
Abstract
Introduction
Nursing home residents are at high risk for pressure injuries (PrIs), localized damage to the skin and underlying tissue, usually caused by prolonged pressure against the skin which can happen when someone is left in the same position for long periods of time (European Pressure Ulcer Advisory Panel et al., 2019). Nursing home (NH) residents living with Alzheimer’s disease or a related dementia (ADRD) are at even greater risk for PrI formation due to the decline in neurophysiologic function, which affects one’s ability to sense pressure/pain and move to offload the underlying tissue from said pressure (Harris-Kojetin et al., 2016; Jaul & Calderon-Margalit, 2015). Approximately 48% of NH residents are diagnosed as having ADRD (Center for Disease Control and Prevention, 2020); and of those, up to 66% are at-risk for PrI development at some point during their stay (Harris-Kojetin et al., 2016; Jaul & Calderon-Margalit, 2015). While regular repositioning is the cornerstone of PrI prevention (and mandated by government regulation) a number of barriers exist to conducting frequent, scheduled resident repositioning. Participation in repositioning activities is difficult for many residents given their limited mobility, sensation, and common behavioral challenges. In fact, up to 90% of residents with ADRD suffer from behavioral issues (Feast et al., 2016), such as agitation, aggression, and apathy. Managing these behavioral expressions is one of the most difficult challenges nursing staff encounter (Finkel & Burns, 2000), and the inability to successfully meet this challenge often results in increased care burden (Mohamed et al., 2010).
Nursing staff in NHs have finite resources and tight, protocol-driven schedules, making PrI prevention care delivery difficult and time-intensive for residents with ADRD who experience fluctuating behavioral and psychological symptoms (BPSD) (Selbaek et al., 2014; Sun et al., 2018). Given the staff’s fixed amount of time to care for each resident, resident preferences regarding care delivery may be overlooked, potentially causing or exacerbating BPSD (Ervin et al., 2014). Past research has demonstrated that BPSD expressions often arise from the incongruence between a person’s needs and the environment (Cohen-Mansfield et al., 2012). Medication is often the first choice for stabilizing moods and managing BPSD (Cohen-Mansfield & Jensen, 2008; Olsson et al., 2010); however, nonpharmacological approaches provided by caregivers, that include both the social and physical environment, have proven effective and have the added value of avoiding adverse effects experienced when using pharmacological intervention (Chenoweth et al., 2009; Cohen-Mansfield et al., 2007; Cohen-Mansfield et al., 2012; Ervin et al., 2014). Resident cooperation is vital for successful repositioning; hence, recognizing and integrating a tailored nursing staff approach can improve resident cooperation and engagement within the fixed amount of time available for providing care (Fazio et al., 2018a; Fossey et al., 2006; Poey et al., 2017; Yoon, 2018). Yet, little is understood about successful repositioning care models for those living with ADRD. This study aimed to better understand nursing staff decision-making processes for repositioning approaches aimed at PrI prevention.
Methods
Design
This was a mixed-method prospective, exploratory design conducted in 3 NHs as a supplemental study to an ongoing clinical trial [3R01-NR016001-04S1; ClinicalTrials.gov: NCT02996331, First registration (12/19/2016)] comparing 2-, 3-, and 4-hour repositioning intervals for PrI prevention across nine NHs. Details are published elsewhere (Yap et al., 2018). Observational data were collected on a convenience sample of NH residents during routine, naturally occurring repositioning events. Focus groups (2 per NH) with nursing staff were convened following completion of parent study data collection.
Setting and Sample
Setting
The study was conducted at 3 for-profit, Medicare-certified, intermediate, and skilled care NHs with >100 beds in the eastern United States participating in the parent study.
