
Abstract
The purpose of this study is to develop candidate common data element (CDE) items related to clinical staff training in long-term care (LTC) homes that can be used to enable international comparative research. This paper is part of the WE-THRIVE (Worldwide Elements to Harmonize Research in Long-Term Care Living Environments) group’s initiative which aims to improve international academic collaboration. We followed best practices to develop CDEs by conducting a literature review of clinical staff (i.e., Regulated Nurses, Health Care Aides) training measures, and convening a subgroup of WE-THRIVE experts to review the literature review results to develop suitable CDEs. The international expert panel discussed and critically reflected on the current knowledge gaps from the literature review results. The panel proposed three candidate CDEs which focused on the presence of and the measurement of training. These three proposed CDEs seek to facilitate international research as well as assist in policy and decision-making regarding LTC homes worldwide. This study is a critical first step to develop candidate CDE items to measure staff training internationally. Further work is required to get feedback from other researchers about the proposed CDEs, and assess the feasibility of these CDEs in high and low resourced settings.
As the global population ages, the spotlight is on long-term care (LTC) homes (e.g., care homes, nursing homes) to meet the needs of older adults with multiple complex and chronic conditions (Beard et al., 2016). Staff training is a widely accepted method to build staff capacity with broad-reaching benefits for residents (Alzheimers Disease International, 2013; Fujisawa & Colombo, 2009; Hussein & Manthorpe, 2005; Spector et al., 2016). Staff training involves programs (e.g., in-services and workshops) offered by the workplace that impart a set of specific skills or knowledge to improve employee performance in certain areas and settings (Davis & Lundstrom, 2011; Saponaro & Baughman, 2009). Such training augments and enhances individuals’ knowledge, understanding, behaviors, skills, values, and beliefs (Davis & Lundstrom, 2011). Training, alongside other professional development opportunities, can also improve societal perceptions of careers in LTC homes and therefore attract and retain more people to the sector (Fujisawa & Colombo, 2009; Hussein & Manthorpe, 2005).
LTC homes are defined as facilities certified within their countries to provide continuous nursing care and personal support to residents that include assistance with their activities of daily living and complex health conditions (National Institute on Ageing, 2019). This care is often provided by informal caregivers (e.g., family members) and clinical staff. The current paper will focus on clinical staff defined as staff who are formally trained and employed part- or full-time by LTC homes (e.g., Registered Nurses, Registered Practical Nurses, Licensed Practical Nurses, and Health Care Aides/Personal Support Workers/Nursing Aides) to provide direct patient care. As clinical staff provide direct patient care, inadequate workplace training can negatively impact staff’s attitudes and skills, the quality of care provided and worsen health outcomes for older people residing in LTC (Cooper et al., 2016). While preparatory education may encourage individuals to potentially seek employment in LTC, this paper is focused on supporting the clinical staff in LTC by means of on-the-job training which may be associated with staff retention, and the ability to enhance the quality of care and quality of life for residents in LTC (Caspar et al., 2016; Fujisawa & Colombo, 2009; Kane, 2003; Spector et al., 2016).
Staff Training in LTC: Challenges for International Research in LTC Homes
The provision of staff training in LTC is met with logistical and methodological challenges; first, previous research indicates that the variability of the LTC workforce, such as their professional backgrounds, cultural and sociodemographic characteristics, and educational levels, coupled with high rates of LTC staff turnover of an aging workforce in LTC, complicates the process to provide training (Fujisawa & Colombo, 2009; Hussein & Manthorpe, 2005). Second, while staff training is often prompted by the care needs of the residents in the LTC home, current training often fails to scaffold on current knowledge and inadequately addresses the knowledge, skills and competencies required (Stone & Harahan, 2010). Third, the OECD (Fujisawa & Colombo, 2009) has reported significant within and between country differences in the availability of the content, duration and emphasis on on-the-job training versus theoretical learning in training programs for LTC staff. Lastly, from a resource perspective, individual LTC homes’ access to expertise, technology, and time will also influence the number and quality of staff training opportunities.
