
Abstract
This study describes and provides qualitative analysis of an innovative, inter-professional (IP) geriatrics curriculum focused on team-based care with healthy older adults in a home-based community setting. The curriculum consisted of five, four-hour didactic and experiential sessions over one academic year. Dental, medical, occupational therapy, pharmacy, physical therapy, and physician assistant students were placed into teams led by IP faculty from each health professional school. Teams met with a community-dwelling older adult three times. At the program’s conclusion, students responded to the reflective question “What is the most important learning experience you expect to take away from the geriatric inter-professional training? A qualitative analysis of student responses revealed four common themes from all five professions aligning with curricular goals: (1) health professional roles/scope of practice, (2) geriatric care and health outcomes, (3) team communication/collaboration, and (4) advocating for one’s own profession. As sites for institutional clinical training become scarcer for health professions’ trainees, this study offers both a novel, IP, geriatrics curriculum with didactic/experiential learning through community partnerships in a home-based setting and a reflective evaluation.
Introduction
The worldwide growth in the older adult population is increasing, impacting higher-, middle-, and low-income nations (Abegunde et al., 2007). The socioeconomic and health implications of this aging trend is significant with the vast number of the aging population occurring in less developed countries (Global Health and Aging, 2020). The growing older adult population requires a healthcare workforce that is trained and prepared to meet the needs of this population (Crisp & Chen, 2014; Ortman et al., 2014; Retooling for an aging America: Building the health care workforce, 2008). There is increased focus by health professional accreditation bodies on the importance of inter-professional care. Additionally, there is a lack of health professions education both in geriatrics and interdisciplinary team training across multiple disciplines and in non-institutional settings. Interprofessional (IP) team training in geriatrics has been called “an essential component of quality healthcare for older adults” (Partnership for health in aging workgroup on interdisciplinary team training in geriatrics, 2014, p. 1) and the ability to work in interdisciplinary teams has been identified as a key competency for all health professions (Core competencies of the interprofessional collaborative practice, 2011). Training an IP health team will be critical to meeting the community-based health shortage needs of the aging population (Weiss et al., 2019).
IP education is essential to the development of skills necessary to deliver care in a team environment. Team-based care is designed to address the complexity of medical needs and one way the health care system is attempting to respond to the growth in the number of people with chronic illnesses (Partnership for health in aging workgroup on interdisciplinary team training in geriatrics, 2014; Weiss et al., 2019). Further, an aging population demands a broader spectrum of medical professionals educated in team-based care and multi-system disease management. The older adult population therefore provides an ideal population for IP education and training.
Studies over the past several decades have reported various geriatric educational models for health professions trainees. No one approach has been shown to be more effective in improving geriatric knowledge or generating a positive attitude toward care of older adults (Reilly et al., 2014). For medical students, these models have included a 1-week geriatrics experience (Duque et al., 2003), an intensive 8-day course (Hughes et al., 2008) a mentoring program that introduced medical students to healthy older people (Bernard et al., 2003) case-based problem-oriented modules in transitions of care (Baloguin et al., 2015) and a community clinic geriatric rotation (Rosher et al., 2001). Additional approaches included geriatric lectures, workshops and conferences (Ford et al., 2014), geriatric lecture/homework discussions with nurses and general practitioners (Oeseburg et al., 2013), and a geriatric medicine module with large group teaching, small group interactive workshops and small group discussion (Koh et al., 2012).
A smaller body of literature exists about geriatrics training programs for other health professions students. Pharmacy student geriatrics training is largely didactic and simulation-based (Adkins et al., 2012). Studies demonstrate that dentistry students receive geriatrics experiential and clinical exposure, rather than didactic training (Formicola et al., 2012). Geriatric training of physical therapy students has focused on service learning experiences (Beling, 2003). Experiential and classroom/workshop geriatric training has been used in the curricula of occupational therapy, physical therapy, and physician assistant students (Kelly, 2003; Koh et al., 2012; Rask et al., 2007; Wilkins & Rosenthal, 2001).