Sample
All NH residents were eligible for the additional study and if clinically assessed during routine care as having a Braden Scale for Predicting Pressure Sore Risk© (hereafter Braden Scale) score of 10–12 = high, 13–14 = moderate, 15–18 = mild, and 19–23 = low risk for PrI (Bergstrom et al., 1987a; Bergstrom et al., 1987b). Exclusion criteria included existing PrI, severe risk for PrI (Braden score ≤9 because they had individualized treatments in place such as specialty beds), adhesive allergy, use of specialty beds, or presence of a “do not turn” order.
Nursing Staff
Focus groups consisted of a convenience sample drawn from all eligible nursing staff (irrespective of job category, gender, race, or ethnicity) working clinically full-time or part-time with residents. Staff were recruited using flyers containing the purpose and logistics of the study, as well as by word of mouth and invitations from researchers. Interested participants contacted the researchers in person or by phone if interested in participating in a scheduled focus group.
Measures and Procedures
Electronic health record (EHR) data were extracted to ascertain each resident’s clinically assessed Braden risk score (Bergstrom et al., 1987a), demographics (age, gender, race, and ethnicity), and ADRD status. ADRD was defined as the presence of an International Classification of Disease (ICD) code for Alzheimer’s disease or another dementia diagnosis (with the exception of Huntington’s disease, major depressive disorder, multiple sclerosis, Parkinson’s disease, Batten disease, schizophrenia, and AIDS dementia) (National Institute on Aging). Because it is known that dementia develops over time and is often without diagnosis in early stages, the research team also used the Brief Interview for Mental Status (BIMS) score <12 as a mechanism for early detection of cognitive impairment in residents without a formal ICD10 ADRD diagnosis (Chodosh et al., 2007; McCarten et al., 2012; Saliba et al., 2012; The Gerontological Society of America Workgroup, 2015).
Observations were conducted using an investigator-developed checklist to guide researcher interpretations of routine repositioning events. The checklist was not validated but the same 3 team members collected observational data at all 3 NHs and random inter-rater reliability checks for both resident and nursing behaviors were performed. The checklist was based on current behavioral and psychological symptoms of dementia (BPSD) literature (Cummings, 1997; Gerlach & Kales, 2018; van der Linde et al., 2016), to assess residents’ behaviors and nursing responses. Research team members observed resident/staff during repositioning events throughout the day and evening shifts during the last week of implementation and recorded the observations. Repeated repositioning events performed on the same resident were considered independent, unique events. There was no consistent pairing of staff to residents, and participation in helping reposition residents was random (i.e., often a solicited team effort).
Focus groups provide a broader range of insights than may have been obtained with individual interviews (Krueger & Casey, 2000). All sessions lasted between 45 and 60 min and were held on a single day at each NH. An investigator-developed, semi-structured interview guide was used. Specifically, the interview guide aimed to elicit staff perceptions of 1) the impact residents’ BPSD had on repositioning events; 2) strategies employed to manage challenging resident behaviors; and 3) tailoring required during repositioning events. Two study team members experienced in focus group methods moderated each session, with emphasis placed on facilitating interactions between consented staff participants. The lead moderator provided an overview of the study’s purpose, background, and procedures, such as investigator roles and session recordings; all group members were encouraged to participate in the discussion, and differing views were explored with follow-up probes. All sessions were audio-recorded and transcribed verbatim and imported into NVivo 12.0 (QSR International Team, 2018). Four team members with backgrounds in ICU, gerontological nursing, and organizational science participated in the data analysis and transcript accuracy.
Analysis
Descriptive statistics were used to analyze EHR (resident demographic characteristics and ADRD status) and observational checklist data. Potential differences in resident characteristics within the ADRD vs. non-ADRD groups were analyzed using a Mann–Whitney U test for nonparametric continuous variables, and a Pearson chi-square or Fisher’s exact test, as appropriate, for categorical variables. Differences in behaviors observed between residents with or without ADRD, and differences in nursing approaches toward residents with or without ADRD, were assessed using a Pearson chi-square or Fisher’s exact test as appropriate.