The lack of a minimum international standard for LTC training is prohibitive to accurately compare country experiences, curricula, and requirements (Fujisawa & Colombo, 2009). Methodologically, the resultant heterogeneity with respect to the training details like frequency, content, modality of delivery (e.g., online or in-person), and evaluation, prevents the aggregation of data to build cross-national evidence about effective training in LTC. Most training initiatives have been in experimental stages in small-scale and/or did not include an evaluation component (Aylward et al., 2003; Beeber et al., 2010; Hussein & Manthorpe, 2005; Kuske et al., 2007). These previous literature reviews referred to the evidence on staff training from a variety of settings and countries to suggest that the effectiveness of training and its long-term impact on resident care remains unclear. In sum, gaps in evidence due to methodological weaknesses, differences in training content, training duration, organizational structures in LTC, and evaluation method makes it difficult to determine what common data elements (CDEs) are important to effective staff training from a cross-national perspective (Beeber et al., 2010; Hussein & Manthorpe, 2008; Kuske et al., 2007). There is a need to create a measurement infrastructure to better understand the current landscape of clinical staff training in LTC homes located in in high and low resourced LTC settings.
International LTC research is a key lever to improve international development, policy, and practice, and more broadly enable the LTC workforce to prepare for the increasingly complex care needs of residents (Corazzini et al., 2019; World Health Organization [WHO], 2011). To this end, the “Worldwide Elements To Harmonize Research In LTC Living Environments” (WE-THRIVE) international group was formed to aggregate cross-country data to support the decision making in LTC (Corazzini et al., 2019; Lepore & Corazzini, 2019). WE-THRIVE aims to identify, develop, and evaluate the effectiveness of ecologically viable CDEs to further mutual understanding and facilitate international research in four overarching domains: LTC context; workforce and staffing; person-centered care; and care outcomes (Corazzini et al., 2019). This paper is a part of a broader body of literature examining the central concepts related to “workforce and staffing” domain (Zúñiga et al., 2019, McGilton et al., 2020). An international approach with CDEs to measure staff training in LTC will facilitate comparative research focused on the role of training in supporting staff and the workforce, and contribute to an international measurement infrastructure (Lepore & Corazzini, 2019).
The purpose of this study is to develop feasible candidate CDE items related to clinical staff training in LTC that can be used to enable international comparative research. This study is a critical first step to develop a small number of candidate CDE items that are ecologically viable to measure staff training in high to low income countries.
Methods
Following the similar approaches of recently published WE-THRIVE work (McGilton et al., 2020), we followed the Best Practices for Identifying Common Data Elements identified by Redeker et al. (2015) which involved: (1) completed a literature review of staff training outcome measures; and (2) convening a group of WE-THRIVE experts to review the literature review results to develop suitable CDEs. This is an iterative process by which the expert panel is convened, and the CDEs are developed based on the evidence over the course of multiple subgroup discussions (Redeker et al., 2015). The process of developing and proposing CDEs is ideally transparent, inclusive, and involves identifying and developing CDEs by national and international experts in the field (Redeker et al., 2015). The discussion points from the expert panel will be described in the results.
Literature Review
A WE-THRIVE subcommittee group focused on the “work staff and staffing” domain advised on the broad research questions and identified search terms to include in the search strategy. A literature review was completed to gain a broad understanding and describe the state of the literature of the “on-the-job training” provided to clinical staff in LTCs around the globe, followed by utilizing expert consensus based on the findings of the literature review. Arksey and O’Malley’s (2005) scoping review framework was used: (i) identifying the research questions, (ii) identifying relevant studies, (iii) study selection, (iv) extracting and charting the data, and (v) summarizing and reporting the results. The expert panel wanted to understand what the evidence to inform the development of CDEs were and asked the following questions: what are the characteristics of training provided to clinical staff in LTC home settings? What measurement tools are used to evaluate the training? Is staff training effective in influencing staff and resident outcomes?
