy et al. found that the CV of force was greater in the elderly than young adults at the 2.5 and 5% MVC forces and was similar between age groups at 10, 50, and 80% MVC, indicating that force control in older adults is significantly impaired at lower % MVC (Tracy, 2007a).
Previous literature associated increased force variability with older adults to the relative contribution of neural activity (Christou, 2011; Tracy, 2007a), supporting our findings on force variability. Prior research has observed that the variability in the discharge rate of single motor units contributes to the greater force output variability of the older subjects (Vaillancourt et al., 2003). Laidlaw et al. extend the prior observation that older adults have greater motor unit discharge variability and greater force output variability than young adults during submaximal contractions (Laidlaw et al., 2000). In the current investigation, our results show an age-related negative relationship between maximal force and submaximal control at a lower percentage of maximal force. Our results may be due to neurological changes, which affect maximum voluntary force production and force control. The shift in the relative contribution of neural recruitment, firing rate, and possible elevated coactivation of antagonist’s muscles contribute to reduced force production and increased force variability in older adults (Hortobágyi & Devita, 2006; Suetta et al., 2007). Based on current evidence, the age-associated augmentation in force variability can impair the ability even of healthy older adults to modulate force to changing environmental demands and could consequently compromise their independence.
Decreased Walking Performance in Older Adults
Walking is one of the most frequently performed activities in daily life. Examining spatiotemporal walking characteristics can provide insight into physical function, quality of life, and health status (Garcia-Pinillos et al., 2016; Hollman et al., 2011). Our investigation found significant differences across gait parameters between older and younger adults. Older adults presented with a slower cadence and gait speed than younger adults. Several investigations have found that elderly populations tend to develop a more cautious gait, characterized by a reduced walking speed, stride length, and increased step width (Herssens et al., 2018). Our results suggest that age-related decline of muscular capabilities at the ankle could contribute to the decreased walking performance observed in older adults. Several investigations have supported this hypothesis showing that reduced muscular strength could negatively impact gait performance (Anderson & Madigan, 2014; Uematsu et al., 2014). The observed changes in gait performance result from compensatory strategies to increase stability and prevent falls from adapting to the physiological changes that occur with aging (DeVita & Hortobagyi, 2000; Hortobágyi & DeVita, 1999).
Age-related differences in spatiotemporal variability measures were observed in the investigation. Compared to the younger adults, older adults had increased temporal variability (cadence and step duration) and spatial variability (step width). The observed increase in gait variability may represent a decline in the automaticity of stepping during normal gait due to a worsening of centrally mediated motor control. The differences in locomotor variability between elderly and young walkers have been previously demonstrated. Guimares and Isaacs found a more variable step length in the elderly when compared to a young group (Guimaraes & Isaacs, 1980). Grabiner et al. observed higher variability in stride width, stride time, stride length, and velocity and increased stride width variability in older adults (Grabiner et al., 2001). There has been a reported increase in spatiotemporal variability in older adults compared to younger adults, which may be a result of loss of lower extremity strength, variable muscle firing rate, a decline in central motor control, or worsening in the automatic stepping mechanism (Barbosa et al., 2020; Callisaya et al., 2010; Laroche et al., 2012). Our results partially match those of previous investigations. The seemingly conflicting findings may indicate a diverse spectrum of older participants or the limited statistical power associated with the small samples.
Relationships Between Gait, Force Control, and Physical Activity
The age-related increase in variability applies to both muscle and physical function. A primary aim of this investigation was to examine how aging affects the relationship between force variability and gait variability. Our results showed that increased force control was related to increased levels of gait variability in older adults.
Interestingly, PF and DF force control was independently related to specific components of gait variability. Force control, at 5%, for PF, was related to temporal components of gait variability; cadence and step time. Alternatively, force control at 10% was related to spatial components of gait variability; step length and step width. The functional role of the plantar flexors and dorsiflexors during the gait cycle is distinct; however, they must work in parallel for a safe and efficient gait. The current evidence suggests an association between aging and functional decline in the PF and DF. It should be noted that no relationship was found between gait variability and force control for the younger adults. Thus, highlighting the susceptibility of each muscle group to unique deficits associated with aging.
Inactivity has been related to aging and is a pivotal contributor to disease in older adults (McPhee et al., 2016; VanSwearingen et al., 2011). Therefore, we sought to explain our results by analyzing self-reported PA. Interestingly, in the older adults, self-reported time spent walking, participating in exercise, and doing chores was associated with improved spatiotemporal gait and muscular strength variables. Furthermore, there were no reported differences in balance confidence between older and younger adults. These results suggest that increased PA could preserve walking and ankle function in older adults; however, further research is needed to examine if these results are dose or mode-dependent.
There were several potential limitations in the research. First, force data were only collected from the ankle’s dorsiflexor and plantar flexor muscles. We do not discredit the role of the hip or knee during the gait cycle; however, we chose to solely include the ankle due to its pivotal role in propulsion during the gait cycle. In order to develop a comprehensive understanding of force and gait performance components, future investigations should incorporate all significant muscles surrounding the lower body joints.
We recognize that PA levels recorded through questionnaires may not accurately reflect the domains assessed in this investigation. Future studies should employ activity tracking, activity journals, or sleep monitors to acquire more accurate quantitative variables. Although our study found many significant correlations, we recognize that this study had a relatively small sample size, and our older adults age group did not exceed 85 years of age. Herssens et al. reported that most measures related to gait variability were confined to an elderly cohort above the age of 70 (Herssens et al., 2018). Future investigations should include a broader age group to accurately reflect age-related performance measures and capabilities.
Conclusion
The purpose of this investigation was to identify parameters indicating reduced muscle functionality that are responsible for variations in the normal gait cycle. The results indicated an age-related decline in ankle strength and reduced force steadiness compared to younger adults. These deficits extended into decreased gait performance and increased gait variability. Lastly, physical inactivity was related to several domains of functionality, both in muscular and gait performance. As a practical application, these findings should be considered in designing interventions to reduce specific symptoms of aging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval of this study was obtained from Appalachian State University IRB [20-0078]