There is an emerging body of literature with IP experiential, innovative models for team training of students in the care of older adults. The current efforts are largely led by Geriatric Workforce Enhancement programs (GWEP) grants, designed to increase funding resources to train a geriatric IP workforce. The existing inter-professional (IP) geriatric educational curricula are experiential, didactic, case-based and the clinical exposure is largely institutional (Keijsers et al., 2016; Schapmire et al., 2018). The most well-known is the Geriatric Interdisciplinary Team Training (GITT) Program, funded by the John A. Hartford Foundation, where health professions students receive didactic education and then apply it in an experiential clinical scenario using trained standardized patients (Fulmer et al., 2005). The Collaborative Inter-professional Team Education (CITE) training program was developed to assess team health professions students education and its impact on attitudes toward older adults in social work, nursing, medical, and pharmacy students (Bridges et al., 2011). Other IP team-based geriatric learning has included a virtual school and a multi-disciplinary quality improvement project with nurses, social workers and physiotherapists (Bridges et al., 2011; Fulmer et al., 2005; Rask et al., 2007). Still another study examined an osteopathic program with medical students, nurses and a variety of non-traditional health-related disciplines including athletic training, exercise science, and communication studies (McManus et al., 2017). A few smaller studies have utilized home visits as IP training sites with health professional students (Giuliante et al., 2018; Macrae, 2012; McManus et al., 2017; POGOe-Portal of Geriatrics Online Ed, 2016; Reilly et al., 2014).
While the need for inter-disciplinary team training has been well established, the setting in which this training should best occur, which disciplines should be included, the duration of the training, and the specific content of the team training curricula are variable. Further, qualitative data on interprofessional team training is rarely reported in the literature. This paper describes an innovative interprofessional geriatrics training program using a team-based curriculum. The hypothesis is that employing a community focused, didactic/experiential learning model in a home-based setting will provide positive student perceptions of the elderly measured through qualitative analysis of student’s reflections.
Methods
Seventy-two health professions students from six health professions programs (dentistry, medicine, occupational therapy, pharmacy, physical therapy, and physician assistant) at one university participated in the interprofessional geriatric program (IPGP). Student participation was voluntary with the exception of occupational therapy students who received course credit in their department. Students were grouped into 12 teams, each team included six students, one from each discipline. Each student team was randomly assigned by the program coordinator to an older adult resident living in a subsidized housing unit for older adults.
Six faculty participated, one from each of the professional training programs involved in the program. Faculty volunteered to participate, received IP training from didactic workshops and IP faculty certified in a “train-the-trainer” course offered by the Collaborative Change Leadership Program ( https://collaborativechangeleadership.ca , 2009).
The IPGP program partnered with two local, low-income senior residential independent living sites with the intention of providing: (1) educational services to the housing site’s older adult residents and (2) for the older adults to serve as “teachers” for the health professional students.
Twelve older adults living in each of the two sites were recruited by the unit housing supervisor and voluntarily participated. Those eligible for the program were (1) over the age of 65, (2) living independently, (3) English-speaking, (4) willing to have a student team come into their home, (5) with cognitive function adequate to interact with the team as assessed by the unit housing supervisor, and (6) deemed most in need of the services offered by IPGP by the unit housing supervisor. Those eligible older adults not participating in IPGP were invited to participate in group health education sessions.
An IPGP coordinator was identified to assist in the management of team and community partnership logistics. In addition to assigning students to teams, the coordinator served as the single point of contact for communication with the students, the facility housing site coordinator and the older adult resident participants.
Measures
A computer-based survey was completed by each student prior to and after the conclusion of the curriculum. Surveys were sent to the students in an electronic format using Qualtrics (Qualtrics, Provo, UT). The pre-program survey documented information about the students’ demographics, year in training, prior exposure to interprofessional education (IPE), prior experience with older patients and assessed attitudes and knowledge about inter-professional and geriatric care. In addition, as part of the pre-curriculum survey, students were asked to respond to the reflective question, “What is the most important learning experience you expect to take away from the geriatric inter-professional training?” The qualitative data were collected and reviewed by two independent reviewers and categorized into common themes.
Curriculum
A multi-disciplinary faculty team developed the IPGP curriculum. It is designed to train students during their health profession training to work as a team in the care of older adults in a community-based senior housing setting. The IPGP objective is to enhance health professional students’ appreciation of the value of collaborative, inter-professional care toward the maximal well-being of the older adult, using a combination of didactic and experiential curriculum. The curriculum focuses on building skills in assessing the broad health care needs of older adults, while providing participants with health education and community resources to meet those needs. This program was in addition to the standard health professional curriculum. The latter included a wide range of didactic, experiential, and clinical training hours that were specific to each health profession program.
Students met five times over the course of the academic year (Figure 1): (1) The first meeting was a four-hour, faculty-directed, intensive orientation workshop that involved all participating students. This session provided an overview of the program including logistics and introduction to each of the community housing sites, a lecture on the essential components of teamwork, and an experiential team-building exercise. It also included an opportunity for the students to educate one another about each of their respective disciplines, specifically how their knowledge and roles overlapped and how they were different. Communication skills, “home visit” skills/expectations and challenges to IP teamwork were addressed. (2) This was followed by three 4-hour student team meetings held with their older adult resident over the course of 6 months at one of the two senior housing sites.