Search strategy
An information specialist conducted a search in July 2019 in four electronic data sources: Medline, Embase, CINAHL, and HAPI. A secondary search was conducted on Google Scholar and only the first 200 results were screened. These databases were selected to cover a broad range of disciplines from various academic sources. The search was limited to peer-reviewed publications that were full-text manuscripts and published in the last 20 years in English.
The search query consisted of terms and their synonyms suggested by the expert panel and the information specialist. Clinical staff include health care workers and professionals like nurses (“Registered Nurses; Regulated Nurses; Registered Practical Nurses; Licensed Practical Nurses), aides (“Personal Support Workers, nursing aids, nursing assistants, care aids”), training (“education”), paired with terms “nursing homes” (“LTC homes; home for the aged”), and measurement (“questionnaire; survey”). Inclusion criteria included studies that quantitatively evaluated on-the-job training on any topic for clinical staff providing direct resident care in LTC home settings. Studies focusing on pre-service education were excluded because WE-THRIVE is focused on building the capacity of the workforce in LTC settings. Citations were imported into Covidence, a web-based systematic review software to remove duplicates, and to conduct the title and abstract relevance screening.
Three research assistants (RAs) with nursing backgrounds alongside the PI (CC) conducted the screening. First, the title and abstract of citations were independently screened by two reviewers, and double checked. Studies that did not meet the eligibility criteria described above were excluded. Reviewers discussed any uncertainties to resolve conflicts related to study inclusion. Next, full-text review of the studies that were deemed relevant was completed. Articles were obtained through University institutional access. For articles that could not be accessed, the corresponding author was contacted to obtain the article. An extraction form in Excel was created based on the discussions and questions from the expert panel and included: author name, publication year, journal name, manuscript type, sample size, demographics of the sample, number of homes participating, research questions or aims, format, duration, and frequency of training, and forms of evaluation of the training, research design, attributes of staff training (training topic, summary of content, type and number of trainers, evaluation measures, follow-up duration), tools used to measure the training, how training is documented, impact of training on any nurse or resident outcomes, source of training funding, and study limitations. Outcomes related to training were included to inform a baseline understanding of the effect of training programs.
Expert panel
The formation of the expert panel has been described elsewhere (Corazzini et al., 2019; Zúñiga et al., 2019). We followed the best practices for identifying and developing CDEs (Redeker et al., 2015), and group processes were established within WE-THRIVE including forming a subgroup focused on the “workforce and staffing” domain comprised of colleague experts from Canada, USA, Switzerland, Sweden, and the United Kingdom. The subgroup held regular quarterly meetings throughout 2019 and 2020 to discuss the staff training literature review search parameters which informed the extraction form described above. Subsequently, the results of the review were discussed with the intention of determining the basic data elements related to staff training that would be applicable and inclusive of low- and middle-income countries (LMICs).
Results
The search generated 356 manuscripts for screening, and after duplicates were removed, 282 manuscripts were left to be screened. Only 47 met the eligibility criteria for full-text screening based on the abstracts. During the full screen, articles that were not relevant were removed (Figure 1 shows the PRISMA flow diagram). Twenty-nine studies were included in the scoping review. Table 1 outlines the study characteristics such as study design, number of sites, analysis methods, and effectiveness of training on outcomes. All the included studies were from high-income countries. Most studies occurred in a single LTC home, or in multiple LTC homes in the same geographical region. The total sample size across all 29 studies included 4,933 staff participants (range = 4–1,076). Nursing Assistants (NAs) were the most common type of learners in 20 of the studies (68.97%) followed by Registered Nurses (RNs) who were involved in 13 of the studies (44.83%).

PRISMA flow diagram for article selection.
Summary of Literature Review Findings.