Verbatim focus group transcripts were analyzed using the constant comparative coding method, an inductive qualitative process aimed at establishing clear links between the research objectives and the raw data (Smith, 2000). Open, axial, and selective coding levels were used to examine the discrete elements, reveal categories, and attribute meaning related to information obtained about repositioning events during observational data collection (Figure 1, Qualitative Analysis Process). The working group’s initial step was to use open coding to compare individually coded units of data. Discrete pieces of transcript data were assigned descriptive labels from which categories developed as part of an iterative process. The interconnections of the initial categories were examined during the axial coding stage. Transcripts were reread to validate and clarify initial coding decisions and resolve differences identified in coder discussions and across transcripts. Some categories required revision as the coding team worked to establish coding consistency. Categories were subsequently refined into four themes through the selective coding process. A summative check was conducted for reliability for all transcripts; inter-coder reliability at above 85% was established (Smith, 2000). Qualitative analysis process.
Results
Characteristics of the Sample.

M=mean; SD= standard deviation;
unable to calculate due to small numbers of Hispanic residents.
Observational Checklist Findings
Resident Repositioning Behaviors.

Insufficient number of events for analysis.
Nurse Repositioning Approaches.

Insufficient number of events for analysis.
Focus Group Findings
Themes: Definitions, Supporting Quotes, and Exemplar Strategies.

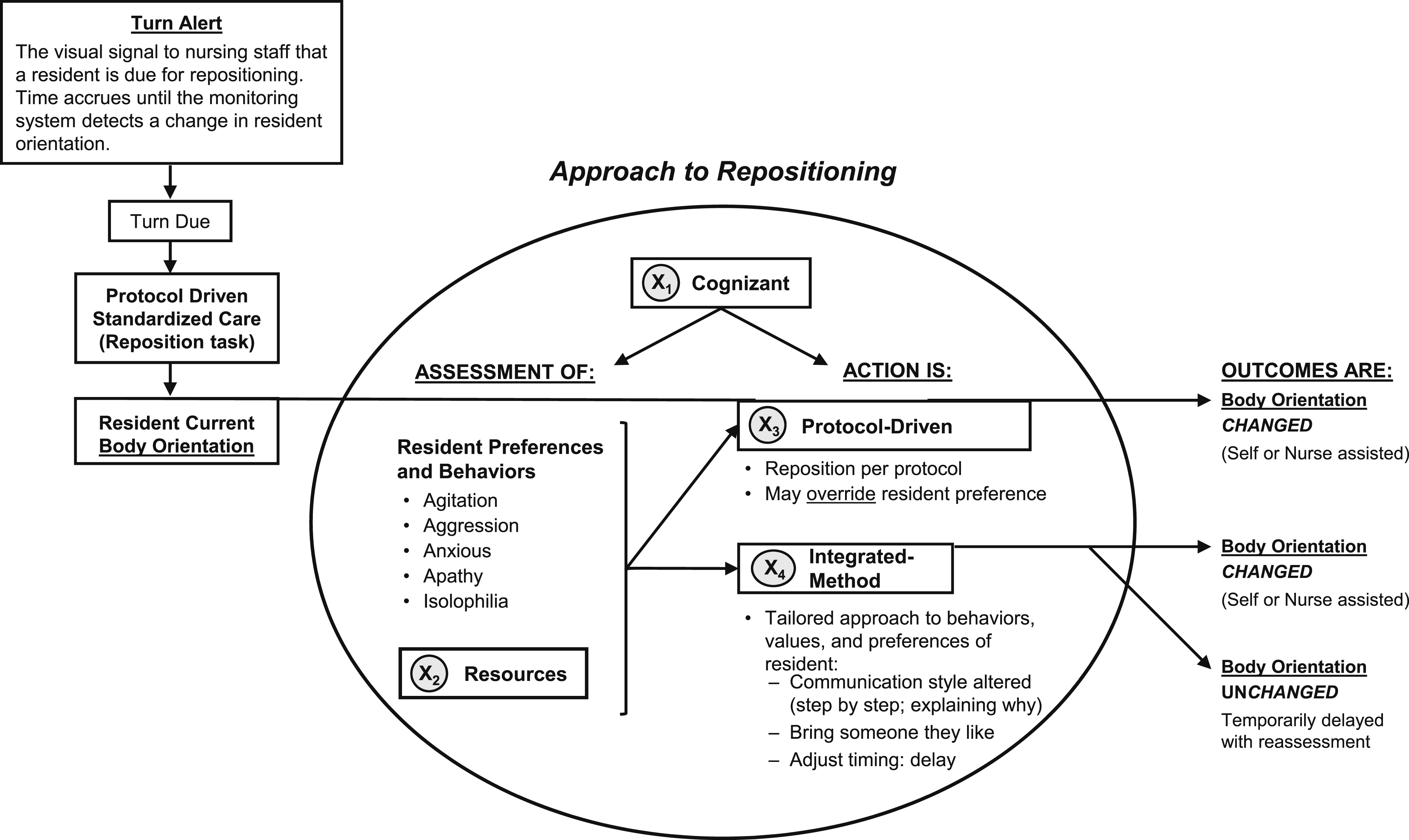
Nursing staff repositioning process for pressure injury prevention.