IPGP curriculum.
Student Teams
Curriculum
The 12 student teams were divided into two groups so that at any given session, six teams participated with six elderly residents at one site. Each team met with the same resident for each of the three visits. These team visits were facilitated by an IP faculty member. Faculty members rotated teams such that students were exposed to multiple faculty disciplines over the course of the three sessions. (3) Lastly, all participating students met in a final four-hour faculty-directed workshop “wrap-up session” at the end of the curriculum training. During this meeting, teams shared their experiences over the course of the program and offered oral reflections about the interprofessional team-based experience and caring for the elderly.
The three sessions at the senior housing unit each followed a similar structure (Figure 1). A focused, interactive, didactic lecture (session #1: polypharmacy and medication reconciliation, session #2: gait evaluation and memory/cognition assessment, session #3: nutrition assessment and oral health evaluation) was taught by the IP faculty at the beginning of each session. Following the lecture, each team conducted a student-faculty led pre-planning meeting to set goals for the home-visit interaction. After the pre-planning meeting, the student teams visited the older adult resident in their apartment and conducted a team-based interview and assessment focused on the session’s topic. This was followed by a post-visit debriefing session by each team. Lastly, each team shared their visit experience with the larger group.
After the session, students wrote a one-page reflection on their IP experience, reflecting on both their interactions with the older adult and their IP experience. These reflections were emailed to students’ individual discipline IPGP faculty mentor who responded with written feedback. Following the session, faculty met in person and/or via phone, with the housing site coordinator to share needs and concerns that teams identified about the health conditions of the older residents. Faculty helped to communicate with medical providers and facilitate referrals when requested by the resident and housing site coordinator.
Analysis
Answers to the qualitative question were collated and independently reviewed by two IPGP faculty who read the responses and identified common themes. They then conferred with a third faculty and agreed upon four common themes that encompassed all responses. Next, each response was independently scored by the faculty rater for one of the identified themes that best fit the response. Lastly, the number of responses per theme was totaled.
Results
The survey was sent to each of the 72 inter-professional health student participants. Of these, 67 completed the survey, a 92% response rate. This included 11 medical, 10 dental, 11 pharmacy, 11 physician assistant, 12 occupational and 11 physical therapy students. Five student’s data were not included due to student documentation errors. Table 1 shows the demographic characteristics of the participants. Overall, student participants were primarily female (71%) with an average age of nearly 27 years. Half were Asian (50.7%), and 30% were Caucasian, with differences of 8 to 27% in the distribution of “other” ethnic groups (Latino/Hispanic, African American, Native American, and Pacific Islander) between health professional programs. These demographics are representative of each health profession program’s student population.
Demographic Characteristics of the Inter-professional Geriatric Care Students.

Responses to the qualitative question fell within four common themes (Table 2). The most common theme (45%) was (1) learning about the roles and scope of practice of other health professions. This was followed by (2) learning more about geriatric care and geriatric patient health outcomes and (3) learning how to communicate and collaborate with other team members.