Note. Abbreviations used based on order of appearance: NH = nursing home; NA = nursing assistant; RCT = randomized control trial; PCC = person centered care; QoL = quality of life; RN = registered nurse; OT = occupational therapist; PT = physical therapist; ADRD = Alzheimer’s disease and related dementias; PE = pain education; HCA = healthcare aide; LTC = long term care; LPN = licensed practical nurse; PSW = personal support worker; AI-C = Apathy Inventory–Clinician version; NPI-NH = neuropsychiatric inventory-nursing home version; ADL = activities of daily living; SW = social worker; CTN = control group; INT = intervention group; ACP = advanced care planning; DCM = dementia care mapping; ME value = mood and engagement value; WIB = well-being and ill-being.
Characteristics of the Staff Training
Table 2 presents the training content, components, formats, duration, funding source, evaluation measures, and instructor. The most commonly taught topic involved dementia care (n = 16) including topics such as caring for residents with dementia through QoL and person-centered care (PCC) training (Ballard et al., 2018; Kemeny et al., 2006), managing apathy and depression in residents with dementia (Leone et al., 2013; Rosen et al., 2002), communication and behavior management with residents with dementia (Burgio et al., 2001, 2002; Magai et al., 2002), nutrition in dementia residents (Chang et al., 2006), restraint use on dementia residents (Huizing et al., 2006), self-efficacy training to prevent staff burnout related to caring for residents with dementia (Mackenzie & Peragine, 2003), pain practices and beliefs in dementia care (Ghandehari et al., 2013) and engaging in advanced care planning (ACP) related conversations with dementia residents (Wils et al., 2017). Two studies each provided training about oral care (Janssens et al., 2016; Williams et al., 2016), nutrition (Crogan & Evans, 2001; Greene et al., 2018), and depression and mental health (McAiney et al., 2007; Smith et al., 2013). Remaining training topics were: communication styles with residents (Soderlund et al., 2014), ergonomics (Peterson et al., 2004), pain management (Jones et al., 2004), staff hand hygiene (Huang & Wu, 2008), PCC (Bökberg et al., 2019), restorative care (Resnick et al., 2009), and behavioral modification (Arco & Du Toit, 2006).
Summary of Training.
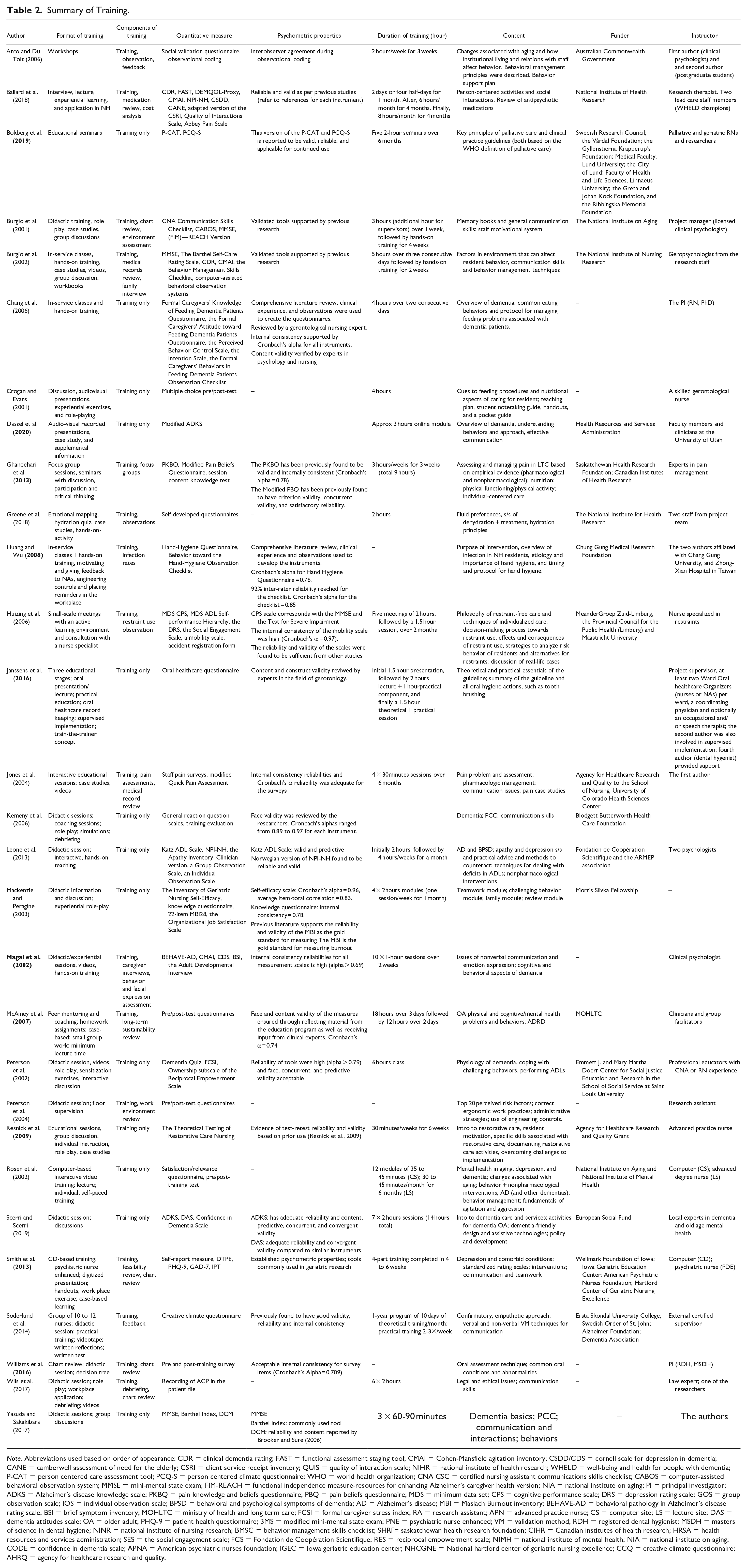