Discussion
The current study contributes to understanding how staff navigate the tension between institutional repositioning protocols aimed at safety and PrI prevention, and individual resident preferences and behaviors, which may not always align with conventional procedures. Residents living in NHs are all at risk for developing a PrI, and those living with ADRD are at an increased risk. However, little is known about how staff approach evidence-based PrI prevention repositioning protocols.
Resident behaviors
The literature about NH residents living with ADRD describes the difficulties in understanding their environment and the behavioral manifestations of this confusion (Conn & Thorpe, 2007; Cummings, 1997; Cummings et al., 1994; Lai, 2014; Loreck et al., 1994; Melander et al., 2018; Mungas et al., 1989; Ray et al., 1992; Rosen et al., 1994; Tible et al., 2017; Wood et al., 2000). We expected to observe disruptive behaviors during and interfering with, repositioning events. In actuality, few challenging behaviors occurred, and from these data, we speculate the staff’s approach (before, during, and after repositioning) may have prevented or reduced the intensity of common BPSD. For example, staff commented on the importance of reducing behavior antecedents like confusion and overstimulation, which aligns with the current literature strongly supporting a non-pharmacologic approach using simplified communication and environmental modifications (Caspar et al., 2018; de Oliveira et al., 2015). At the same time, staff engagement with residents during repositioning events, including addressing personal care or other unmet needs, likely provided stimulation to counterbalance boredom and withdrawal.
Of the challenging behaviors observed, similarities were noted for both the ADRD and non-ADRD residents (Table 2). Staff approaches to repositioning either group did not differ (Table 3). The most pronounced resident behavior was agitation, occurring in 23% of those living with ADRD and 15% without ADRD (p = 0.24). While agitation is a commonly described behavior for those living with ADRD, it is clear that this is not limited to residents with ADRD and is, in fact, a common human behavior. Furthermore, this similarity suggests that agitation manifests universally as an expression of fear, fatigue, or frustration with unmet needs (real or perceived), which might be more challenging to understand in those residents living with ADRD. Even when challenging resident behaviors were not observed, staff explained the need to reposition in simple positive language and adjusted the environment to provide privacy and reduce unnecessary stimuli. Staff consistently provided encouragement (and/or reassurance) in a calm, soothing manner.