Common Themes and Example Quotations.
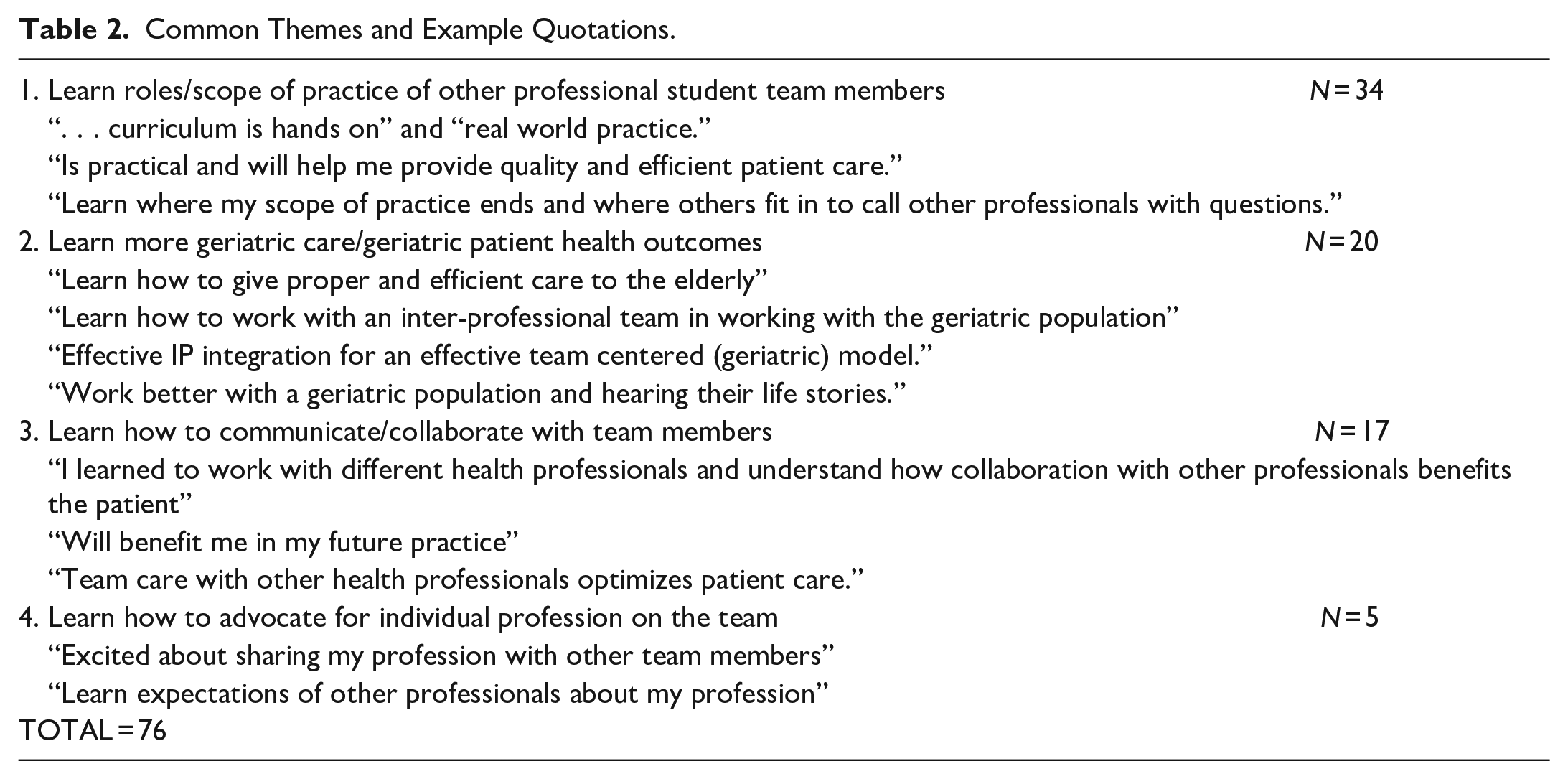
The least common theme, cited only five times, was (4) learning how to advocate for each profession within the team.
Discussion
This paper describes an innovative curriculum to train health profession students through a longitudinal, community–based, geriatric, inter-professional team-based model over one academic year. The themes illuminated by the student expectations aligned well with the goals of the curriculum. This unique curriculum brings together geriatrics and interprofessional team training, two health professional priority areas that do not typically co-exist. It uses a combined didactic and experiential curriculum delivered in an in-home, community-based setting. This training includes multiple health disciplines not commonly exposed to one another, working in student teams with inter-disciplinary faculty facilitation in a non-institutional setting.
Health professions students receive modest geriatrics training but few receive it in a team model or in an experiential, non-institutionalized setting with healthy older adults (Retooling for an aging America: Building the health care workforce, 2008). This combination of geriatrics and team training for health professions students in a community setting provides a model for health professional education. Further, IP team training and IP care also provide more person-centered care, better meeting the complex health care needs of older adults. This model could easily be adopted and adapted for broad use by training programs seeking to improve and increase both geriatric and IP curriculum content.
The majority of geriatric didactic education has occurred in the classroom within a single profession’s curriculum and clinical education commonly occurs in an institutional setting (i.e., hospital, clinic, or nursing home). Most curriculum have used didactic training, standardized patients, DVD training videos, and nursing home based geriatric clinical rotations. In contrast, students in this program work with IP faculty and older adults in direct contact within a community home setting. This model allows for what has been described by the student participants as a rich “real world experience,” an opportunity to move “beyond the classroom” and learn with older adults. The non-institutionalized care opportunity enhances the students’ educational skills in a positive, community, home-dwelling environment with “well elderly.” Geriatric, health professions student home visit team-training is under-reported, has little variability in disciplines represented, small sample sizes, and is not well studied in the literature (Giuliante et al., 2018; Macrae, 2012; McManus, 2017; POGOe-Portal of Geriatrics Online Ed, 2016; Reilly et al, 2014; Steel, 1995). The combination of didactic and experiential curricular exposed students to the unique medical and psychosocial needs of older adults living in a non-institutional setting. The use of IP team training was designed to improve students’ appreciation for the benefits of older adult interprofessional team care. Additionally, IPGP utilized a total of five sessions and student reflections indicated favorably that it met the instructional training goals. This “dose” fit in well with the curricular needs and constraints of multiple IP schools; However, it is not clear that it is the ideal “dose” and needs further study. Lastly, this institution does not have a formal IP health profession’s curriculum across disciplines or an IP institute. IPGP provided a forum however, where students/faculty could meet and form professional relationships and friendships that would go beyond the IPGP.