Note. Abbreviations used based on order of appearance: CDR = clinical dementia rating; FAST = functional assessment staging tool; CMAI = Cohen-Mansfield agitation inventory; CSDD/CDS = cornell scale for depression in dementia; CANE = camberwell assessment of need for the elderly; CSRI = client service receipt inventory; QUIS = quality of interaction scale; NIHR = national institute of health research; WHELD = well-being and health for people with dementia; P-CAT = person centered care assessment tool; PCQ-S = person centered climate questionnaire; WHO = world health organization; CNA CSC = certified nursing assistant communications skills checklist; CABOS = computer-assisted behavioral observation system; MMSE = mini-mental state exam; FIM-REACH = functional independence measure-resources for enhancing Alzheimer’s caregiver health version; NIA = national institute on aging; PI = principal investigator; ADKS = Alzheimer’s disease knowledge scale; PKBQ = pain knowledge and beliefs questionnaire; PBQ = pain beliefs questionnaire; MDS = minimum data set; CPS = cognitive performance scale; DRS = depression rating scale; GOS = group observation scale; IOS = individual observation scale; BPSD = behavioral and psychological symptoms of dementia; AD = Alzheimer’s disease; MBI = Maslach Burnout inventory; BEHAVE-AD = behavioral pathology in Alzheimer’s disease rating scale; BSI = brief symptom inventory; MOHLTC = ministry of health and long term care; FCSI = formal caregiver stress index; RA = research assistant; APN = advanced practice nurse; CS = computer site; LS = lecture site; DAS = dementia attitudes scale; OA = older adult; PHQ-9 = patient health questionnaire; 3MS = modified mini-mental state exam; PNE = psychiatric nurse enhanced; VM = validation method; RDH = registered dental hygienist; MSDH = masters of science in dental hygiene; NINR = national institute of nursing research; BMSC = behavior management skills checklist; SHRF= saskatchewan health research foundation; CIHR = Canadian institutes of health research; HRSA = health resources and services administration; SES = the social engagement scale; FCS = Fondation de Coopération Scientifique; RES = reciprocal empowerment scale; NIMH = national institute of mental health; NIA = national institute on aging; CODE = confidence in dementia scale; APNA = American psychiatric nurses foundation; IGEC = Iowa geriatric education center; NHCGNE = National hartford center of geriatric nursing excellence; CCQ = creative climate questionnaire; AHRQ = agency for healthcare research and quality.