Cognizant
Insights from the focus groups highlight the importance of being cognizant of competing factors in one’s approach to repositioning and reveal staff’s critical reasoning to balance the tension between time-sensitive, institutional protocols, and resident preferences. Staff expressed that they were often successful with repositioning if they were cognizant of competing factors: best evidence (institution-driven, evidence-based protocols), knowing the resident’s preferences based on past interactions, shift report, other forms of team communication/tracking, and applying their cumulative clinical expertise with this population. Consistent with prior literature, focus group participants shared that while there may be institutional repositioning protocols in place, guidance was lacking on how to implement said protocols when residents living with dementia are not cooperative. While staff clearly understood that residents often lacked insight into their own impairment and daily care needs, they were also cognizant of the tension placed on a trust-based, “nurse–patient (resident)” relationship if conflict arises and staff overrode their resident’s repositioning preferences (Molina-Mula & Gallo-Estrada, 2020). Although shared decision-making is an intuitively appealing approach to delivering care, individuals often do not accurately judge their future feelings (preferences), which means that staff approaches for successful repositioning are not simple. Further exploration with our focus groups revealed that staff wanted to honor resident refusal to reposition in situations they empathized with, such as the desire to remain in a comfortable position, sleep uninterrupted, and/or simply not being touched or bothered. In fact, many of the focus group participants believed that many of the ADRD behaviors they encounter result from the sleep disruption caused by longstanding, institutional repositioning protocols (i.e., two-hour intervals, twenty-four-hours-a-day, and seven-days-a-week), which is consistent with concerns noted in the literature (Sharp et al., 2019).
Indeed the needs and treatment of residents living with dementia evolve over time (Gaugler et al., 2014), and our focus group participants also highlighted that residents living with more advanced dementia may not be able to (consistently) express their care-related preferences even during the same day. Accordingly, as resident physical and behavioral assessment fluctuated throughout the day, staff were cognizant that to be successful with repositioning, it may be necessary to seek out additional resources (equipment, supplies, and staff) and information about individual residents prior to each repositioning event.
Resources
Focus group participants spoke about the importance and consistency of resources (i.e., equipment, supplies, and staff) necessary to perform quality repositioning care delivery on all shifts. To safely reposition, nurses shared how gathering other team members, particularly those whom the resident liked/favored, helped encourage cooperation and/or participation in the repositioning event. In contrast, some resources were viewed as potential barriers to repositioning. For example, focus group participants observed that equipment resources used for repositioning (i.e., lifts/lift slings) can cause resident discomfort/pain and can potentially trigger ADRD behaviors during use (i.e., anxiety and agitation) from fear of falling while being hoisted and physically suspended to reposition or transfer to another surface (i.e., bed to chair). The progressive nature of dementia and fear of falling are strongly linked (Soysal et al., 2021); being cognizant of the potential spectrum of reactions from residents during repositioning events reinforces the importance for staff to seek key team members and/or use comforting, verbal assurances while employing repositioning equipment.
Protocol-Driven
Focus group participants described repositioning as a task embedded within institution-specific protocols to be performed in a timely, efficient manner; hence, a protocol-driven approach prioritizes repositioning; thus, staff from these focus groups often found themselves in the unenviable position of overriding resident preferences (protocol-driven care) to avoid being perceived as a poor-performing employee and unable to complete repositioning in a timely, efficient manner as expected. Hence, a protocol-driven approach to ensure that a resident receives repositioning care to prevent PrI (U.S. Centers for Medicare & Medicaid Services, 2017b) makes the goal of person-centered care/shared decision-making (U.S. Centers for Medicare & Medicaid Services, 2017a) a challenge for nursing staff who have to negotiate and effectively navigate the nurse-resident partnership throughout each day (Molina-Mula & Gallo-Estrada, 2020; Sevdalis & Harvey, 2006). While person-centered care is a federal regulatory requirement that defines a resident’s rights to participate in care planning, as well as the right to select or refuse specific treatment options, enforcement of PrI prevention protocols is likely to be prioritized to avoid citation. A federal NH surveyor, for example, does not need to prove that a PrI developed; rather, a NH can be cited if it has been determined that the provider failed to implement interventions to prevent the development of PrI for a resident identified at risk (U.S. Centers for Medicare & Medicaid Services, 2017b). Hence, when the tension between respect for NH resident preferences and the perceived duty to care cannot be initially resolved (and refusal to reposition is not considered a viable option), staff from our focus groups shared how they sought out creative, tailored strategies (e.g., playing music) to achieve care goals considered essential per repositioning protocol. For our focus group participants, use of music was often an effective strategy to persuade residents to reposition for PrI prevention, and is consistent with the literature (Molina-Mula & Gallo-Estrada, 2020; Yap et al., 2016). In addition, findings from this study are consistent with prior literature describing the tension created for nursing staff when a hospitalized patient refuses a prescribed procedure and the expectation is then for the nurse to persuade (and in some instances, coerce) the patient with additional information (Aveyard, 2004). Importantly, while our focus group participants also viewed consent as preferred (even for everyday clinical nursing care), it was not always viewed as essential, and some staff chose to override resident repositioning preferences.