This geriatric IP training program is unique in several aspects. First, it brings together students from a large number (six) of traditional health professions at one institution for a longitudinal clinical training experience. Second, the curriculum provides a unique lens through which students experience the multi-layered needs and challenges faced by aging adults outside the formal medical care delivery system. Third, the educational program occurs in independent, low-income senior housing units, an under-utilized older adult population for geriatric training and offers students exposure to diverse, immigrant community senior health issues. The model allows the students to see healthy, community dwelling older adults “aging in place,” and fourth, the training gives students an opportunity to do home visits, not a part of most health professional training programs.
At this institution, some occupational and physical therapy students experience home visits routinely as part of their curricula, but the other health profession students’ training lack this exposure as a part of the regular curriculum. Lastly, the community-based model also provided the opportunity for an academic institution to partner with local community organizations for service learning. An unanticipated outcome of the IPGP was that the community housing sites requested the IP faculty provide site staff with additional education and a health fair for the older adult residents.
As medical care moves beyond traditional boundaries, academic institutions need to respond to the changing health care delivery system, and to think creatively beyond the campus and traditional medical institution training sites. The development of partnerships with community organizations for the delivery of education and training programs should be considered a standard model for future health profession student training.
Qualitative team student health professional data such as collected as part of this curriculum, is underreported in the literature. Failure to utilize such data, particularly in both geriatrics and IPE, may miss the richness of such training experiences. In this study, the qualitative data findings are in alignment with the curriculum’s stated goals and objectives. The reflective answers and themes demonstrate that students (1) recognize the value of team care, (2) the need for health professionals to learn how to communicate well with one another, and (3) to increase their understanding of each other’s roles and capabilities. Students’ recognition of the need for more knowledge about the care of older adults provides further support for the value of a team-based geriatric approach to increase students understanding of, care of, and appreciation for the varied needs of the older adult population.
Utilizing a community housing setting for the experience allowed for a comprehensive and collaborative educational assessment of an older adult’s life. Students gained better understanding of the needs of community-dwelling older adults, the unique factors that affect their functioning in a community setting and how the knowledge and skills of their own and other health professions can support better healthcare outcomes. Future studies should consider adapting/exploring this model for an age-friendly university and/or age-friendly health system training paradigm.
Limitations to this study include the absence of nursing students as one of the major health professions categories participating. While nursing is a vital part of an IP team, the lack of a nursing school at the participating institution precluded their inclusion. Further, the older adults participating in our study were healthy/cognitively intact. While this model is not completely representative of a “real world experience” in that it includes only healthy older adult participants, this institution’s experience was that early health IP students struggled significantly with cognitively impaired, institutionalized elderly with chronic/acute health conditions which may have contributed to unfavorable views of older adults. In an effort to train and optimize early IP students experience with seniors, especially those who lacked a foundational clinical experience/communication skill set, healthy older adults were most suitable. Of note, seasoned/trained IP faculty instructors were critical to the success of the course to navigate individual student issues, student IP team challenges, older adult family/community site issues, and the administration of the course. Finally, IPGP utilized a total of five sessions and student reflections indicated favorably that it met the curricular training goals. This “dose” fit in well with the curricular needs and constraints of multiple IP schools; however, it is not clear that it is the ideal “dose” at other institutions and needs further study.
Conclusion
This study describes an effort to train future health care providers in an IP geriatric team care model based in an independent older adult community-housing site. The multiple, complex, and inter-disciplinary needs of older adults offer an ideal training vehicle for both IP and geriatrics. As the global older adult population continues to increase and health profession students across disciplines continue to need training to meet this demand, development of IP geriatrics curricula offers an option to meet these needs. The program described here provides a model that can be easily used and adapted by others to their institutional and local environment. Lastly, our study suggests, there is value in partnering with non-institutionalized community-based organizations to expose health professional students to healthy older adults in a home setting.
Footnotes
Authors’ Note
This study was reviewed by the USC Institutional Review Board and approved as exempt: Keck IRB APP-12-07433 & amendment ID: HS-11-00617-AM001.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Health Resources and Services Administration (HRSA) under grant number UIQHP28740.