Training program duration ranged from a single 2-hour session to a full year’s intervention and follow-up. The most common format was didactic in-person educational sessions in the LTC home. The most common type of trainer were the authors of the studies, with a majority holding clinical psychology titles and/or nurse researchers.
Measurement Tools Used in Staff Training Studies
Table 2 presents all the measurement tools included in the review. Overall, studies used validated, non-validated, or a combination, to measure the effectiveness of training with a lack of consistency of measurement tools between the studies. For example, each of the 16 studies that provided dementia training used a unique combination of tools to measure resident outcomes, and while the majority of studies used validated scales including dementia severity (e.g., Clinical Dementia Rating [Morris, 1997]), behaviors (e.g., Cohen-Mansfield Agitation Inventory [Cohen-Mansfield, 1997], Neuropsychiatric Inventory–Nursing Home (Wood et al., 2000), and depression (Cornell Scale for Depression in Dementia [Alexopoulos et al., 1988]), a small number of studies used self-developed tools to measure staff knowledge and attitudes related to dementia staff training (Chang et al., 2006; Kemeny et al., 2006; Rosen et al., 2002). The heterogeneity of tools is observed across the training topics listed in Table 2.
Effectiveness of Training on Staff and Resident Outcomes
Twenty-eight of the 29 included studies reported staff outcomes (see Table 1). Twenty-five had favorable staff outcomes and three showed no statistical difference (Bökberg et al., 2019; Crogan & Evans, 2001; Huizing et al., 2006). Staff knowledge was the most frequently measured staff outcome that showed statistically significant improvement after the training intervention (n = 15), other studies reported statistically significant improvements in staff confidence and competence after the training intervention (n = 5), staff attitudes after training (n = 3), and staff communication skills after training (n = 3).
Thirteen studies reported on a wide range of resident outcomes (listed in Table 1) related to training and each of these studies reported at least one positive resident outcome. In seven studies, the authors found that resident behavior was positively affected after implementing a training intervention: reduced responsive behaviors (Arco & Du Toit, 2006), increased positive affect (Magai et al., 2002), improved QoL (p = .0042), decreased agitation (p = .0076) and decreased overall neuropsychiatric symptoms (p < .001) (Ballard et al., 2018), and decreased agitation which was maintained at the 3- and 6-month follow-up (p = .01) (Burgio et al., 2002). Additionally, two studies showed that residents had increased independence in self-care activities (p = .04) (Burgio et al., 2001) and improved “dressing” and “transferring” scores on the Katz ADL instrument (Leone et al., 2013) compared to the control groups, after staff participated in a communications training intervention, and apathy training, respectively. Lastly, there were significant reductions in resident reports of constant pain (p ≤ .001) and improvements in resident pain reassessments (p < .05) after staff were provided pain management training (Jones et al., 2004). In a separate study, decreased pain levels in residents were found (p = .006) after staff completed the depression training program (Smith et al., 2013).