Integrated-Method
Many of the staff delivered an integrated method of care, a repositioning approach seeking balance. While the goal is to achieve regular repositioning for PrI prevention, resident preferences are acknowledged; identified preferences can then be uniquely and creatively addressed by staff. Standard interventions for BPSD involve close contact between individuals living with dementia and their caregivers (Bessey & Walaszek, 2019). Hence, allowing for some flexibility during tight, time-driven protocols during complex activities of daily living promotes a more trusting, therapeutic relationship and may increase the likelihood for greater cooperation in future care-related exchanges.
In considering institutional goals and resident preferences, the staff shared their creative, often dynamic, approach to repositioning as individual resident responses could vary between repositioning events or within an event itself. Staff from this study sought permission to reposition and repeated words slowly and clearly in a step-by-step, comforting fashion. Finally, focus group participants observed that the push for institutional, protocol-driven adherence and efficiency was often counterproductive; consistent with the literature, overriding resident repositioning preferences or rushing them to complete tasks can trigger or exacerbate existing BPSD (Kar, 2009).
Importantly, the staff’s use of an integrative method to repositioning may also help explain why common BPSD described in the literature were observed with relatively low frequency during the observation period. For example, the staff shared how they anticipated challenging behaviors based on previous experience(s), and how they have learned to strategically position themselves out of harm’s way if challenging behaviors like agitation or aggression were demonstrated, allowing them to remain safe and proceed with alternative repositioning approaches. Strategies included honoring time delays, walking away after a repositioning refusal (to avoid or de-escalate challenging behaviors), and gathering of other team members (resources) whom the resident liked/favored to help encourage cooperation and/or participation in the repositioning event (rather than an “extra set of hands” for the physical labor component of repositioning). Knowing the consequences of inconsistent repositioning, staff from these focus groups also provided examples of negotiation strategies they had used in the past with varying levels of success, while simultaneously acknowledging that residents have a right to refuse care. While short time delays for repositioning did occur using an integrated method of care, none of the residents refused repositioning for PrI prevention during the observation period.
Limitations
A limitation of this study was that the focus groups were from only three NHs within the same corporation that volunteered to participate in the parent study. Therefore, they may be systematically different from facilities in other geographic regions or corporations, limiting generalizability. Furthermore, we used a convenience sample of staff available and willing to participate on the day of the scheduled focus groups. Efforts to recruit a diverse group of staff were likely effective, as evidenced by a discussion consisting of negatively toned comments about insufficient resources.
Conclusion
We are the first, to our knowledge, to explore nursing care approaches to repositioning for PrI prevention for NH residents living with or without ADRD. This is important because existing repositioning protocols assume that each repositioning event occurs on time and without incident; how to manage real-life challenges with regard to resident preferences or behaviors is not addressed within task-driven protocols. Hence, identifying an effective, integrated method for PrI repositioning will assist staff in balancing the tension created by these challenges. Knowledge of a practical, effective approach may also inform new staff orientation, continuing education/competency training, and guidance for other protocol-driven tasks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication is supported by the National Institute of Nursing Research of the National Institutes of Health under the Award Number R01NR016001 [ClinicalTrials.gov NCT02996331, First registration (12/19/2016)] and an Administrative Supplement Award Number 3R01-NR016001-04S1. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.