Expert Panel Discussion
The literature review results were examined by the expert panel and the salient findings and gaps in knowledge identified by the panel were: (1) staff training was heterogeneous in almost all aspects including content, facilitation, duration, processes for monitoring effectiveness, and measurement tools; (2) the lack of any evidence of staff training in LMICs; (3) the absence of any international collaboration in training, and the local and regional scale of the training that was often limited to one home; (4) there was no macro-level measurement of staff training or indication of how staff training was documented that would allow aggregation of data between LTC homes; and (5) training appeared to be effective and positively influenced a broad range of resident and staff outcomes. Based on these findings, it was clear that there was no extant international measurement infrastructure and that the current literature was exclusive of LMICs; therefore, there was a need to create inclusive and accessible CDEs that could capture basic data internationally.
First, the expert panel acknowledged individual privileges and the discrepancies in resources and staffing as well as differences in system priorities between high, middle, and low-income countries. From this lens, the expert panel required that the proposed CDE candidates be feasible and applicable in a multitude of sociopolitical conditions in order to include data from LMICs. Further, we recognized that due to differences in languages, a CDE with nuanced or complex theoretical concepts may be lost in translation (e.g., self-efficacy as a primarily Western notion may not be easily translated or understood in other cultures) or may not be considered relevant. The proposed CDEs needed to be single-items that were simple, clear, and have face validity in a wide variety of social contexts in order to have buy-in from understaffed or under-resourced settings.
Second, the expert panel discussed how staff training could be reflected in a small number of meaningful CDEs. For example, it was important that training be current in order to keep staff up-to-date with relevant practices. There was further expert consensus that fewer items were preferred to a higher number of CDEs to increase the probability of implementation in high and low-income countries given the complex characteristics of LTC settings. Third, the expert panel discussed the critical need to evaluate the staff training using a validated measure as the literature review suggested that training has positive staff and resident impacts, but several studies reported their own unstandardized instruments. The expert panel considered the quality of the measurement tool and included the aspect of using standardized measurement tools to ensure that the same information can be gathered, compared and aggregated about staff and residents. To this end, the expert panel determined that CDEs focused on the presence and the measurement of staff training will begin to fill a current international data gap. Lastly, the expert panel discussed that the permissible values should be binary “yes” or “no” rather than Likert scales or scales that use terms with room for interpretation (e.g., “sometimes,” “often”). The CDEs needed to be accessible, feasible, clear, and not resource-intensive to answer in order to increase their likelihood of implementation into LTC settings.
From the WE-THRIVE expert panel discussions described above, the members focused on the necessity of basic data elements, that is, the presence and measurement of staff training related to staff and resident outcomes in LTC as an initial step to conduct cross-country comparative research. Therefore, three candidate CDEs were suggested to lay the groundwork for this critical knowledge building. The suggested CDEs are: (1) “was there institutional training provided to staff in the last 12 months?” with a binary choice of “yes” or “no,” followed by (2) “was there evaluation of a staff-related outcome using a standardized measure?,” and (3) “was there evaluation of resident-related outcome using a standardized measure?” both with a “yes” or “no”. This critical knowledge will support LTC workforce needs and continue to contribute to evidence related to staff training, which may inform the development of policies for a sustainable and equitable LTC system which are needed (United Nations, Department of Economic and Social Affairs Population Division, 2019; WHO, 2017). It is important to note that these are proposed CDEs are an initial starting point, and subject to change according to the emerging literature and future ongoing consultations with the broader academic and LTC community.
Discussion
This work presents the process of developing CDEs related to staff training in LTC homes; a literature review about staff training was completed, and the results were presented and discussed by an international expert panel as part of WE-THRIVE’s “Workforce and Staffing” subgroup. Best practices and a systematic method combining evidence in expert opinion were used to develop the candidate CDEs. The literature review results illuminated significant heterogeneity in staff training and use of measurement, a paucity of any international collaboration to evaluate staff training in LTC, as well as an absence of evidence about staff training from LMICs. The expert panel determined that a greater baseline understanding about whether training is provided and measured across different jurisdictions and countries is critical to understand inequities in professional development opportunities. A macro-level measurement infrastructure that can be applied to high- and low-income countries will begin to inform the development of LTC staff training benchmarks and quality standards aimed at ensuring research integrity, public accountability, and equitable allocation training.
Considerations from the expert panel about the quality of measurement tools used is consistent with previous staff training literature. Concerns with measurement have been longstanding in previous reviews of staff training programs in LTC (Aylward et al., 2003; Beeber et al., 2010; Kuske et al., 2007), and there is a consensus for a greater need for more rigorous evaluation of training with validated and standardized tools. Proposed CDEs that are explicit about the use of standardized tools may motivate more robust measurement and emulate the aspirational values of WE-THRIVE to build capacity and support cross-country research.
Significance and Next Steps
The WE-THRIVE initiative seeks to facilitate international research in order to support high quality of care for older adults and comparative research in LTC, such that findings between different researchers in diverse countries can be seamlessly pooled to create appropriate policies and interventions for LTC staff training (Corazzini et al., 2019). The findings of the current review can aid in the creation and development of appropriate LTC strategies and documentation related to staff training (Lepore & Corazzini, 2019). Accurately capturing such foundational data can benefit policymakers to create guidelines and benchmarks about staff training, and also help inform LTC home administrators about resource allocation. For example, if the proposed CDE data about staff training was collected and shared between regions, it could promote a greater understanding about the degree of capacity building and effects of staff training for staff and residents.
The iterative process and stakeholder engagement are critical elements to the successful development and use of CDEs according to Redeker et al. (2015). The input of stakeholders in the development and use of CDEs promotes harmonization nationally and internationally (Choquet et al., 2015; Redeker et al., 2015). We plan on engaging in dialogue and discussions with the researchers and LTC stakeholders to get feedback about the proposed CDEs and the feasibility of these CDEs. Future directions include efforts to advance the development of CDEs through continued international research as part of WE-THRIVE. Further investigations are required to examine if the proposed CDEs are able to be translated across cultural, geographical and institutional barriers, as well as how the proposed CDEs will improve data quality and opportunities for comparison between international researchers.
Strengths and Weaknesses
One strength of this review is in the robust approach of expert consultation based on the diverse group of researchers from the WE-THRIVE initiative. Another strength is that we used a systematic approach when conducting the literature review that included a search generated by an information specialist spanning the last 20 years, and independent reviewers who completed the full-text screen and extractions. The search was limited to English only titles which may have excluded training programs from non-English speaking parts of the world. Additionally, publication bias could be a limitation as training that was not found to positively influence outcomes may not have been published. Lastly, although there are dozens of countries represented in the WE-THRIVE group, not all countries are presented in the panel, specifically countries in the Global South and Africa. The expert panel was composed of experts from high-income English-speaking countries. Moving forward, WE-THRIVE has active online campaigns to strongly encourage researchers in LTC from LMIC and non-English speaking countries to participate with the WE-THRIVE initiative and the workforce domain to ensure the selected LTC CDEs are relevant and applicable to these contexts.
Conclusion
In summary, this paper presented a systematic process by which an international expert panel proposed three CDEs as part of the WE-THRIVE CDE initiative to advance international research related to staff training in LTC. Proposing appropriate CDEs can bolster comparative research and create the evidence-base for policy and LTC decision-making. The three candidate CDEs proposed are accessible, feasible, and intended to be ecologically viable in LMICs in order to fill current knowledge gaps to evaluate staff training. Researchers must continue to be mindful that observed differences in training across countries are likely influenced by social policies and context specific to each jurisdiction, thus continuous assessments are required. These proposed CDEs are positioned as the starting point for staff training, and are subject to change based on new evidence, feedback from LTC stakeholders, and the cultural, political, and institutional changes that may occur.
Footnotes
Acknowledgements
The authors would like to acknowledge the guidance and support of Drs Kirsten Corazzini and Michael Lepore, co-chairs of the WE-THRIVE consortium.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.